



White Spots, Bumps, and Donor Dots Need Context
White spots after FUE are not one diagnosis. When I see a white mark, I first look at whether it is sitting on top of the skin, raised like a small white bump, or flat inside the healed donor pattern. That detail matters more than the color itself.
The details I need are timing, surface texture, pain, drainage, redness, and location. If the material moves with gentle washing, it is more likely to be loose dry skin, scale, or product residue. If the spot is raised, tender, yellow white, or surrounded by redness, I treat it more like inflammation or possible infection. If the dots are flat, pale, evenly scattered in the donor area, and most visible after a very short haircut, they may be FUE extraction marks. That last group is not an emergency, but it matters for future donor planning and short hair expectations.
White spots after FUE need context
A close phone photo of pale dots can be alarming because several different healing events can look similar on a screen. The same phrase, white spots, may describe dry flakes sitting on top of the scalp, small white headed bumps, pale holes in the donor area, crust remnants, or light marks that become visible when the hair is shaved very short.
One close up photo alone is not enough for this finding. I ask when the operation was done, where the spots are, whether they are flat or raised, whether they wipe away, whether the area hurts, whether there is fluid, and whether the surrounding skin is getting calmer or more inflamed.
When the pattern is in the recipient area during the first weeks, the main concern is often healing surface, washing, residue, folliculitis, or irritation. When the pattern is in the donor area months later and appears as tiny pale dots after a fade, the concern is more about FUE scarring, punch pattern, donor density, and haircut limits. Those are different decisions.
Flakes or product residue
Loose white material that sits on top of the scalp, lifts with gentle washing, or appears after minoxidil, foam, ointment, dry shampoo, or styling products is more often surface material than a scar. It may look patchy under harsh light, especially around short transplanted hairs.
In the early recovery period, washing is often cautious. It is easy to become too gentle with washing because you do not want to disturb the grafts. If loosened skin and product are not removed well, they can dry into a white film or small pieces of scale around hairs. I separate this from deeper problems by asking whether the scalp underneath is calm once the material is softened and cleaned.
If the white material is flaky, itchy, and dry, white flakes on a healing transplant scalp is the more specific surface scaling problem. Here, the decision is broader because the white finding may be residue, bumps, or scar dots.
Do not scratch or pick white material out of the recipient area. Soften it with the washing method your clinic gave you. If it does not lift, or if the skin below looks angry, painful, wet, or increasingly red, send clear photos instead of forcing it off.
White spots that look like folliculitis
Small white bumps around hairs are different from flat pale marks. They may represent folliculitis, irritation around a follicle, ingrown hair activity, or blocked follicles during regrowth. Timing changes the meaning. A white bump around a newly emerging hair during the regrowth phase is not judged the same way as a flat donor dot after a one year fade. The finding matters more when the bumps are tender, itchy, burning, spreading, clustered, or filled with fluid.
Folliculitis is not diagnosed by color alone. I check for a raised bump, a central hair or follicle, surrounding redness, pain, crusting, and whether several spots are appearing together. One or two calm bumps are different from tender clusters, spreading redness, heat, or fluid. Squeezing them can inflame the area and may push bacteria deeper.
If the spots are raised or pus filled, I first think about folliculitis and hair transplant surgery. For the current decision, the important point is that a white head behaves like a skin lesion, not like a permanent FUE scar. It needs hygiene, photo review, and sometimes medical treatment, depending on the pattern.
Do not squeeze white bumps in the recipient area. Do not puncture them with a needle, pull at a central hair with tweezers, or try to drain them at home. If a bump is painful, warm, spreading, or surrounded by worsening redness, ask for review with symptom details. If fever, increasing pain, drainage, or a generally unwell feeling appears, local medical review should not wait for online reassurance.

Texture matters because surface flakes, raised bumps, and flat donor dots are not the same finding.
Warning signs that change the triage
White spots become more concerning when they come with inflammation or symptoms beyond the spot itself. I pay close attention to worsening redness, increasing pain, heat, swelling, cloudy or yellow drainage, crust that becomes thicker instead of loosening, bad smell with wet discharge, fever, chills, or feeling unwell.
Those signs move the question away from cosmetic appearance and toward infection review. Hair transplant surgery still creates many small wounds. Most heal quietly, but a wound that becomes more painful, wetter, hotter, or more inflamed needs direct medical judgment. Patients with diabetes, immune suppression, or recent serious illness should be quicker to seek local medical review when redness, drainage, or fever appears.
Fluid, odor, or spreading redness changes the triage. Yellow fluid after hair transplant, scalp odor during FUE recovery, and infected hair transplant warning signs point to patterns that need faster review than a calm white spot.
Do not let the size of the spot give false reassurance if the surrounding story is getting worse. A tiny white point with calm skin is one thing. A white point with pain, drainage, heat, and fever is a different situation.
White donor dots and FUE scar marks
FUE avoids the long linear scar of FUT, but it is not scarless. Each extracted follicular unit leaves a small round wound, and in some patients those healed points become hypopigmented donor dots. In many patients the marks are difficult to see when the hair has a little length. In some patients, especially with short fades, dark hair against lighter skin, darker skin that contrasts with pale scar tissue, larger punch size, dense extraction, or repeated sessions, the dots can be visible.
In the donor scar pattern, the dots are flat. They do not wipe away. They do not behave like flakes. They are often more visible when the donor area is shaved close or when the lighting hits from the side. You may first notice them months or years later because the hair is cut shorter than before.
Flat pale donor dots are a healing and scar contrast issue, not a surface problem that can be scrubbed away. Creams, oils, and aggressive exfoliation will not remove an extraction mark. Even experimental donor scar creams, including topical metformin after FUE, still need evidence, timing, and skin review before they are used. The wrong product may only irritate the skin and make the area harder to judge.
FUE marketing deserves caution when a clinic calls it invisible or scar free. Donor marks can often be minimized by planning, punch selection, extraction spacing, graft number discipline, and good healing, but they cannot be promised away.
Before surgery, I connect short hair expectations with FUE punch size and donor scarring and short hair after FUE donor scars. Someone who wants a skin fade forever needs a different consent conversation from someone who always keeps the donor area longer.
Use the 8 white spot review slides below to separate surface flakes, raised bumps, flat donor dots, timing, warning signs, short hair visibility, and the photo details needed for a useful review. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.



Separating scar dots from overharvesting
White dot scarring and overharvesting are related but not identical. A donor area can show tiny pale extraction points while the overall hair coverage still looks acceptable. Overharvesting means the donor has also lost too much visual density, often in a patchy or see through pattern.
I judge this by stepping back from the macro photo. Close up images can exaggerate every mark. A proper review needs normal distance photos, side and back views, the haircut length, lighting information, and the number of grafts removed. I want to know whether the donor looks evenly reduced or locally emptied. For a future procedure, I also look at whether there is enough untouched donor between old extraction marks, not only whether the white dots can be hidden by a longer haircut.
A dot pattern is a scar pattern. A thin or patchy donor is a donor management problem. Sometimes both exist. When both are present, the future plan becomes more limited because there may be less safe donor reserve for correction, thickening, or a second procedure.
Broad thinning, patchiness, or a window like donor pattern belongs under donor area overharvesting. This white spot discussion is narrower because it helps you decide what the visible pale points might represent.
White spots in the recipient area and graft loss
Not by themselves. A white spot in the recipient area can be dry scale, a tiny pimple, product residue, a crust remnant, or light reflecting from short hair and healing skin. Graft loss is usually judged by the event history, not by a pale point alone. The useful details are whether a graft came out with bleeding, whether there was trauma or forceful picking, and whether infection followed.
It is very common to inspect the recipient area at close range after scabs come off. The scalp can look uneven, pale in some areas, pink in others, and empty during the shedding stage. That uneven look does not prove that grafts failed. It does mean the photos should be taken consistently, not under harsh bathroom lighting one day and soft daylight the next.
If the pale point sits among redness, scabs, and pimples after hair transplant, judge it as part of the wider inflammation pattern. Clear bleeding belongs in a different triage path because after transplant bleeding changes how urgently the area should be reviewed. A white spot without bleeding, on its own, is not enough to diagnose lost grafts.
Photos that help the clinic judge white spots
One extreme close up is rarely enough. Send one normal distance photo of the whole recipient or donor area, one closer photo, and one angled photo under natural light. If the spots change after gentle washing, send before and after photos rather than only the worst moment. If the spots are in the donor area, include the haircut length. If they are in the recipient area, include the day after surgery and whether scabs have already come off.
Also describe whether the spots are flat or raised, whether they wipe away, whether they are painful, whether there is drainage, whether the number is increasing, and whether the surrounding skin is red, hot, or swollen. Mention recent minoxidil, ketoconazole, oil, ointment, dye, dry shampoo, fibers, styling product, scratching, picking, pressure during sleep, a tight hat, or a very short fade.
I cannot judge this safely from a cropped photo with no timeline. The timeline turns the same white spot into a different diagnosis. Day 8 residue, week 6 folliculitis, and one year donor scar dots are not the same problem.
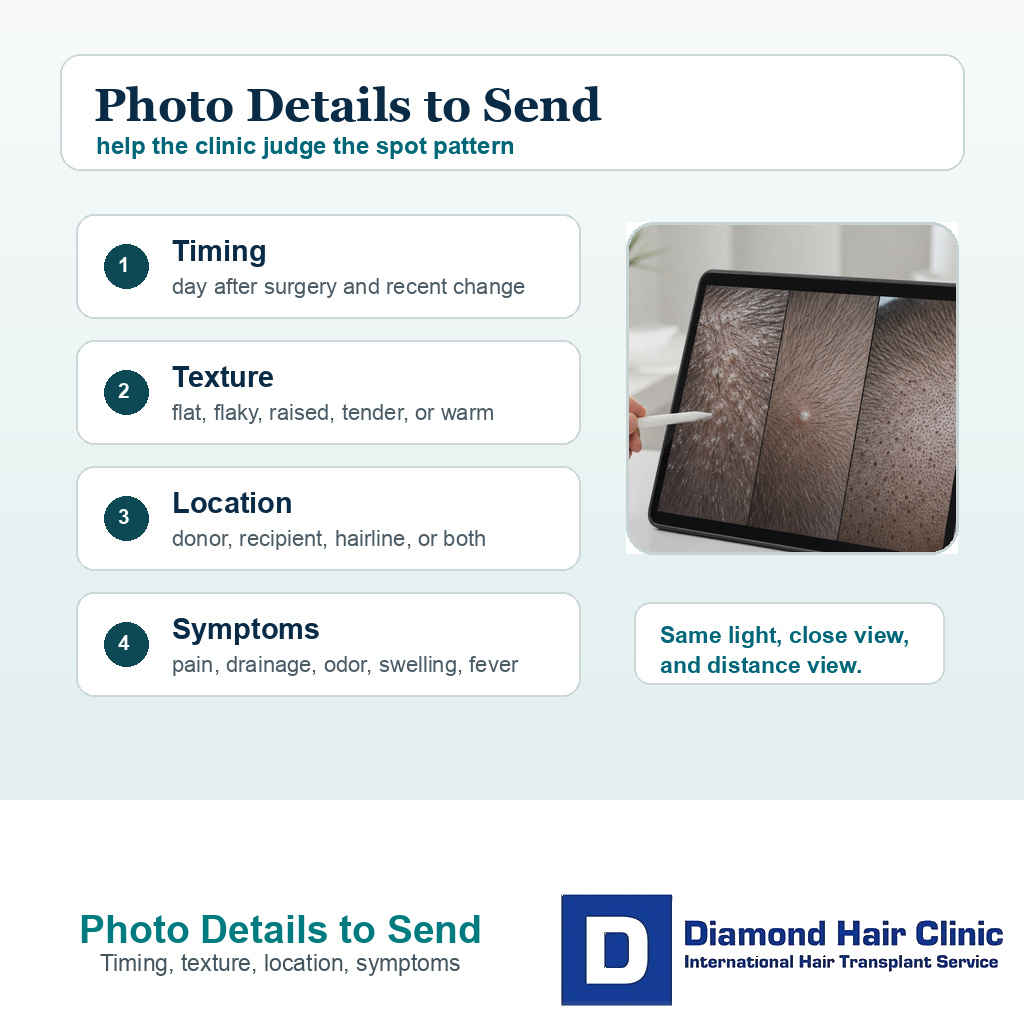
Good photos show timing, texture, location, and symptoms so the clinic can judge the pattern.
Before putting products on white spots
Do not cover the problem before it is understood. Heavy oils, thick ointments, cosmetic concealers, fibers, gels, and aggressive dandruff treatments can make the surface harder to judge. Do not apply alcohol, hydrogen peroxide, acids, retinoids, bleaching creams, steroid creams, or antibiotic creams to transplant wounds unless a clinician specifically tells you to. Some products also irritate follicles or trap residue around healing skin.
Photograph the spots before covering them, because products can hide the pattern or irritate the skin.
If the issue appears early, follow your clinic’s washing protocol. If the scalp is already healed enough for normal washing but flakes continue, the timing of washing after hair transplant and ketoconazole shampoo after hair transplant depends on the operation date, skin condition, and clinic instructions.
If minoxidil residue is suspected, document what the surface looks like before changing treatment. Minoxidil after hair transplant can be useful, but the scalp must be ready for it and the product should not leave a film that makes the skin harder to judge. I handle that as a timing decision first.
Some liquid and foam products leave a white cast or crusty film, especially when applied too much or before the scalp is ready. The answer may be a timing change, product adjustment, or temporary pause, but that depends on the clinical context and the medication plan.
White dots after a fade
This is a common long term discovery. The donor area may look acceptable with a few millimeters of hair, then dotted after a skin fade. That does not mean the surgery suddenly caused a new problem. It may mean the haircut removed the camouflage that was hiding tiny extraction scars.
A very short fade can reveal donor dots that were hidden by a few millimeters of hair.
Before FUE, I discuss how short you want to cut the back and sides in the future. Some people accept a grade 2 or 3 guard. Others want a zero fade or fully shaved head. The shorter the haircut, the less margin there is for donor marks, contrast, and extraction pattern.
If white dots are already visible after a fade, try different guard lengths, take photos in normal daylight, and avoid judging the donor only from a flash close up. Do not tan or burn the scalp to hide contrast. Sun exposure can make color difference and irritation harder to judge. Scalp micropigmentation, beard or body hair repair, and redistribution have roles in selected cases, but they cannot fully undo a poorly spent donor area. The better protection is conservative extraction before the first surgery.
I judge white spots as a surgeon
I start by identifying what the white spot is physically doing. Surface material can be washed. A pustule can inflame. A pale scar dot can persist. A donor area can look dotted but still acceptable, or dotted and depleted. These differences matter because each one leads to a different action.
In a recent recovery, my priority is to avoid picking, squeezing, or hiding the finding with products before it is reviewed. In a long term review, donor clarity matters because FUE can be excellent, but short hair may reveal marks that longer hair used to hide, especially after large or repeated sessions.
For a useful review, include timing, symptoms, products used, haircut length, and whether the spots are raised or flat. A calm flat dot is often monitored. A painful, wet, spreading, or fever linked spot needs faster medical review. A visible donor dot pattern needs clear planning for haircut choices, donor reserve, and whether another extraction session would make the pattern harder to camouflage.
What I need to know is whether the mark is movable, raised, or flat, and whether the surrounding story is getting better or worse. That is how I decide between washing guidance, photo review, medical treatment, donor planning, or monitoring.