Weak Donor Area Hair Transplant Planning
A hair transplant can sometimes be possible with a weak donor area, but the decision depends on what the donor can safely give. If the hair at the back and sides is limited, I first ask whether a modest, focused improvement can be done without creating a second problem in the donor area. If the reserve is truly poor, surgery may need to be smaller, staged, medically delayed, or refused. This is especially important when a patient wants a transplant to replace a hair system. A limited donor reserve does not by itself mean no surgery, but it always means no careless surgery. That judgment is the core of cases where I say no to a hair transplant.
The same donor first logic applies when assessing a hair transplant after 40 or 50, because age, medical stability, and coverage goals can make a limited donor area even less forgiving.
I treat this as a serious lifetime graft decision because hair removed from the donor area cannot simply be put back. If it is used badly, you do not only risk a thin result on top. You can also be left with the back and sides looking depleted, which is much harder to hide and much harder to repair. That point is central to why donor hair does not grow back after FUE, because a weak donor becomes riskier when regrowth is assumed. For that reason, verteporfin donor regrowth planning should not make a weak donor plan more aggressive before the evidence is reliable.
I do not start by asking how many grafts we can take. I ask what the donor can give safely, what the recipient area really needs, and whether the plan will still make sense years later. This matters when someone has been offered 5,000 grafts in one operation, because the same number can be sensible for one person and too aggressive for another. When camouflage is part of the plan, scalp micropigmentation after hair transplant still depends on stable skin and conservative donor judgment. The same restraint is central to Norwood 4 or 5 hair transplant planning, where coverage goals can quickly outrun donor reserve. The same restraint applies to donor SMP camouflage, because pigment should not hide a donor reserve problem.
Checks before calling a donor safe
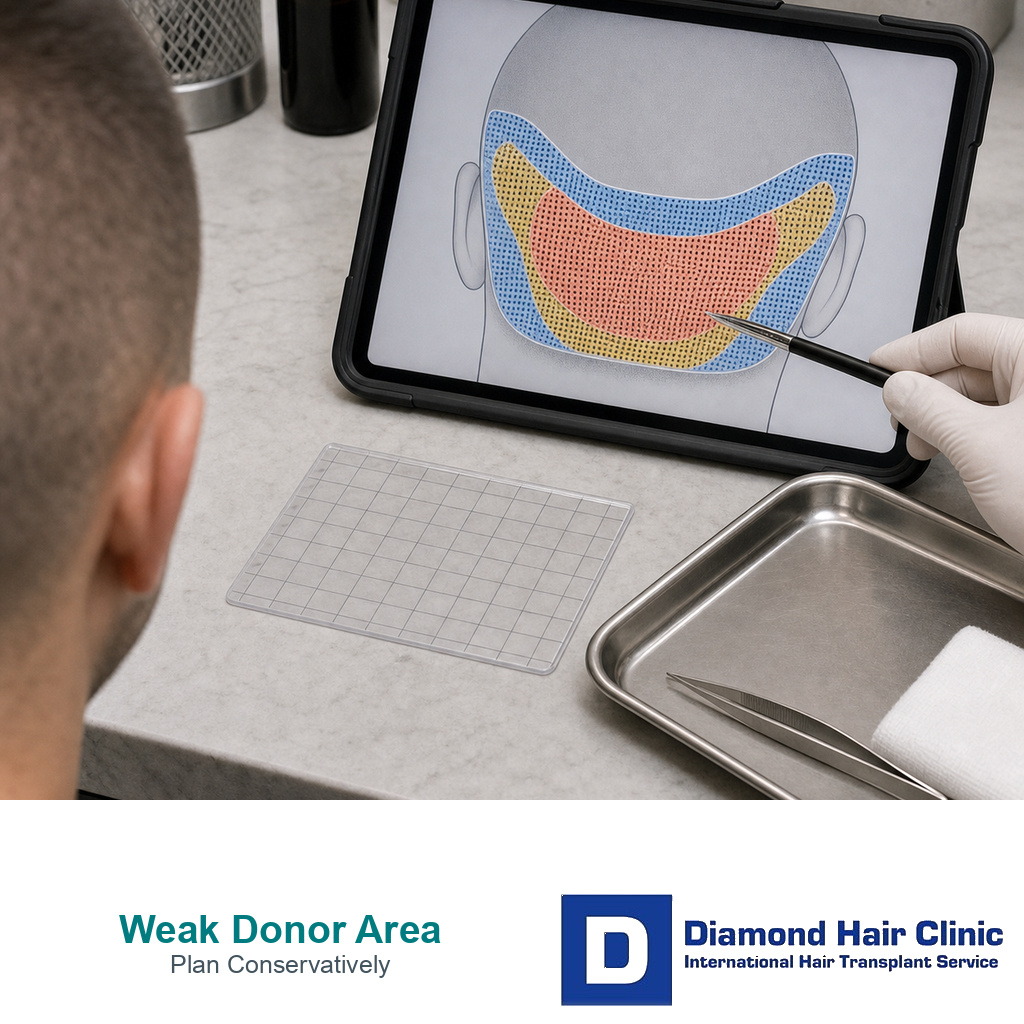
When I examine a limited donor area, I do not judge only from the amount of hair visible at the back of the head. I check density, hair shaft thickness, miniaturization, previous extraction marks, contrast with the skin, crown demand, and how the patient may lose more native hair in the future.
International patients often send photos taken in good lighting. That is useful, but it is not enough by itself. I also need views of the donor sides, nape, crown, and thinning areas, plus medication history and any previous surgery details. If the findings suggest donor miniaturization or a wide future pattern, the plan may become smaller, staged, or not advisable.
Limited donor hair means usable safe supply, not just hair count
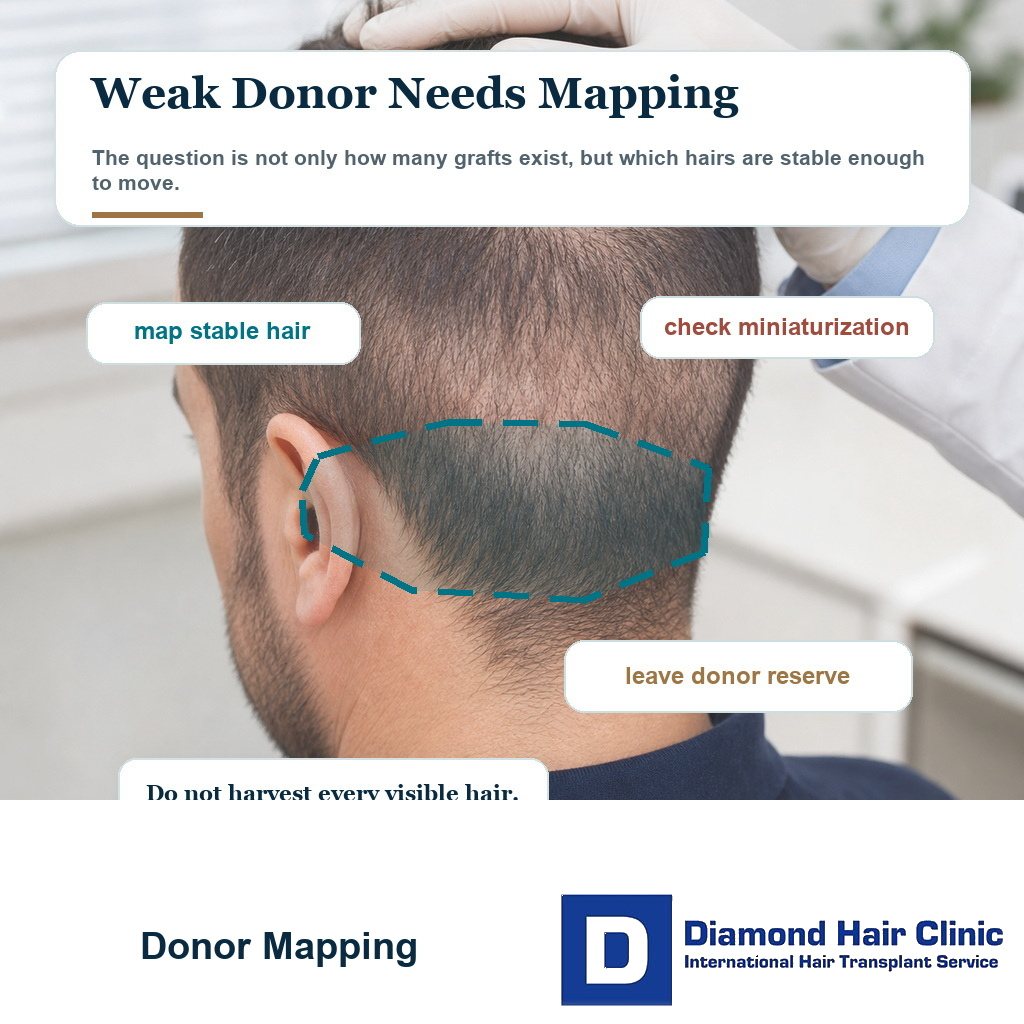
When people say “weak donor area,” they may be describing several different problems. The natural density may be low, and a donor miniaturization check before hair transplant may show whether the hair shafts are stable. The hair shafts may be fine, so the same graft count gives less visual coverage. There may be retrograde thinning, miniaturization, a narrow safe zone, scarring, temporary after illness shedding, or damage from a previous operation.
The first practical distinction is whether the donor only looks weak in a certain photo, haircut, or recovery phase, or whether the actual permanent reserve is limited. These situations are not the same, and I do not plan them the same way. A limited donor supply does not mean every hair there is useless. It means the margin for error is smaller. I have to decide which hairs are stable enough to move, how many can be removed without making the back and sides look see through, and what reserve should stay untouched for the future.
Naturally fine hair needs one type of planning. A donor that has already been overharvested needs another. Ongoing miniaturization may require medical stabilization or a decision to avoid surgery. After chemotherapy, I assess post chemotherapy transplant planning only after the supply has stabilized. A patient who already had FUE also needs a separate review before FUT after FUE, because a strip scar needs surrounding donor hair to cover it.
I always begin with the basics of the donor area in hair transplant because this is the foundation of the whole operation. The recipient area may be where you look first, but the available supply decides what is possible. If the lower nape has active raised bumps, acne keloidalis nuchae can make FUE donor planning unsafe even when the upper donor looks stronger.
A photo can mislead as easily as it can help. Longer hair can hide weakness. Short hair can exaggerate it. Bright light, hair color, scalp contrast, and camera angle can all change the impression.
A proper donor assessment must ask whether the hair is dense enough, stable enough, thick enough, and safely located enough to be used. If one of those answers is uncertain, the plan should become more conservative before any graft is removed. If the discussion includes nape hair as a hairline donor, the lower border stability has to be checked before extraction.
Photos can make donor quality look misleading
Photos can make donor quality look better or worse than it really is. Longer hair can hide low density. Very short hair can make normal spacing look harsh. Strong bathroom light, wet hair, skin contrast, and camera angle can all change the impression.
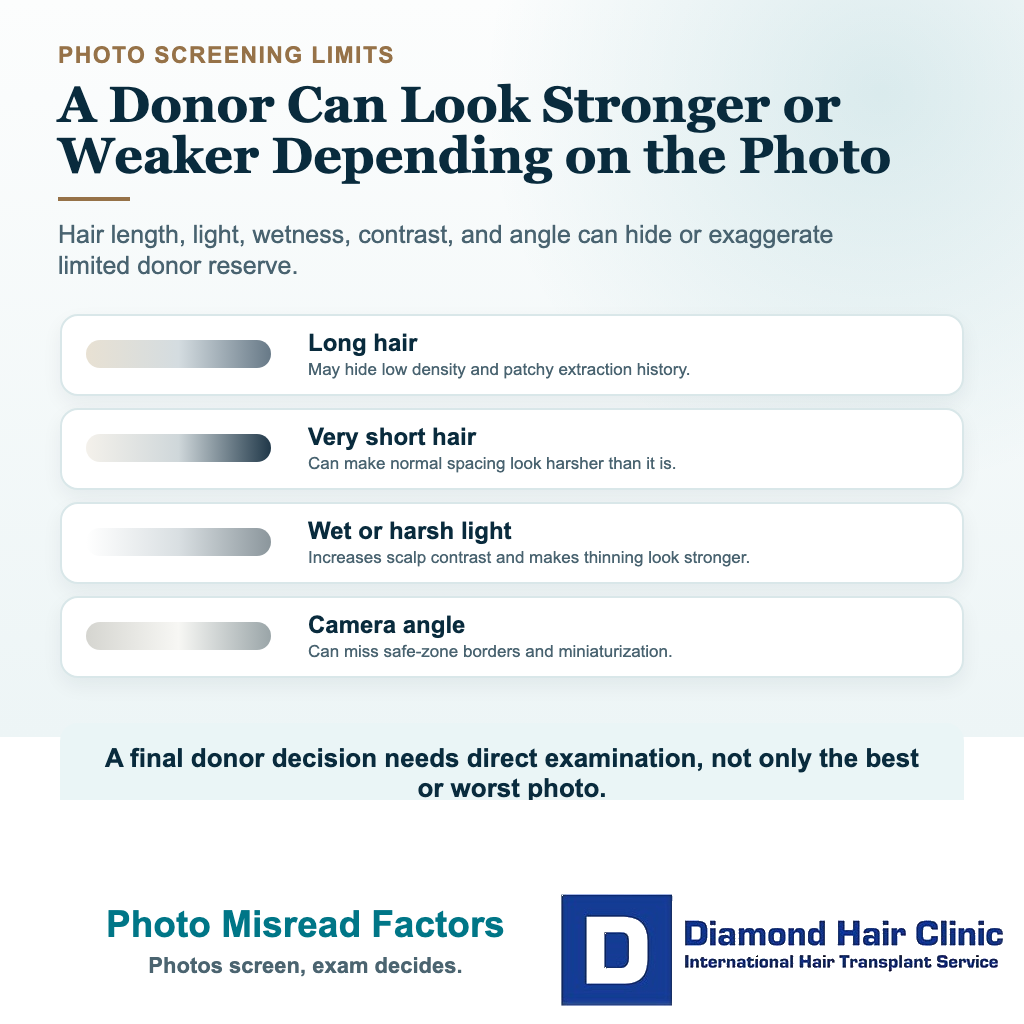
I use photographs for screening, not for final donor approval. A photo can show the shape of hair loss, but it cannot tell me enough about hair shaft thickness, miniaturization, safe zone borders, extraction history, or how the donor behaves when the hair is lifted and trimmed.
If you send photos, I need clear views from the back, both sides, and the crown, with the hair dry and separated enough to show the scalp. I also need age, medication history, family pattern, previous surgery, and whether the donor looks thinner than it did before.
The limitation is even more serious when a surgeon tries to plan a hair transplant from photos. A photo can start the conversation, but it should not become the final approval for a limited donor.
Limited donor hair should not be approved because one flattering photo looks acceptable. The supply must be safe in real clinical conditions, not only in the best image.
Surgeon examination before approving a limited donor plan
Before approving surgery in this situation, I examine the donor from more than one angle and under more than one condition. The hair can look acceptable when it is longer, then look thin when trimmed. That difference matters because many people still want the option to wear their hair shorter after surgery.
Inside the donor, I check for miniaturization. If the donor hairs are already becoming thinner, they may not behave like reliable permanent grafts. Moving unstable hair into the recipient area does not create a stable result. The same donor check matters when a patient reports transplanted hair thinning years later, because an unstable donor can make a late result less dependable.
The borders of the safe donor zone also matter. Harvesting too low, too high, or too far forward can create problems if those hairs are not stable long term. Limited supply gives less room for this kind of mistake.
Hair shaft thickness is another major factor. A donor with lower density but thick, wavy hair may still create useful coverage. A donor with moderate density but very fine, straight hair may have less visual power than the graft number suggests. Donor strength is more than a count.
The recipient area has to be judged at the same time. Limited donor supply may be enough for a small, clear frontal problem but not enough for a broad area across the top. The number only makes sense when it is connected to the area and real capacity, which is the real point behind why hair transplant graft numbers differ. This becomes even more important when the target is a radiated scalp, because hair transplant after scalp radiation can waste donor hair if the recipient bed is not stable.
The final question is whether the plan still protects the future. You may need another session later, or you may need to preserve the option of repair. If the first plan spends too much without that future in mind, it is not responsible.
Knowing when donor hair is too limited for surgery
You cannot know with certainty from a mirror or a few photos. Limited donor hair needs close examination of density, hair shaft thickness, miniaturization, safe zone borders, extraction history, hair direction, and how the hair looks at shorter lengths.
If the donor looks see through even at normal hair length, I slow the assessment down. If the sides are thinning upward, I harvest even more conservatively. If the nape is thinning, or the lower donor looks unstable, I avoid treating that lower zone as if it were permanently safe.
A common warning sign is patchiness after previous FUE. It can feel as if another surgery is the answer, but the reserve may already be close to its limit. When that happens, repair planning must be very careful because every remaining graft has to justify its use.
Donor area overharvesting in hair transplant shows why donor damage can be difficult to correct. Once the donor has been thinned too aggressively, we cannot pretend it is still a full reserve.
Limited supply does not always disqualify you. But it changes the goal. It may mean choosing a mature hairline instead of a low one, waiting on the crown, using a smaller session, or deciding that surgery is not safe enough.
This kind of caution is not rejection for its own sake. A careful no is sometimes better than a confident yes that leaves permanent donor damage.
Limited donor supply can also change the emotional goal of surgery. The focus may shift from full restoration to facial framing, from maximum density to natural improvement, or from immediate surgery to stabilization first. That can be disappointing at first, but it is often what prevents regret. SMP can make limited coverage look stronger, but hair transplant after scalp micropigmentation still has to respect the same donor capacity.
The worst outcome is not always doing less. Sometimes the worst outcome is doing too much with a donor that never had enough reserve for that ambition.
A small hairline transplant may still work with limited donor hair
A small hairline transplant can sometimes work when donor hair is limited if the recession is clear and the design is conservative. The surgery must solve a real cosmetic problem without pretending the supply can support a full transformation.
Sometimes a focused hairline refinement can give a meaningful facial improvement with a modest graft number. In other cases, even a small hairline change may be unwise because the donor is too unstable or the hair loss is still progressing aggressively.
I decide this by asking whether the situation truly fits the criteria I use for a good candidate for hair transplant. Limited donor hair has to pass a stricter test because the cost of a mistake is higher.
The hairline design matters enormously. A low, flat, dense line can consume too many grafts and make future loss look worse. A mature and natural line may give the patient a better result with fewer grafts.
This is a compromise in design, not a compromise in quality. The plan is being adapted to biology instead of being forced against it.
If a clinic offers a dramatic hairline without explaining donor limits, be careful. A good result is not only what grows in the front. It is also what remains safely in the back.
A small hairline procedure still deserves full surgical seriousness. A smaller number of grafts does not make the case simple. When the reserve is limited, even a modest operation must be planned with exact purpose.
Moving some hair is not enough. I check whether moving that hair creates enough visible value to justify what is being taken from the donor reserve.
Limited donor tradeoff map
Four checks before using a weak donor area
A weak donor area changes the question. The plan has to prove safe supply, reduce ambition when needed, choose the highest value zone, and know when not to operate.
Donor proof
Is the donor safe enough to use?
Photos alone can make donor quality look better or worse than it is.
Sometimes. It depends on donor quality, hair characteristics, target size, and whether a smaller plan can still create useful value.
Use this as a planning frame, not a diagnosis or approval for surgery. The final plan still depends on donor reserve, recipient area anatomy, hair type, medical history, and future hair loss risk.
Written limits before travel
With a weak donor, the plan should not only say how many grafts are possible. It should say the highest value zone, the maximum safe harvest range, what haircut or scarring trade off may remain, and which areas will be left untreated.
I also want the refusal boundary to be clear. If magnification shows miniaturization, if the safe zone is narrow, if the crown demand would consume the reserve, or if the patient expects full density everywhere, the plan must be reduced, staged, or stopped. A lower number is not a failure when it protects the last useful grafts.
Aftercare matters more in this group because any shock loss, inflammation, or unexpected donor visibility creates more anxiety. Before travel, I want it clear who reviews the donor after surgery, what photos are needed after returning home, and when a concern needs medical review.
High graft numbers can be dangerous with limited donor hair
Aggressive extraction can be dangerous when the reserve is limited because the scalp may not tolerate it. The more limited the reserve, the more each graft matters.
Patients often think a bigger number means the clinic is more generous. With limited supply, a bigger number can be the opposite. It can mean the clinic is willing to spend what should have been protected.
In advanced hair loss, this is especially risky. Wanting coverage across the front, mid scalp, and crown is understandable. But if the supply is limited, trying to cover everything can create a thin result everywhere and a damaged donor zone. In a Norwood 6 or 7 hair transplant, limited donor reserve often changes the whole goal from full coverage to natural framing.
Advanced baldness in one hair transplant session needs careful limits even with a stronger donor. A limited reserve makes those limits stricter.
A high number can also create false hope. You imagine density, but the grafts are spread across a large area and the donor becomes visibly reduced. Then there are two problems, a thin top and a thin donor.
The unsafe part is not only that the result may look light. Aggressive extraction can leave a see through or patchy donor area and reduce the options for future repair. If the donor area cannot support the number safely, the number should not be used. No marketing promise changes that.

Hairline and crown priority with limited donor hair
When supply is limited, the frontal frame often deserves priority before the crown, if surgery is appropriate at all. The front is what frames the face. It often gives more visible value per graft than the crown.

The crown can require many grafts and still look modest because the hair changes direction and light reflects strongly. With limited supply, spending too many grafts in the crown can remove options that may be needed for the front later.
I am not saying the crown never matters. I am saying the crown must earn its place in the plan. If the crown is small, the reserve is still safe, and the frontal area is stable, crown work may be reasonable. If the supply is limited and the front still needs support, I often give the front priority.
The priority decision in hairline or crown first in a hair transplant becomes even more important when the reserve is limited.
It can feel frustrating when the crown needs to wait. But donor management is not about treating every requested area in one session. The priority is making sure the result still makes sense years later.
If the donor cannot support both areas, the surgeon must choose carefully. A good plan sometimes leaves an area untreated because treating it would weaken the whole result.
I often tell patients that an untreated crown is not the same as a failed plan. In some limited donor cases, leaving the crown lighter is the decision that allows the front to look natural and the supply to remain usable. That is a difficult conversation, but it is a necessary one.
A clinic that promises to treat every area may sound more attractive, but it may also be ignoring the donor reality. A surgeon led plan should make the patient understand why some areas are treated first and why others may need to wait.
Medication may help protect native hair
Medication cannot create a completely new donor supply, but it can sometimes help stabilize native hair, reduce ongoing loss, and clarify whether surgery should be done now or later. The value depends on the patient’s diagnosis and tolerance.
If the donor weakness is mainly natural low density, medication may not change donor capacity much. If there is miniaturization or unstable thinning, medical treatment may be part of the decision before surgery.
Medication matters most when the recipient area still contains miniaturized native hair. If that hair can be protected, the patient may need fewer grafts and the limited supply may be used more safely.
The decision around medication before hair transplant is not only about whether medication grows hair. It is also about whether it helps us spend donor grafts more intelligently.
You should not be pushed into medication blindly, and you should not be pushed into surgery blindly either. Both decisions need medical judgment.
If medication is not suitable, the plan must respect that. But if the reserve is limited and the native hair is unstable, refusing to discuss medical stabilization can lead to a poor long term surgical plan.
In some patients, waiting several months to understand stability is wiser than rushing into surgery. That waiting period may feel frustrating, but it can reveal whether the donor and native hair are stable enough for a surgical commitment.
When the biology is not clear, delaying the operation can protect the patient from a mistake that would only become obvious later.
Beard or body hair has limited use as support
Beard or body hair can help in selected repair or advanced cases, but it is not a simple replacement for a strong scalp donor. These hairs behave differently, look different, and require very careful use.

Beard hair can sometimes add bulk in certain areas, especially in repair planning or when scalp donor supply is limited. But beard hair is not often ideal for creating a soft natural frontal hairline. The front still needs the most refined graft selection possible.
Body hair is even more variable. Growth cycle, texture, length, and survival can differ from scalp hair. It may have a role in some cases, but it should not be sold as a universal solution for every patient with limited donor hair.
If a clinic tells you that beard or body hair will solve everything, slow down. Sometimes it can support a plan. Sometimes it cannot.
Repair cases become difficult here. Someone who has already lost donor capacity may need a combination of conservative scalp grafting, selective beard hair, camouflage strategy, and realistic expectations.
Bad hair transplant repair must start with diagnosis rather than hope. The remaining donor resources have to be used even more carefully.
Beard or body hair also cannot erase the need for a natural hairline. The frontal edge usually needs the softest and most refined scalp grafts. If coarse beard hair is used in the wrong place, the patient may gain coverage but lose naturalness.
I see extra donor sources as support, not permission to ignore scalp limitations. They may help the right patient, but they do not make every limited donor case a good surgical candidate.
Conflicting clinic opinions need careful review
If one clinic says yes and another says no, do not choose the answer that feels more comforting. Ask why. A good yes and a good no should both come with a clear explanation.
One surgeon may say yes because the goal is small and realistic. Another may say no because the reserve is too limited for the patient’s expectations. Both may be reasonable if they are answering different versions of the plan.
The dangerous answer is the one that avoids limits. If a clinic promises a large graft number without discussing donor density, hair shaft thickness, miniaturization, safe zone, and future loss, the consultation is incomplete. When one clinic has already raised a donor concern, compare the plan with the weak donor warning against a high graft quote before extraction.
Numbers can mislead patients here. One clinic may offer 2,000 grafts and another may offer 4,500 grafts. Even a 2,000 grafts hair transplant has to be interpreted through area and donor safety.
Do not compare clinics only by which one sounds more optimistic. Compare the precision of the explanation. A careful clinic will show what can be treated, what should be left untreated, and how the donor may look afterward.
A strong consultation should leave you clearer, not just more excited. If you leave with a big promise but no understanding, you do not yet have a real plan.
Deciding whether surgery is worth the donor risk
I decide this by asking whether the donor can safely support the goal, whether the improvement is worth the grafts spent, and whether enough reserve remains for future thinning or repair. If any of those answers is weak, the plan should become smaller, delayed, or refused.
This decision can lead to a conservative frontal improvement, medication and observation, or no surgery. Fine hair, broad baldness, high contrast, and low donor density make the choice more delicate. Fine hair transplant planning matters here because hair quality can reduce visible coverage even when grafts grow.
Limited donor hair should never be treated like a standard package case. The surgeon must be willing to say what can be improved, what should be left alone, and what would cost too much donor reserve for too little visible gain.
If your donor supply is limited, do not search for the clinic that promises the most. Search for the surgeon who explains the limits most clearly and still protects your future.
Surgery can be possible in selected limited donor cases, but it has to respect what the supply can safely provide. Anything else risks turning a limited donor reserve into permanent regret.
If the realistic plan feels smaller than what you hoped for, take time before making the decision. A careful plan should still make sense the next day, after the excitement of the consultation has faded. If the plan only feels acceptable because the clinic pushed urgency, that is not a good sign.
With limited donor hair, waiting can be part of the surgical plan, not a sign that nothing is being done. The plan should improve your appearance without spending the one resource that your future result may still need.