



Bad Hair Transplant Repair Planning
If you think you need repair after a bad hair transplant, my first advice is to separate an urgent medical problem from a cosmetic problem. Fever, spreading redness, increasing pain, pus, black skin, or worsening swelling need immediate medical review.
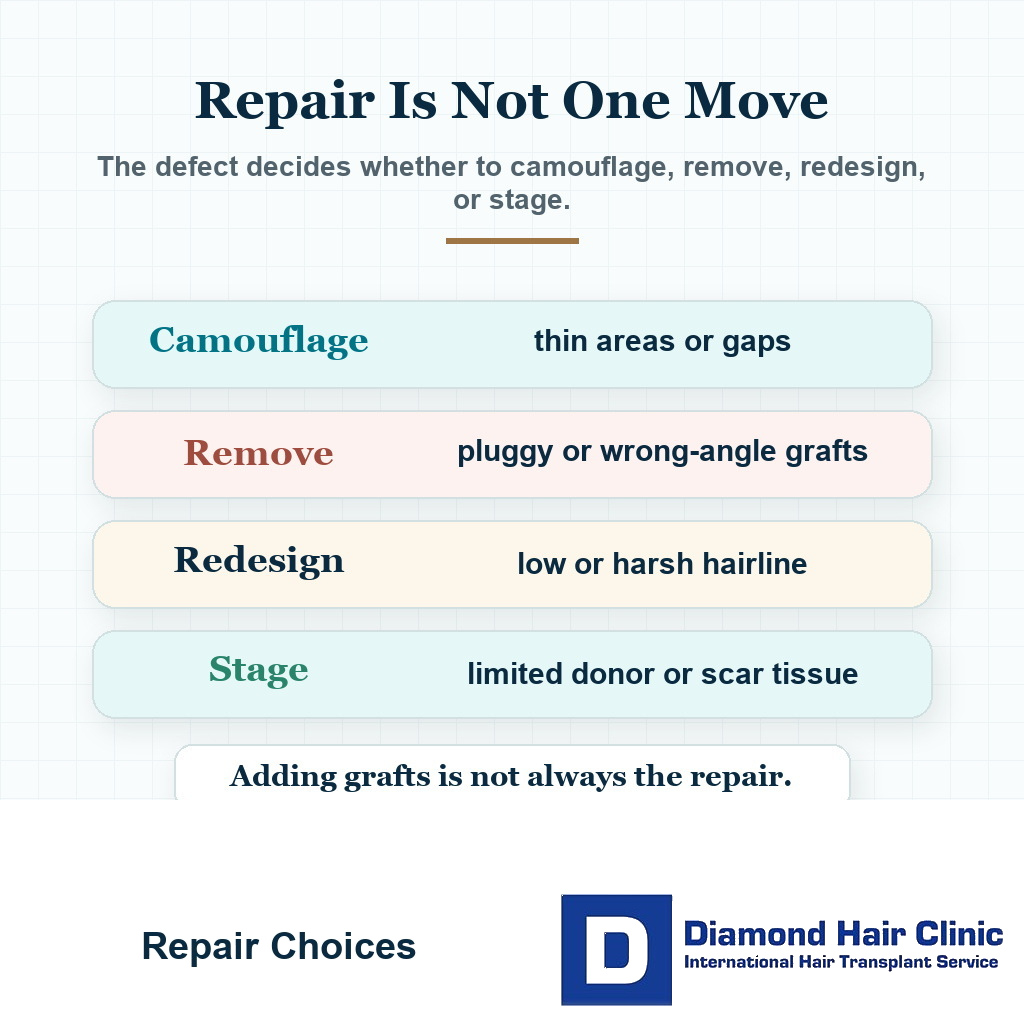
If the weak point is cosmetic, the safest first move is not another surgery. Most repair decisions need to wait until at least 12 months, and many cases are judged more responsibly between 12 and 18 months. Before repair, collect photos, records, graft numbers, medication history, and a proper donor area assessment. A pluggy hairline repair is one of the repair situations where adding more grafts is not always the first answer.
This may not be the answer you want when the result feels visible and humiliating. The instinct is to fix it immediately, confront the clinic, or book another operation as quickly as possible.
But repair surgery is not the same as a first surgery. The donor area may already be reduced. The recipient area may contain scar tissue, including a hairline advancement scar. The hairline may need redesign, removal, camouflage, or a staged plan. When the visible problem is a donor line from strip surgery, the question becomes whether FUE grafts can repair a FUT scar without wasting the remaining donor supply. The separate guide to removing transplanted hair explains when removal helps and when it can make repair harder.
How I judge repair risk before offering surgery?
Before I offer repair, I want to know what was done in the first operation and what donor reserve remains. Repair planning is not only covering a bad area. It may require removing grafts, softening a hairline, rebuilding density in a limited zone, or refusing a second surgery when the remaining donor cannot support it.
For international patients, I ask for clear photos from normal distance and close range, the original graft number if available, the date of surgery, medication history, and donor area images. Without that context, an easy repair promise is not trustworthy. I compare the repair plan with results from hair like yours, not only with the best repair photo in a gallery.
Take the disappointment seriously, but slow down before making a second mistake. Hair transplant regret after surgery is real, but regret cannot be allowed to make the surgical plan.
Repair work begins with diagnosis. Not every bad looking result is the same problem, and not every worried person actually has a bad result yet. One part of the diagnosis is deciding whether selected bad hairline grafts should be removed, softened, or left alone before another repair is planned.
What the repair plan must say in writing?
Before repair, I want the plan to name the real defect. Is the problem low design, pluggy grafts, wrong direction, weak density, visible scarring, donor depletion, active native loss, or timing that is still too early to judge? Those are different operations.
The written plan should also say what I am not promising. I may be able to soften a line, improve a transition, remove selected grafts, or rebuild a limited zone. I cannot promise to erase every old graft, make scarring disappear, or recover donor hair that has already been spent.
When donor reserve is too weak, scalp healing is not mature, native loss is moving quickly, or the requested density would spend the last useful grafts, repair should be delayed, reduced, or refused. This is not pessimism. It is how the next surgery avoids becoming the next problem.
First steps when a transplant seems wrong
The first thing to do is stop trying to diagnose the result from fear. Write down the date of surgery, the technique used, the graft number you were told, the clinic name, the surgeon involved if one was named, your medication history, and the main problem you see.
Then gather photographs in consistent lighting. Take front, both temples, top, crown, donor area, and side views. Use dry hair, similar hair length, and no fibers or concealer. If there is previous SMP, hair transplant after scalp micropigmentation needs separate assessment because pigment can hide the real hairline and density pattern. If the issue is camouflage after a poor result, SMP with hair transplant results needs separate review from surgical repair.
Do not rely only on dramatic close up photos. A harsh close photo can make any transplant look worse. But do not hide the problem either. The goal is accurate documentation.
If you have operation records, graft count, consent forms, invoice, post surgery instructions, or day one photos, keep them. These details may help a repair surgeon understand what was done.
Next, contact the original clinic in writing and ask for your medical details. This is not because the clinic will always help. It is because a written record can be useful.
Do not begin with public threats or angry messages. If the result is truly poor, organized documentation is more useful. If the result is too early to judge, anger may only make the next months harder.
Organize the facts before reacting publicly. A surgeon who repairs hair transplants needs facts, not only frustration.
Once the facts are organized, seek an independent evaluation from a surgeon who actually understands repair cases. A salesperson cannot assess donor capacity, hair angle, scar tissue, graft survival, and long term planning properly.
Describe the problem in plain language. A low hairline, weak density, patchy donor area, unnatural direction, or pluggy grafts each require a different repair plan. A clear description makes the consultation more medical and less emotional.
Sometimes someone says the whole result is bad, but when I examine carefully, there are two or three specific issues. That distinction changes the repair plan. Surgery needs to target the real problem, not the general feeling of disappointment.
Waiting before judging the result
If you are at month 3 or month 4, it is usually too early to call a transplant failed. The shedding phase can make the scalp look worse before it improves, and meaningful cosmetic growth often does not begin until around month 4.
Between months 6 and 9, the picture becomes more useful, but it is still not the final result. Density, caliber, texture, and coverage can continue to improve.
The mature result is usually judged around 12 to 18 months. That timeline matters because hair transplant growth is not immediate, and early judgment can lead to unnecessary panic.
Whether a result is a failed hair transplant or too early matters because timing protects you from calling a normal ugly phase a disaster.
There are exceptions. If the hairline was designed obviously too low, the angles are visibly wrong, there is clear infection damage, or the donor area was overharvested, some concerns can be recognized earlier.
Even then, recognizing a problem early does not always mean repairing it early. The scalp still needs time to heal and mature before another surgery is planned.
A common mistake is to decide on repair at month 4 because you hate the mirror. The emotion is understandable, but month 4 is not a mature surgical result.
Another mistake is waiting forever when the result is clearly poor after 12 to 18 months. At that point, a proper repair assessment becomes reasonable if you have realistic goals and enough donor reserve.
There is an uncomfortable middle period between month 6 and month 12. You can often see enough to worry, but not enough to know the final answer. In that period, monitoring, photography, and planning discussions are more useful than aggressive decisions.
Planning can begin before the final month, but committing to repair is different from preparing for repair. The scalp, grafts, and native hair all need time to reveal what is truly there.
The carousel below splits the judgment checkpoints into one image each. Swipe sideways, use the arrows to move one slide at a time, or use the numbered indicators under the image to jump to a specific slide.




Mistakes to avoid before repair
The main thing to avoid is a rushed second surgery. When you feel embarrassed, the fastest possible correction can look attractive, but fast repair is not always safe repair.

Do not let another clinic promise to fix everything before the first result has matured, the donor area has been examined, and the exact problem has been diagnosed. Do not pay a new deposit, accept a new graft number, or book a correction before those basics are clear. If the first surgery damaged donor reserve, the second decision has to be even more careful.
Do not keep changing every treatment at once without a plan. Starting, stopping, and restarting minoxidil, finasteride, supplements, fibers, cosmetic cover, or scalp treatments can make it harder to understand what is truly happening.
Do not tattoo, camouflage, or permanently alter the donor or recipient area before a repair surgeon has examined it. Sometimes camouflage can help later, but if it is done too early or in the wrong place, it can make diagnosis and future planning harder.
Do not judge the result only with wet hair, shaved hair, harsh overhead light, or distressed close up photos. Those images can be useful for documentation, but they must not become the only reality in your mind.
The waiting period needs to be active, not chaotic. Take consistent photos, collect records, stabilize the scalp, protect the donor area, and get a serious repair assessment when the timing is appropriate.
Urgent signs versus cosmetic concerns
Urgent problems are medical, not cosmetic. Increasing pain, spreading redness, fever, foul smell, yellow or green pus, skin that turns black, or rapidly worsening swelling need prompt review.
These signs are not something to watch casually for months. Infection, vascular compromise, and tissue injury require timely medical attention.
For necrosis warning signs after a hair transplant, the timing question is when a scalp problem is beyond normal redness or scabbing.
Most bad transplant complaints are not emergencies. They are about density, design, angles, gaps, scars, donor appearance, or slow growth. Those problems matter, but they usually need assessment after the healing timeline becomes clearer.
The concern is confusing these two categories. Infection cannot be dismissed as something to watch for months. Normal slow growth at month 3 cannot be pushed into repair.
Good medical judgment means knowing which situation you are in. The wrong reaction in either direction can create harm.
If something feels medically wrong, contact the operating clinic and seek local medical attention if needed. Do not wait for an online opinion when the scalp is worsening.
If the scalp is medically stable but the result looks poor, the repair conversation can be more measured. That is when diagnosis, timing, donor supply, and realistic options matter most.
Pain and dissatisfaction also need to be separated. You may dislike the hairline and feel distressed, but that is not the same as a scalp that is becoming infected. A stable cosmetic problem gives us time. A worsening medical problem does not.
Identifying the type of bad result
This question matters because the repair plan depends on the defect. A thin result is not the same as a low hairline. A low hairline is not the same as wrong angles. Wrong angles are not the same as donor damage. In milder cases, touch up graft planning may be more appropriate than a full repair strategy.
Weak density may be the main issue. The scalp still shows through, so the result feels like a failure. The reasons hair transplant results look thin are not all the same, and density disappointment needs its own diagnosis.
In other cases, the main issue is design. The hairline may be too low, too straight, too round, too aggressive, or not suitable for your face and future hair loss.
Angle can be the main issue. The hair may grow in a direction that looks unnatural. This is harder to hide because direction affects how the hair behaves even if growth is good.
Blending may be the weak point, such as a gap between transplanted and native hair. This can happen when the transplanted area and native hair behind it were not planned together.
The weak point can also be donor area damage. This may appear as patchiness, overharvesting, visible thinning, scars, or an uneven pattern that becomes obvious with short hair.
Sometimes the transplanted hair is growing, but the surrounding native hair continues to miniaturize. That can look like transplant failure when the real problem is ongoing hair loss around the grafts.
A repair surgeon must identify the true problem before offering treatment. Otherwise, the second surgery may chase the wrong target.
Magnification and donor assessment matter here. The naked eye can miss miniaturization, poor direction, and scars hidden by longer hair. A repair plan based only on selfies is not serious enough.
A repair assessment needs to ask whether the result looks bad in every condition or mainly in extreme conditions. Harsh light, wet hair, and very short hair can expose weaknesses that ordinary social viewing may not show. That does not make the concern fake. It means the repair goal must be realistic.
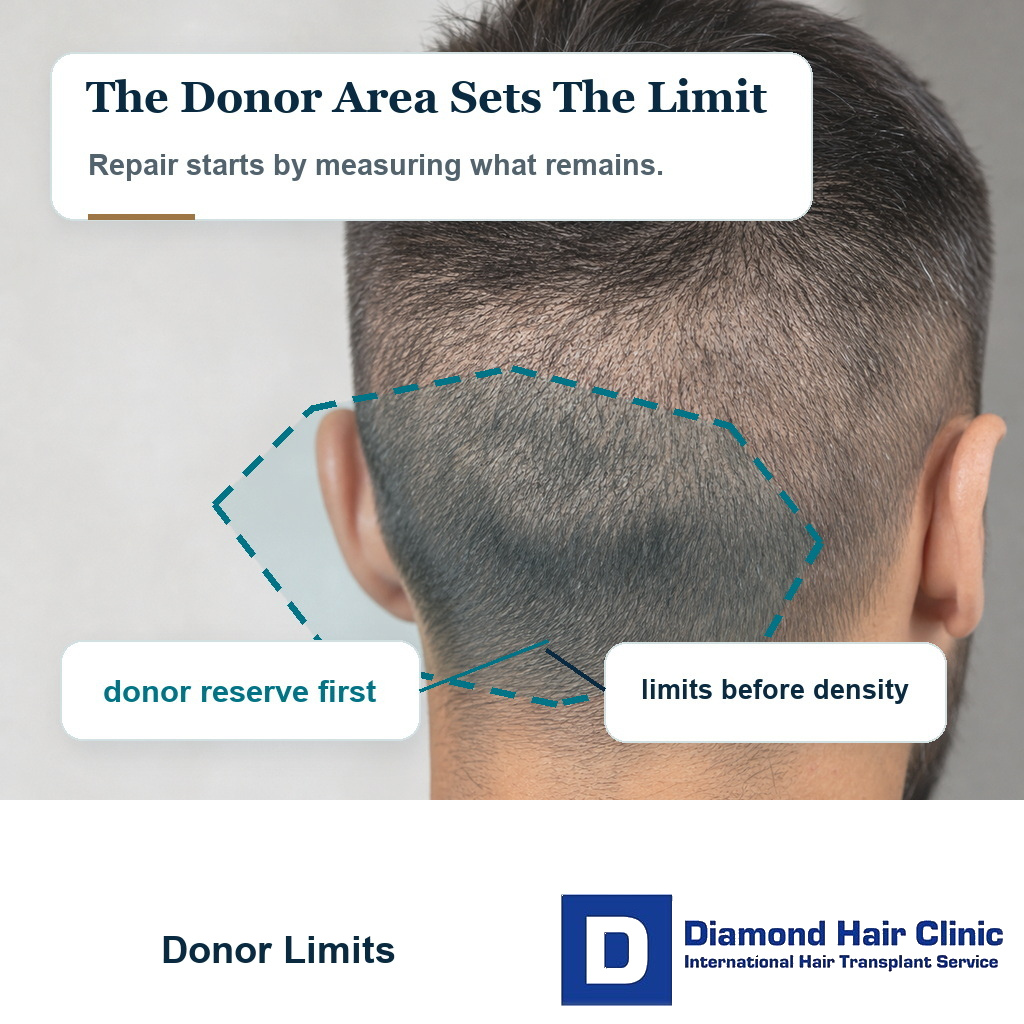
Donor area comes first in repair planning
Donor reserve is the foundation of every repair plan. Before improving the front, the first question is what remains available at the back and sides of the scalp.
A strong reserve gives wider repair options. If donor reserve is weak, overused, or scarred, the plan must be more conservative.
Donor area overharvesting is such a serious problem because a poor hairline can sometimes be corrected, but a heavily damaged donor area limits almost every future option.
It is natural to focus on the recipient area because that is what you see in the mirror. But the donor area decides how much correction is possible.
The repair assessment looks at density, hair caliber, extraction pattern, scarring, miniaturization, and whether the donor area still looks natural. It also has to consider how you want to wear your hair in the future.
If you want a short haircut but donor reserve looks visibly depleted, the repair plan must include that reality. Adding grafts to the front will not solve a donor that looks damaged.
Sometimes repair surgery is possible but limited. Sometimes the best option is not another large transplant, but a smaller correction, medical stabilization, hairstyle adjustment, or camouflage.
A responsible surgeon needs to tell you what can be improved and what cannot be fully reversed.
In some repair cases, donor reserve is still good and there are real options. In others, the donor has already been pushed too far. When that happens, the most ethical answer may be a smaller correction rather than another large session.
This can be difficult to hear because you may want the second operation to undo the first. But the donor area does not reset. Repair planning begins by accepting what remains, not by pretending nothing happened.
Returning to the same clinic
Sometimes returning to the same clinic can make sense, but only if the clinic understands the problem, takes responsibility, has a qualified surgeon involved, and can explain a medically sound repair plan.
If the first operation was done in a high volume system with poor planning, weak surgeon involvement, rushed consultation, or unclear responsibility, be very cautious about going back. A free repair is not always the right repair. If the same system created the problem, repeating the same system may deepen the damage.
This matters especially when the first clinic has the red flags of hair mill clinics. A repair case needs more judgment, not more volume.
Before returning, the clinic needs to explain the diagnosis, the repair design, the donor strategy, the recipient area plan, and what will be done differently this time. A vague answer must not become reassuring because of the word guarantee. A guarantee does not restore donor supply, correct poor judgment, or turn a technician led system into a surgeon led repair plan.
Ask whether the clinic is willing to provide your records and photographs. A clinic that refuses basic documentation may not be the best place for repair.
The decision cannot be driven only by compensation. A small refund, a free correction, or a discounted second surgery can become expensive if it spends more of the remaining donor supply without a better diagnosis. The bigger question is who is most likely to protect the remaining donor and make the next result better.
Second surgery can help in selected cases
Sometimes yes, but not always completely. A second surgery can improve density, soften a harsh hairline, fill gaps, camouflage some problems, and create a more natural frame when the donor area allows it.
But a second surgery cannot erase every mistake. It cannot create unlimited donor hair. It cannot fully remove all scarring. It cannot always correct every wrong angle without graft removal or staged work.
The question of a second hair transplant needs careful judgment. A second surgery is not always a repair. It may be improvement, completion, correction, or sometimes a bad idea.
Repair surgery often needs a hierarchy. First, protect donor reserve. Second, correct the most visible unnatural feature. Third, improve density where it gives the most cosmetic value. Fourth, avoid creating a new problem.
If the hairline is too low and pluggy, simply adding more grafts behind it may not solve the issue. The first visible line may still look unnatural.
If the result is thin but the design is natural, adding density may be useful. If donor reserve is strong, the plan may be straightforward. If the donor is weak, the plan changes.
If the original surgery caused scarring or infection related loss, the recipient area may behave differently. Graft survival can be less predictable in scar tissue.
A responsible repair plan needs to be clear about limits. It is better to underpromise and protect the patient than to promise a perfect reset that surgery cannot deliver.
Sometimes the best second surgery is not very large. A few carefully placed grafts can soften an edge or improve a weak transition. In other cases, a larger correction is needed, but only if the donor area can support it.
Repair growth follows the same biological timeline as other hair transplant growth. It is not instant. Even after repair, early shedding and months of waiting may still happen.
Graft removal and hairline correction options
Graft removal may be needed when the hairline is too low, too straight, too dense in the wrong place, pluggy, or growing in an unnatural direction. In these cases, adding more grafts is not always the answer. The same repair logic becomes even more delicate when the transplanted area is on the face, because beard transplant regret may involve hair removal, skin texture, and scar trade offs at the same time.
The first row may be the weak point. If the first row is wrong, everything behind it may still look wrong. A repair surgeon must decide whether to camouflage, remove, redistribute, or redesign.
Graft removal can involve surgical extraction, electrolysis in selected cases, or a staged approach. The right choice depends on hair caliber, skin condition, graft angle, density, scar risk, and your goals.
Quick promises in this area deserve caution. Removing grafts can create small scars, and not every extracted graft can be reused successfully. You need to understand the trade off before agreeing to removal.
Sometimes a higher and softer visual hairline can be created by placing finer grafts in front of or around the old line. Sometimes that would only make the hairline lower and worse.
Repair planning is very individual. Two people may both say they have a bad hairline, but one needs density refinement and the other needs removal.
Hairline repair is not only technical. It is aesthetic and strategic. The surgeon must think about facial proportion, age, future loss, donor reserve, and how the result will look when you are 40, 50, or 60.
The plan must not erase every old graft at any cost. The purpose is to create a new plan that looks natural and protects the future.
Removing everything that bothers the patient needs caution. Sometimes removal is necessary. Sometimes removing too much creates more scarring and less coverage. Repair needs to be a plan, not a reaction to frustration.
Documenting the problem before repair
Good documentation helps you and the repair surgeon. Take photos in the same room, with the same lighting, at the same distance, and with the hair dry.
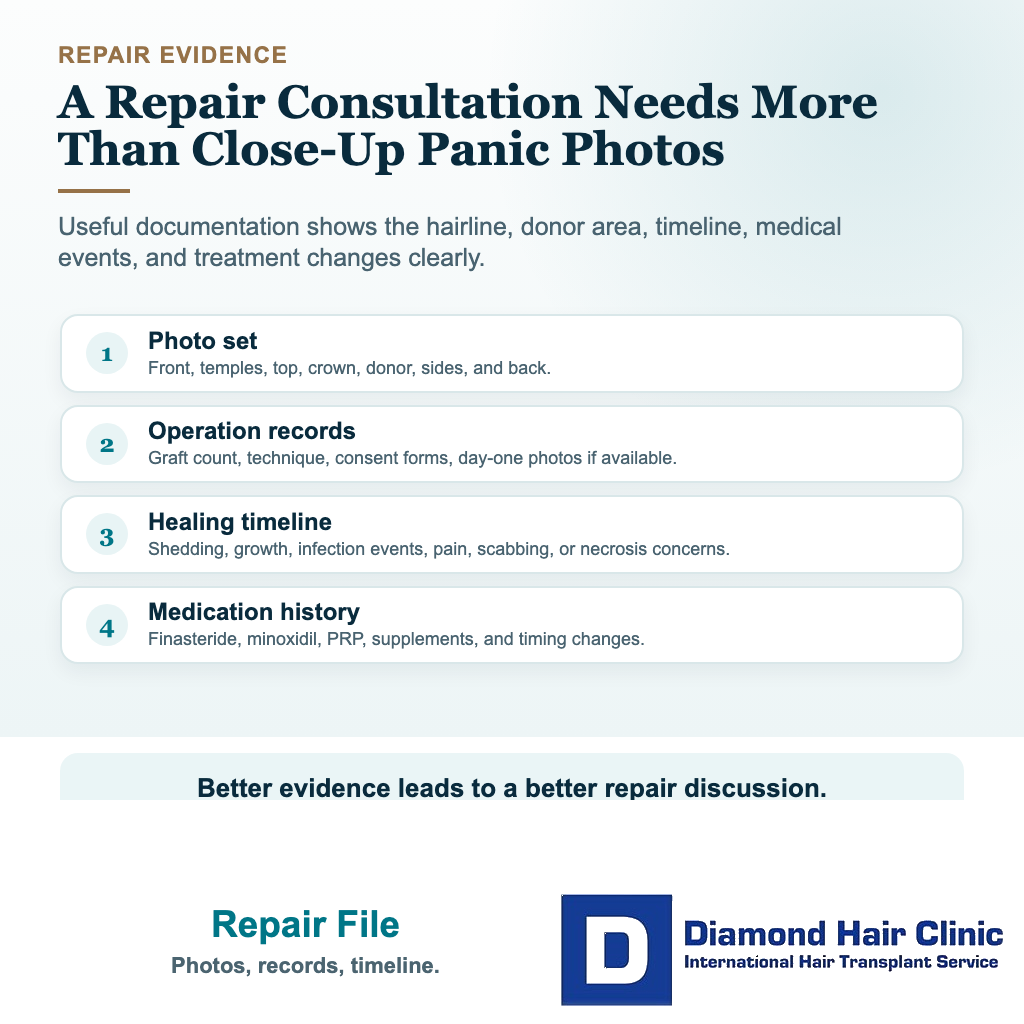
Include the hairline, temples, middle scalp, crown, donor area, sides, and back. If the problem appears only in harsh light, take one set in harsh light and one set in ordinary light.
It matters because before and after photos can mislead when lighting, angles, hair length, or styling are changed. The same rule applies when documenting a poor result.
Keep a timeline. Write down when shedding began, when growth started, when you noticed the problem, and whether it improved or worsened.
If there was infection, bleeding, necrosis concern, scabbing problems, or severe pain, record the dates and any treatment given. Medical events can affect repair planning.
If you used finasteride, dutasteride, minoxidil, PRP, vitamins, or other treatments, note when you started, stopped, or changed them. Ongoing native hair loss can make a transplant look worse even if the grafts survived.
A repair request needs more than one emotional photo. Send a structured case instead. A structured case saves time and helps the surgeon give a more serious opinion.
The more complex the case, the more useful the documentation becomes.
Good documentation also protects you from changing the story in your own mind. When you are distressed, every mirror check can feel worse than the last one. Consistent photos make the discussion more grounded.
They also help a surgeon see whether the weak point is stable. A stable problem can be planned. A changing problem may need more time, medical treatment, or a different diagnosis before surgery.
Deciding whether repair surgery is wise
Repair surgery is wise only when the diagnosis is clear, the donor area can support the plan, the scalp has healed enough, and the expected improvement is worth the risk.
You also have to be emotionally ready. A bad first experience can make certainty feel urgent, but repair surgery still requires patience, healing, shedding, and months of waiting.
Before repair, the case needs to be reassessed as if you were being considered again as a candidate for a hair transplant. You may have been a poor candidate the first time, and that must not be ignored during repair.
Medical treatment may need to come first. If native hair is still thinning quickly, repair may improve one area while another area continues to weaken.
The repair plan needs to be able to say what can be fixed, what can only be improved, and what should not be touched.
A responsible repair plan is not the most aggressive plan. It improves the visible problem while protecting what remains.
Sometimes that means a second surgery. Sometimes it means waiting. Sometimes it means removal before implantation. Sometimes it means accepting that only partial improvement is realistic.
As a hair transplant surgeon, my job is not to make you feel reassured for one consultation. The plan has to still make sense years later.
If you have had a bad hair transplant, do not rush into the next chair. Get the diagnosis right first. Repair is often possible, but only when the next decision is more careful than the first one.
Think about it this way. The first transplant may have been disappointing, but the next decision can still be intelligent. The repair needs to be more precise, more conservative where needed, and more realistic than the surgery that created the problem.