Bleeding After Surgery and Graft Safety
A small amount of dried blood or brief oozing can happen after a hair transplant, especially in the first day or two. The first step is not to wipe, test, or keep checking the area. Protect the grafts, keep your head elevated, use gentle pressure only where your clinic has instructed, and message the clinic if bleeding keeps soaking gauze, restarts repeatedly, follows trauma during the car ride after FUE, or comes with increasing pain, discharge, fever, dizziness, or an open looking area. On night one, pair bleeding judgment with the first night graft safety plan so position, photos, and clinic messaging stay controlled.
I take bleeding seriously because it can mean two very different things. Sometimes it is only surface healing. Sometimes it is a sign that the scalp has been rubbed, picked, bumped, affected by medication, or is not settling as expected. I do not want you guessing from one close photo. If aspirin is part of the story, the timing and reason should be reviewed through aspirin and hair transplant surgery.
Bleeding can be a small recovery issue
A few dry blood spots around grafts, a light stain on gauze, or a little pink fluid during the first wash can be part of early healing. If the stain is straw yellow rather than red or pink, yellow scalp fluid after FUE needs a different check because drainage, bruising color, product residue, and infection do not behave the same way. The scalp has thousands of tiny surgical openings. Some dried blood and crusting around them is expected, especially when the operation has just finished.
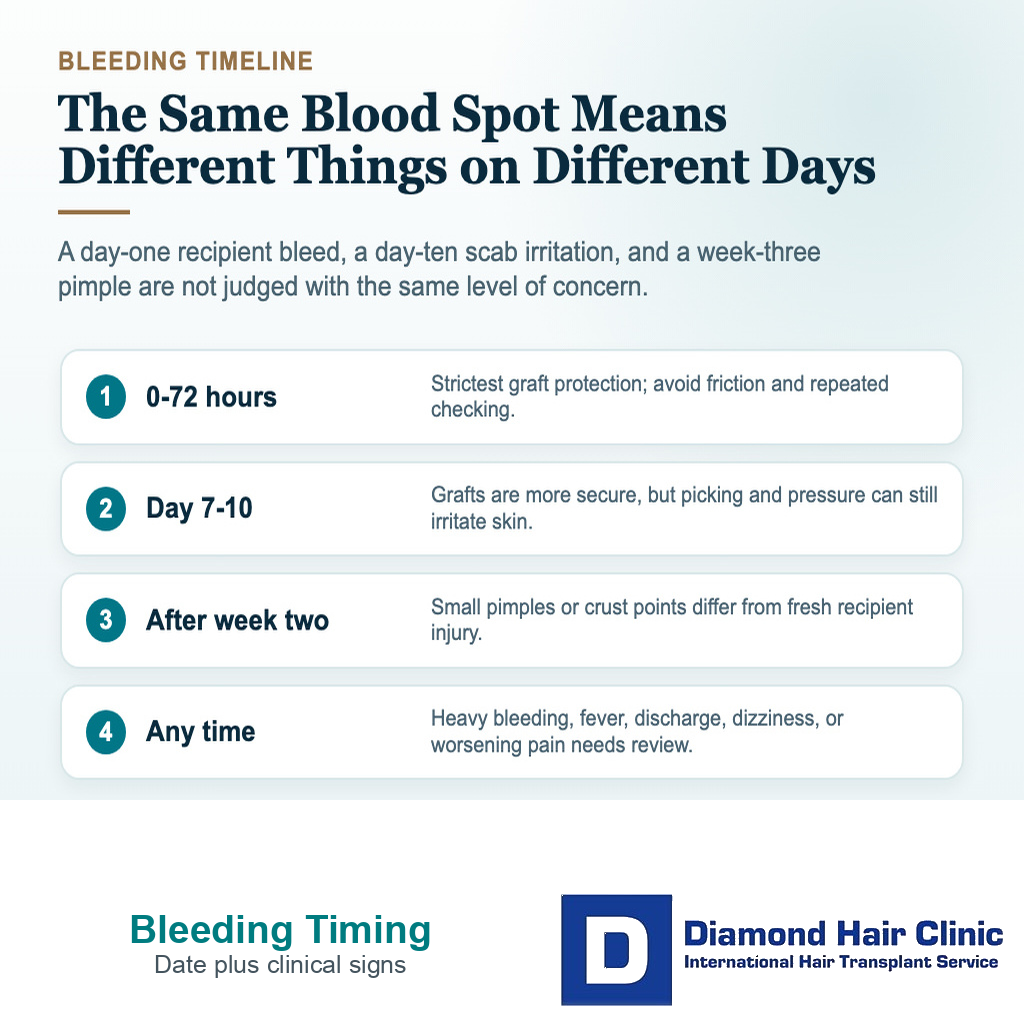
The pattern matters more than one photo. If the amount is small, stops quickly, does not return, and the skin around it is gradually settling, I usually treat it differently from bleeding that keeps coming back or spreads into a larger wet area. The same distinction helps when judging redness, scabs, or pimples during the first weeks.
Small dried blood is not the same as active bleeding. A dark crust from the procedure can look dramatic under harsh light, but it may simply be a clot that is drying. Active bleeding is wet, fresh, and usually changes the surface while you are watching it. The same separation matters with black eye bruising after a hair transplant, where color under the skin is not the same as fresh blood coming out.
The first minute should be calm and simple
First, stop touching the area. Sit upright. Keep the recipient area away from towels, pillows, and fingers. Do not rub the scalp to see whether more blood appears. Do not scrape away crusts to check the grafts. That testing behavior can create more irritation than the original blood spot. The same rule applies after accidental sleep contact, where I explain how to check slept on grafts without testing them.
If your clinic gave a specific pressure instruction, follow that instruction. In general, pressure should be gentle, clean, and controlled. When pressure is instructed, hold the folded gauze still for the full interval the clinic gave instead of lifting it every minute. Pressure on the donor area is different from pressure on the recipient area where grafts were placed. When the source is not clear, send a clear photo before pressing on the grafted zone.
Do not wipe back and forth across the grafts. Wiping creates friction. Friction is exactly what the first days are trying to avoid. A clean folded gauze pad held still is very different from rubbing with tissue, cotton, a towel, or a shirt sleeve.

A clean gauze pad held still is different from wiping across the grafted area.
Bleeding that does not stop needs clinic contact
If bleeding continues despite the first step your clinic instructed, do not keep lifting the gauze every few seconds to check it. Keep the area still, keep your head elevated, and send a clear photo with the exact time the bleeding started. If gauze becomes wet, place a new clean layer over it rather than peeling away material that may be stuck to crusts or grafts. Repeated checking, rubbing, or changing tissues can disturb the surface more than the bleeding itself.
If blood is soaking through clean gauze, flowing rather than spotting, returning again and again, or you feel faint, confused, weak, short of breath, or medically unwell, this is no longer only a graft anxiety question. Urgent local medical help should come before waiting for an online photo review. If you are alone after travel, call a companion, hotel staff, or local emergency service instead of trying to drive yourself. The clinic can still guide the transplant side, but active bleeding and systemic symptoms need direct medical judgment.
Bleeding does not always mean a graft was lost
Bleeding alone does not prove graft loss. I judge the risk by timing, force, location, whether there is visible tissue, and whether the skin now looks open compared with the surrounding grafts. A blood clot around the grafts on day one or day two is not the same as a graft being pulled out.
A true graft loss event is more concerning when it happens early and is associated with fresh pinpoint bleeding, a small soft tissue piece, or a wet hole where a graft was placed. Many patients instead see a hair shaft trapped in a crust. That can be frightening, but a dry scab with a hair inside it is often not a lost graft.
Fresh bleeding plus visible tissue should be assessed carefully. A dry flake, a short shed hair, or old brown crust usually needs a careful interpretation. If you see a soft tissue piece or a possible graft, do not push it back into the opening or pull at nearby crusts. Photograph it once, keep the area still, and avoid handling nearby crusts again.
Donor area bleeding is reviewed differently
Donor area bleeding is judged differently from recipient area bleeding. The donor area does not contain newly placed grafts, but it still contains many small extraction wounds. A little early oozing can happen. Repeated bleeding, late bleeding, worsening pain, spreading redness, discharge, or a spot that keeps opening is not something I dismiss as ordinary recovery.

You may wake up with blood on a pillow and assume the transplant is ruined. If the blood came from the donor area, the recipient grafts may be safe, but the donor skin still needs respect. Friction from a pillow, scratching, pimples, or crusts can reopen small points. If blood appears night after night, the clinic should know.
The donor area also tells me about the quality of the healing environment. Bleeding after too much touching, heavy sweating, dirty pillow contact, or aggressive scab removal is different from a settled donor area with one small dry stain. Do not cover recurring donor bleeding with hair fibers, concealer, or a tight hat just to hide it.
Bleeding signs the clinic should review urgently
Prompt review is needed if bleeding does not stop with the instructed first step, keeps soaking clean gauze, restarts several times, follows a clear bump or scratch, or appears with a wet open area in the recipient zone. The same urgency applies if you feel faint, confused, very weak, short of breath, or unable to keep fluids down. If the bleeding is heavy or you feel medically unwell, urgent local medical help comes before waiting for a photo review.
Tell the clinic about increasing pain, hot spreading redness, pus, bad smell, fever, black or grey tissue, or swelling that is getting worse instead of settling, including a swollen neck lymph node after FUE. Those signs are not only cosmetic. They can point to infection, tissue irritation, trauma, or a wound that needs direct medical review.
Bleeding that keeps returning should not be judged like a photo comparison problem. The clinic needs a pattern. Timing, amount, medication history, and photos all matter. That is safer than asking strangers to judge one close image. It belongs inside a clear hair transplant follow up plan, not a casual message thread.
Protect the grafts, document the pattern, and send the clinic a clear update when bleeding persists or symptoms worsen.
These 8 bleeding and graft safety slides separate stopped staining, returning bleeding, donor versus recipient source, trauma context, warning signs, and the photo details that help the clinic. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.