



Receding Hairline Stages and Treatment Options
A receding hairline means the front edge of the hairline is moving backward or becoming visibly weaker, usually first at the temples. In men, the most common reason is androgenetic alopecia, also called male pattern hair loss. But I want to be clear from the beginning. Not every high forehead, temple shape, or uneven front line is true balding.
A patient with a natural widow’s peak needs this distinction because the center may be stable while the temple corners are changing.
A mature hairline, stress shedding, traction from hairstyles, inflammation, thyroid disease, low iron, and some scarring conditions such as frontal fibrosing alopecia can all change the way the frontal hairline looks. A naturally high forehead is also different from a hairline that is actively moving backward. If the main uncertainty is normal maturation or active loss, the separate mature hairline or receding hairline guide shows how I check that before FUE.
Clinically, I first separate slow pattern recession from changes that need diagnosis. If the change is slow, symmetrical, and supported by family history, it is often pattern hair loss. If the change is sudden, patchy, painful, itchy, red, scaly, or associated with heavy shedding, it needs diagnosis before anyone talks about graft numbers.
In short, a receding hairline should first be diagnosed before treatment is chosen. If the recession is early and active, medication or monitoring may be the first step. If the temples are clearly lost and the donor area is strong enough, a hair transplant may rebuild the hairline. But the safest result depends on age, future hair loss risk, donor capacity, and natural hairline design.
Many patients are not told this clearly enough. A receding hairline is not only a missing corner. It is a forecasting problem. It tells me something about what may happen behind the hairline later. If the crown is beginning to thin, if the mid scalp is weaker than it looks, or if the donor area is limited, the hairline plan must change.
Before I talk about treatment, I want to understand whether the hairline is truly changing, why it is changing, and which treatment would still make sense if we look at the same patient five or ten years later.
First steps when your hairline is receding
If you think your hairline is receding, the first step is not choosing a clinic or asking for a graft number. The first step is understanding whether the hairline is truly moving, why it is moving, and whether the surrounding hair is also becoming weaker.
I want to know the patient’s age, family history, speed of change, old photos, crown condition, mid scalp density, donor quality, and whether there are symptoms such as itching, burning, redness, scaling, or sudden shedding.
A close up temple photo can show the visible concern, but it cannot show the whole risk. A single close up image is too narrow for safe hairline planning. A proper plan needs the front, temples, crown, donor area, hair caliber, age, family pattern, and speed of progression.
Consultations that begin with a package number are a warning sign for me. A real plan should begin with the cause of the recession, the strength of the donor area, future risk, and a design that would still look natural as the patient gets older.
Watch, treat, or consider surgery based on risk
Most patients want to know whether they should watch the hairline, treat it medically, or consider surgery. In real consultations, I separate receding hairline patients into four practical groups.

When the change is mild, the hairline edge is still strong, old photos look stable, the crown is not thinning, and there are no scalp symptoms, watching and photographing the hairline can be reasonable. Daily mirror checking usually creates noise. Consistent monthly photos, taken in the same conditions, are more useful than panic.
When the hairline change is sudden, patchy, painful, itchy, red, scaly, shiny, or associated with eyebrow thinning, heavy shedding, or female frontal recession, diagnosis should come first. These signs can point away from simple male pattern hair loss.
When miniaturized hairs are still present, the patient is young, the recession is actively changing, or the family history suggests more advanced future hair loss, stabilization may be the better first step. Treatment should protect the hair behind the hairline, not only improve the front edge today.
Hairline transplant planning becomes more reasonable when the temple loss is clear, the pattern is stable enough, the donor area is strong enough, there is no active scalp disease, and the patient accepts a natural adult hairline rather than the lowest possible line.
This framework is not a replacement for examination, but it helps patients think more clearly. A receding hairline should not immediately lead to surgery. It should lead to the correct category of decision.




Slide 1 of 4. Pattern evidence before deciding between monitoring, treatment, and surgery.

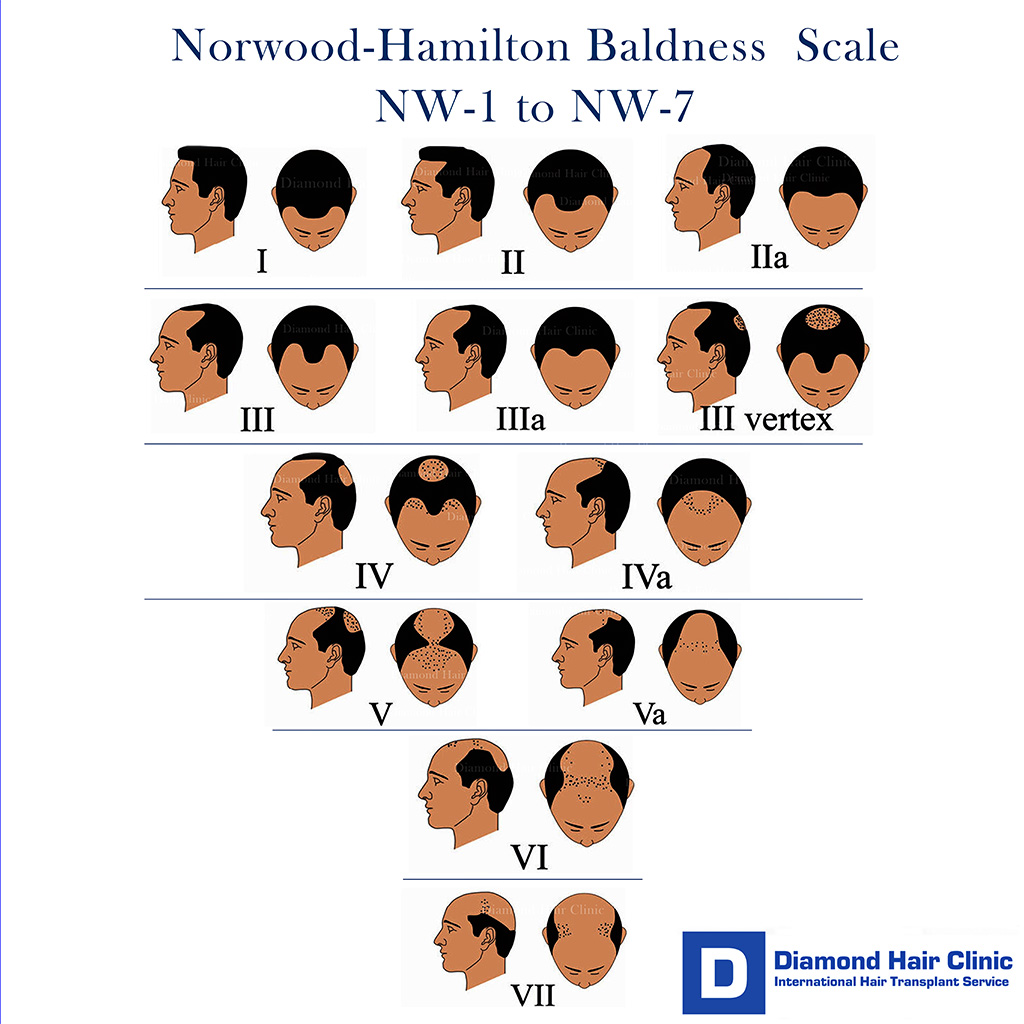
I use the Norwood scale
Norwood 1 and Norwood 2 patterns can be normal or early. Norwood 3 usually means more definite recession. Higher Norwood patterns often include broader front, mid scalp, and crown involvement. Still, the number alone does not decide treatment.
A Norwood 3 patient with strong donor hair, stable loss, and realistic expectations may be a good candidate. A younger patient with diffuse thinning and rapid progression may need stabilization first, even if the visible recession looks smaller.
The Norwood scale does not show donor quality, hair caliber, scalp contrast, miniaturization, medical tolerance, or emotional readiness. Those details often matter more than the label.
Some patients should wait before hairline surgery
Some patients are better served by waiting. This includes patients with very early or uncertain recession, rapid ongoing loss, diffuse thinning behind the hairline, unstable medical causes, active scalp inflammation, weak donor area, or expectations that no surgery can satisfy safely.
Waiting does not mean doing nothing. It may mean tracking the pattern, treating inflammation, correcting a deficiency, using medication if appropriate, and reassessing with better information. Surgery is strongest when the diagnosis and long term plan are clear.
I know waiting can be frustrating, especially when the hairline is the first thing a patient sees in every photo. But sometimes waiting 6 to 12 months gives a much safer answer. It can show whether medication is helping, whether shedding recovers, and whether the recession is truly progressing.
There is also an emotional side. If the decision is driven by panic, comparison, or pressure after seeing aggressive transformations online, more time is often the safer choice. A hair transplant should be a clear decision, not a reaction to anxiety.
Age changes the hairline plan
Age changes the risk. A patient in the early twenties with temple recession may still be at the beginning of a much larger pattern. If I rebuild a low hairline too early and the crown later opens, the patient can be left with an isolated front and not enough donor reserve to manage the rest well.
Patients in their twenties
In the twenties, I am cautious. My conclusion is not that every young patient is refused. It means the diagnosis, family history, donor area, medication plan, and expectations must be taken seriously. If the loss is active and the future pattern is unclear, monitoring and medical treatment may be safer than surgery.
In young patients, the weaker point is not only doing surgery too early. The bigger mistake is designing the hairline as if the final hair loss pattern is already known. At 22 or 24, the front may be the only visible problem, while the crown and mid scalp may declare themselves later. The stronger plan is one that can survive future thinning, not one that only looks exciting on the day of the drawing.
Patients in their thirties
In the thirties, the pattern is often clearer. A transplant may be more reasonable if recession is stable enough and the donor area is good. But I still do not design a hairline as if the patient will never lose more hair. The crown and mid scalp must be checked carefully.
Many patients in this age group are good candidates, but the plan still has to be realistic. A natural adult hairline usually ages better than an aggressive one.
Patients over forty
After forty, the pattern is often easier to read, but donor management still matters. Some patients have strong donor hair and mainly frontal recession. Others have wider thinning and need a more conservative plan. A good design frames the face naturally without pretending the donor area is unlimited.
Real patients need different plans
Two patients can have similar looking temples and need very different plans.
A 22 year old with active temple recession, miniaturized hairs behind the hairline, and a strong family history of advanced baldness should not be treated like a finished pattern. In this patient, I usually think first about diagnosis, stabilization, and time. If surgery is done too aggressively, the result may look good for a short period and then become difficult to manage as the surrounding hair continues to thin.
A 38 year old with stable temple recession, strong donor hair, no major crown thinning, and realistic expectations may be a very different case. If the hairline design is mature and the graft number is calculated carefully, hairline restoration may be more reasonable.
There is no single hairline formula. The correct plan depends on the patient in front of me, not only the shape of the corners.
Hairline or crown priority depends on donor supply
This depends on what bothers the patient and what the donor area can support. The hairline usually gives the biggest visual change because it frames the face. The crown can require many grafts and still look less dense because of the spiral pattern and wider surface area.
When both the hairline and crown are involved, I discuss the tradeoff before choosing the surgery order. Some patients should prioritize the front first. Some should wait until the pattern is more stable. Some need a staged plan. Whether to treat the hairline or crown first is a donor supply decision, not just a cosmetic preference.
The risky decision is trying to solve everything in one session when the donor area cannot truly support it. That can make the result look thin everywhere. A focused frontal plan may create a stronger visible change than spreading grafts too widely.
Typical graft ranges for a receding hairline
Patients often ask for one number, but a receding hairline does not have one fixed graft count. A small temple corner correction may be around 1,000 to 1,800 grafts. A moderate frontal hairline reconstruction may be around 1,800 to 2,500 grafts. A larger frontal third restoration may require 2,500 to 3,500 grafts or more.
These numbers are not promises. They are only a practical way to understand scale. In my planning, I first decide whether the proposed hairline belongs to the face and whether the donor area can safely support it. Only after that do I calculate the graft number.
The opposite approach is risky. A clinic chooses an impressive number first, lowers the hairline too much, and then spends donor hair without thinking about the next ten or twenty years. For a receding hairline, the right number is the number that supports a natural design without damaging the future plan.
Transition zone matters in hairline design
The front edge should not look like a wall. In natural hairlines, there is a soft transition before the denser hair begins. I use finer single hair grafts at the very front and avoid placing the same density and thickness everywhere.
A hairline that is too equal can look artificial even if many grafts grow. The eye catches regularity, rows, and thick grafts at the very front. The patient may not know exactly why the result looks wrong, but he feels that the hairline does not belong to the face.
A natural result depends on design, graft selection, density transition, direction, angle, and incision distribution. A good hairline cannot be judged only by the number of grafts used. This point belongs in the broader discussion of natural hair transplant result standards.
Donor management protects future options
The donor area is limited. Once grafts are removed, they are no longer available for future surgery. I do not plan a hairline as if the patient has unlimited donor supply.
In a young patient with early recession, the better answer may be to wait, stabilize, or choose a modest design. In a patient with advanced loss, the better answer may be to prioritize the front and accept that crown coverage has limits. Good donor management is how a result stays natural over time.
Overharvesting the donor area to chase density at the front can create a second problem. The front may look better for a while, but the back and sides can look thinned, patchy, or depleted. A good hairline result should not come at the cost of an obviously damaged donor area.
If a donor area is weak, the responsible answer may be a smaller plan, a staged plan, or no surgery. For weak donor area and hair transplant, donor quality can change the entire treatment strategy.
Temple points and low hairlines
The temple points can change how the whole hairline is read. If the front hairline is lowered too much while the temple points remain weak or receded, the result can look disconnected. In other patients, rebuilding the temple points too aggressively can look sharp, artificial, or too youthful for the face.
I plan the front hairline and temples together. Temple point hair transplant is part of that balance, and low and flat hairlines show why a lower line is not necessarily a better line.
Some patients want the corners closed completely because they believe that any visible temple recession is a defect. I do not agree with that approach. A slight adult recession can look natural. A forced square frame can look operated.
Poor design makes a hairline transplant look unnatural
An unnatural hairline is usually not caused by one single mistake. It can come from a line that is too low, too straight, too dense at the very front, too regular, or placed with the wrong angles. It can also happen when thick multi hair grafts are used at the front edge instead of fine single hair grafts.
The result has to survive real life. It should look natural when the hair is wet, when the patient is under bright light, when the hair is short, and when the patient ages. Small design decisions matter because patients live with the result in ordinary light, not only in after photos.
Repairing a bad hairline is harder than doing it correctly the first time. A pluggy or overly straight front may need graft removal, redistribution, camouflage, or staged repair. That costs time, donor hair, and emotional energy. The better decision is to avoid the mistake at the first surgery.
A thin looking result can also come from poor planning even when a large number of grafts was used. If the design is too wide, the density is spread too thin, the donor is overused, or the hairline is lowered beyond what the donor can support, the patient may end up with a result that is technically grown but visually disappointing. The same problem from the density side belongs in why some hair transplant results look thin.
Technique choice for a receding hairline
Technique matters, but it should not be used as a marketing shortcut. FUE and DHI are methods of handling and placing follicular units. Neither automatically guarantees a natural hairline. The design, graft selection, recipient area incisions, density planning, and surgical judgment matter more than the label.
For the front edge, I want fine single hair grafts, natural direction, careful angle, and a soft transition. The clinic page comparing DHI and FUE explains the technique difference, but you should not choose a clinic only because one method sounds more modern.
Modern FUE hair transplant can be an excellent method for frontal restoration when the diagnosis, donor management, extraction pattern, and recipient area planning are done properly. At Diamond Hair Clinic, I use Sapphire FUE because I value controlled recipient area incision creation, natural angle, and careful distribution. But the blade or method is not a magic answer. The surgical judgment behind it matters more than the label.
Cost depends on diagnosis and design
Cost depends on the diagnosis and the plan. Early medical treatment is different from a transplant. A small temple refinement is different from rebuilding a full frontal third. What concerns me is choosing graft numbers from a package before the hairline has been designed properly.
For surgery, graft number should follow the design, not the other way around. A careful 1,800 graft hairline can be much better than a careless 3,500 graft promise. The right number depends on the size of the recipient area, hair caliber, donor strength, density goal, and how much reserve must be protected for the future.
Package style graft promises concern me because the number can distract from design. A large number may sound attractive, but if the hairline is too low, too dense in the wrong place, or planned without future loss in mind, the patient may pay later with donor depletion or repair surgery.
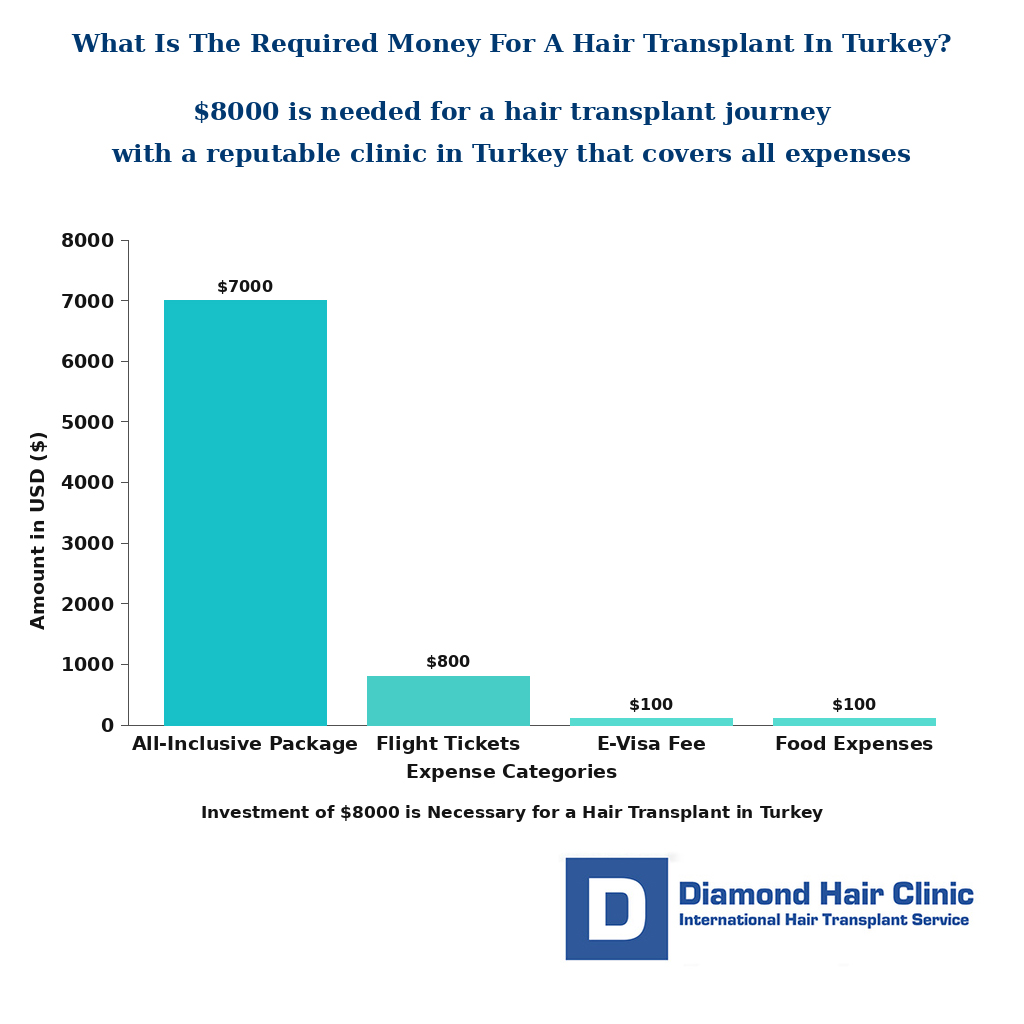
If you are comparing clinics in Turkey, hair transplant cost in Turkey needs judgment together with surgeon involvement, donor management, and the real quality of planning.
Doing nothing can make recession harder to plan later
Doing nothing may be reasonable if the hairline is mature, stable, and not bothering the patient. It may be risky if the hairline is actively miniaturizing and the patient wants to preserve as much native hair as possible. The pattern decides how much waiting costs.
If it is genetic pattern hair loss and no treatment is used, progression may continue. The speed is different for each patient. Some lose slowly over decades. Some change quickly in a few years. Photo tracking and follow up matter because the pattern becomes clearer over time.
Treatment is not necessary for every patient. The point is to understand what waiting means in that specific case. Waiting with a plan is different from ignoring the problem because the decision feels uncomfortable.
Questions to ask before treatment
Before medication, ask what the expected benefit is, how long it takes to judge, what side effects matter, and what happens if you stop. Before surgery, ask why the proposed hairline height is right for your face, how the donor area was assessed, what happens if future hair loss continues, and whether the clinic is planning only the front or the whole scalp.
After a proper consultation, you should feel clearer, not only excited, and understand the reason behind the plan. If the only explanation is a large graft number or a discounted package, the conversation is incomplete.
I warn patients about red flags of hair mills for exactly this reason. A low price, a large graft number, and a very low hairline drawing can feel convincing at the beginning. But the detail that matters is whether the plan protects the donor area and still looks natural in the future.
If you are not sure whether you are a safe surgical candidate yet, whether you are really a good candidate for a hair transplant can help you think through the decision more carefully.
My approach at Diamond Hair Clinic
At Diamond Hair Clinic, I do not look at a receding hairline as an isolated line on the forehead. I look at the whole scalp, the donor area, the crown, the mid scalp, the temple points, the patient’s age, family history, and long term risk.
Some patients are good candidates for hairline restoration. Some need medication or monitoring first. Some should not have surgery yet. This needs to be clear before surgery because a hairline transplant uses permanent donor hair and the decision cannot be treated casually.
If surgery is the right choice, I am not trying to create the lowest possible hairline. The better goal is a hairline that frames the face naturally, uses grafts intelligently, and still makes sense as the patient gets older.
The one patient per day model matters here because rebuilding a receding hairline may look like a small operation from outside, but the design controls the whole result. The angle, direction, density transition, temple balance, and donor planning all decide whether the patient looks natural or operated on.
A good hairline should belong to the patient’s face and protect his future options.
When the hairline pattern is unclear, you can contact Diamond Hair Clinic and share clear photos. A proper consultation is not just about whether a transplant is possible. The deciding issue is whether it is the right decision for your hairline now and for the years ahead.