


Third Hair Transplant Safety and Donor Area Limits
A third hair transplant can be safe, but only when the donor reserve is still real, the previous surgeries grew well enough to justify another operation, and the new goal is modest. If the third plan depends on a very large graft number, weak donor hair, or a promise to cover everything, I take a much more conservative view. At this stage, surgery is no longer only about filling a gap. My priority is protecting the last useful grafts while improving the area that matters most.
Every previous surgery changes the next one. The scalp has already been operated on. Some donor hair has already been spent. Some areas may have scar tissue. Some native hair may still be thinning. The assessment has to begin with the donor supply, not with the patient’s wish list. That same donor reserve check is stricter when a patient is considering FUT after FUE as another harvest route.
For a third operation, the first two surgeries need a clear review. What did they achieve? What did they change or harm? What still looks natural? What can realistically be improved? What should be left alone? A third hair transplant is a strategy decision, not just another small correction. It should have a finish line. The visible gain has to be weighed against the donor reserve that must stay protected afterward.
A third hair transplant can be reasonable in selected cases
A third hair transplant can be reasonable when the first two surgeries were conservative, the donor zone still looks even, the patient has a clear untreated area, and the aim is not excessive density everywhere. In this situation, the third surgery may be part of a staged plan rather than a rescue operation.
Some patients had the frontal hairline restored first, then the midscalp improved later, and only after years they begin to consider the crown. Other patients had a small first surgery many years ago, a second operation to update the result, and now want a careful refinement. These cases are very different from a patient who already had two aggressive operations and now wants one more large session because they are still dissatisfied.
The third operation is often where surgical judgment matters most. The first surgery may create excitement. The second may complete a visible area. The third has to answer a harder question. Is there still enough donor capacity to improve the result without creating a new problem? When that answer becomes weak, the next discussion is when to stop chasing another hair transplant, not how to force one more session.
The third decision shares some logic with a second hair transplant, but it should not be treated as the same decision. A second operation may still have some flexibility. A third operation usually has much less room for error.
A reasonable third surgery usually has a narrow target. It may soften an exposed area, improve a transition zone, place limited grafts into the crown, or correct a small density gap. It should not be sold as a final chance to create unlimited coverage. If the plan sounds too broad, the donor may pay the price.
Emotional readiness matters too. A patient who understands limits often makes better decisions than a patient who is chasing a photograph. If the patient can accept improvement without demanding perfection, a third procedure may be discussed more safely.
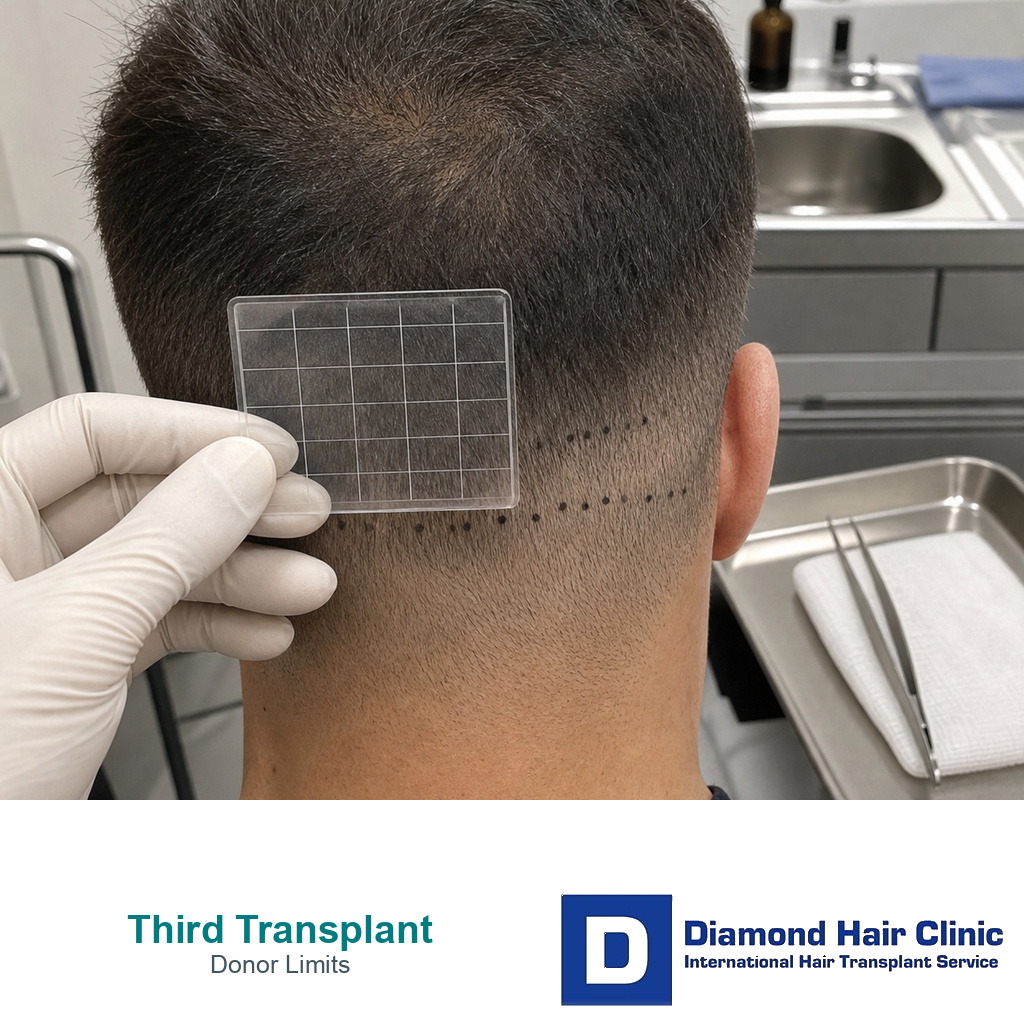
The donor supply comes first
The donor supply is limited, and every future hair transplant plan depends on how much remains. A removed graft cannot simply be returned to the donor zone. This sounds obvious, but many patients only understand the meaning after two surgeries, when the back of the scalp begins to look thinner, uneven, or harder to hide with short hair.
For a third hair transplant, the donor region needs to be examined under good lighting, from several angles, and with attention to hair length. Patchiness, see through areas, extraction scars, thinning above or below the safe zone, and differences between the right and left sides all matter. A donor can look acceptable in one photograph and still be weak in real life.
The previous extraction pattern also matters. Even distribution, extraction height, spacing, and future donor management matter because a donor that was treated as a number to collect may have fewer safe options left.
The risk of overharvesting in hair transplant becomes very serious at this stage. Overharvesting is not only a cosmetic issue at the back of the head. It also reduces future repair options. If the donor is damaged, the surgeon has fewer ways to improve the front, crown, or previous mistakes.
Patients sometimes say they are not concerned if the donor looks a little thinner, as long as the top looks better. That feeling is understandable, but spending the donor carelessly can create a permanent problem. A weak donor supply can limit hairstyle choices, expose scarring, look worse in bright light, and make future correction much harder.
The third operation should protect the donor appearance, not only the recipient area. A natural result is not just the front view in a photograph. It is the whole head under normal life conditions.
Estimating what is really left after two surgeries
The remaining reserve cannot be estimated by subtracting a number from a chart. It has to be judged from the donor that is actually in front of me. Two patients may both say they had 6,000 grafts removed, but one may still have a balanced donor and the other may already have visible depletion.
The old graft numbers may also be unreliable. Some patients were given rounded numbers. Some were given marketing numbers. Some had mixed graft quality. Some had many single hair grafts, while others had stronger grafts with several hairs. The number alone does not tell me how much useful donor value remains.
In a third surgery, a smaller number can sometimes be wiser than the number the patient expected. For one patient, 1,000 to 1,500 carefully placed grafts may create a meaningful improvement. For another patient, even a small extraction may be too risky if the donor is already thin, scarred, or uneven.
The decision should compare visible gain with donor cost. A small third procedure that softens one exposed transition can be wiser than a broad plan that spreads grafts thinly across too many areas and leaves the donor looking weaker.
The first two surgeries shape the third plan
The first two surgeries change almost everything. They change the donor reserve, the scar pattern, the recipient area tissue, the hairline design, the patient’s expectations, and sometimes the patient’s trust. A third hair transplant cannot be planned as if the scalp is untouched.
The first step is to separate what grew well from what did not. If the previous grafts grew strongly and the design is natural, the third procedure may be simpler. If growth was weak, the next question is why. Was the problem poor graft handling, poor placement, poor survival, ongoing native hair loss, unrealistic density expectations, or a donor that was not strong enough from the beginning?
The claimed graft numbers should also be compared with the visible result. Sometimes a patient was told that a high number of grafts were used, but the cosmetic result does not match that number. Sometimes the donor appears too depleted for the amount of visible improvement. In those cases, the third surgery must be planned with even more caution.
This is closely connected to why hair transplant graft numbers differ. A number alone does not tell me whether surgery was wise. The area treated, hair caliber, number of hairs per graft, donor density, spacing, survival, and future pattern of loss all change the meaning of the number.
The previous hairline also matters. If the hairline was designed too low, too straight, or too dense for the patient’s future pattern, a third operation cannot simply add more hair behind it and call that a good plan. Sometimes the old hairline design must be softened or corrected first.
The crown may also have changed. A patient may have used many grafts in the front and midscalp, then discover that the crown is still thin. In advanced hair loss, the crown can consume a large number of grafts while giving a modest visual change. The third plan must decide whether crown improvement is truly worth the donor cost.
The third plan should be smaller, clearer, and more realistic than the first plan. If the first two surgeries were already aggressive, the third should not repeat the same thinking.
In the 5 slides below, I show how the first two surgeries affect the third plan. Use a sideways swipe, the arrows, or the numbers below the image.


Records from the first two surgeries help
Bring everything you have, even if it feels incomplete. The graft numbers, operation dates, clinic names, technique used, shaved donor photos, day one recipient photos, and result photos at 12 months can all help. They show where grafts were placed, where they were not placed, and how well the previous surgery actually grew.

Old photos are especially useful because the scalp changes over time. A current weak area may be a poor transplant result, but it may also be native hair loss around an area that once looked better. Without the timeline, it is easy to blame the wrong cause.
If you do not have records, the scalp can still be examined. But the discussion becomes more cautious. The story has to be reconstructed from donor appearance, scar pattern, hairline design, density distribution, and the patient’s memory. That is possible, but it should never be rushed.
Technique matters more by the third surgery
The technique matters more because the margin for error is smaller. In an untouched donor region, a surgeon may have more flexibility. By the third surgery, every extraction must respect previous harvesting, remaining density, scar pattern, and future need.
A carefully planned FUE hair transplant approach is often useful because it allows selective extraction without creating a new strip scar. But FUE does not by itself make the plan safe. Poorly planned FUE can still overharvest the donor and create visible thinning.
If the patient had a previous FUT hair transplant, the linear scar, scalp tightness, and remaining donor density all matter. Sometimes FUE can be used around old strip work. Sometimes grafts can be placed into a scar. Sometimes the donor should not be pushed further. The technique must serve the future plan, not the other way around.
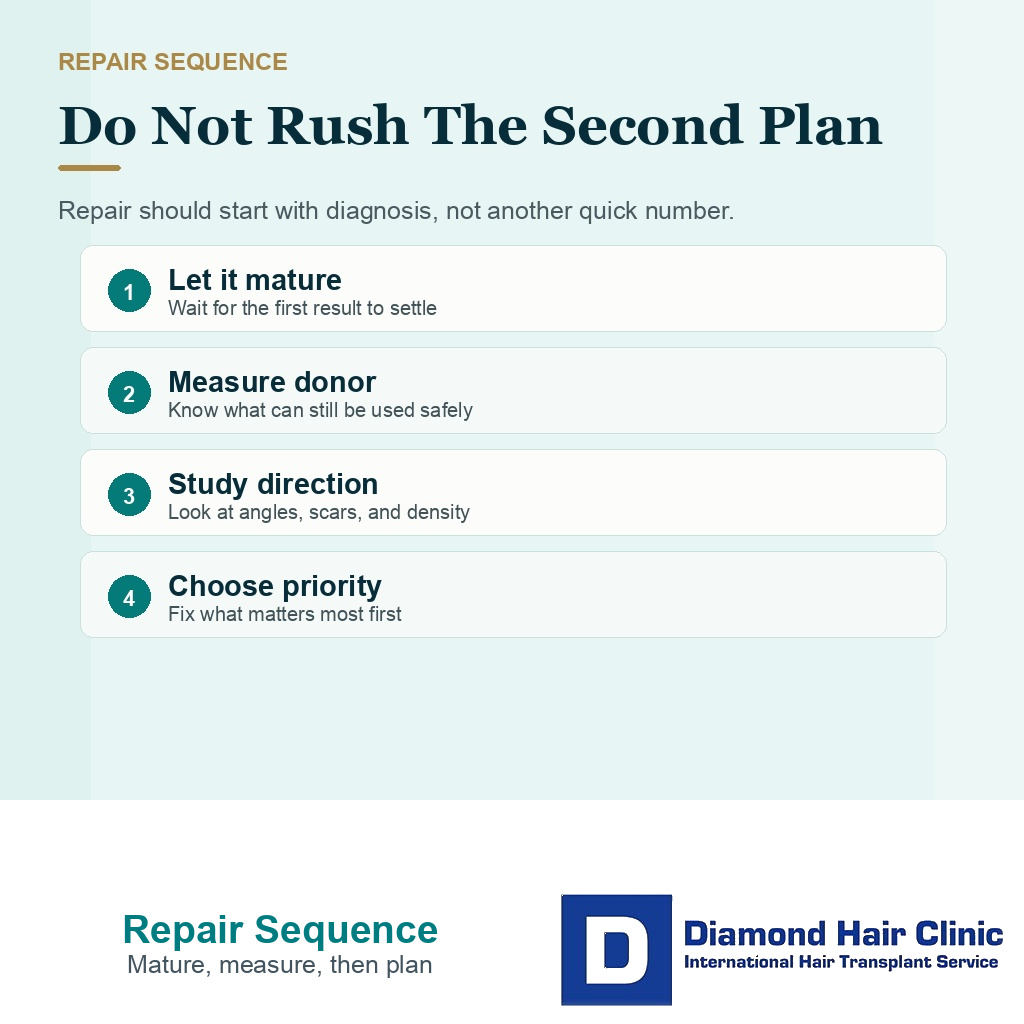
A third transplant can sometimes repair a weak result
Sometimes a third hair transplant can improve a weak or unnatural result, but repair work is not the same as adding density. Repair begins with diagnosis. The weak point may be poor growth, wrong direction, a pluggy hairline, an overly low design, visible scarring, donor damage, crown depletion, or ongoing loss around the transplanted hair.
If the hairline is unnatural, adding more grafts may make the problem worse. The first visible line may still look artificial. The correct plan may involve softening the hairline, removing poorly placed grafts, placing finer grafts in front, or rebuilding the transition in stages.
If the density is weak but the design is good, a limited third procedure may help. Limited is the important word here. Grafts should be placed where they create the highest visual value, not scattered everywhere to create very little improvement in each area.
When the previous surgery caused donor damage, the repair becomes more difficult. A patient may need camouflage, styling changes, scalp micropigmentation, or very selective graft use. Overharvested donor repair is often limited. In some cases, the best surgical answer is not another large extraction. It may be a smaller correction that makes the most visible problem easier to live with.
Bad hair transplant repair is careful and often staged. A repair patient has already paid a physical and emotional price. The next operation must not create another injury in the name of fixing the first one.
Beard or body hair may help selected cases
Beard or body hair can help patients whose case fits, but it does not make a weak plan safe by itself. These hairs can be useful when scalp donor supply is limited, especially for support in the crown or for selected repair work, but they behave differently from scalp hair.

Beard hair can be thicker and stronger, but it may feel different and should be blended carefully. Chest or other body hair can have a different growth cycle, texture, curl, and length. These sources should not become an excuse to spend the scalp donor carelessly.
When beard hair for crown transplant planning or body hair as a donor source is considered, the graft source must improve the plan without making the result look mismatched. In many third surgery cases, beard or body hair is support, not the foundation.
Crown treatment needs stricter priority
The crown is one of the most emotional areas for patients and one of the most demanding areas for surgeons. It can bother the patient because it is visible in photographs, mirrors, elevators, bright rooms, and from above. But surgically, it can require many grafts to produce a change that still looks moderate.
In a third hair transplant, the crown should not be treated automatically. First, the frontal frame must be stable, the midscalp needs enough support, and the donor supply has to afford crown work safely. If the front is weak or the donor is fragile, spending many remaining grafts on the crown may be the wrong priority.
The crown also has a spiral direction. The hair does not simply grow forward. It changes angle around the whorl, and this makes density planning more difficult. A crown that looks thin under strong light may still require a very careful and conservative plan, especially if the patient has limited donor reserve.
Sometimes a small crown improvement is worthwhile. It can reduce the most visible contrast and help the patient feel more comfortable. But the patient must understand that crown hair transplant planning often means improvement, not full coverage. A promise of a dense crown after two previous surgeries should be questioned carefully.
I ask patients to rank what bothers them most in normal life. Is it the frontal hairline in conversation, the midscalp in daylight, or the crown in photographs? This priority matters because the third surgery should spend grafts where they help the patient most.
In many third surgery cases, the best crown plan is moderate. It may be better to create soft visual coverage than to chase density that the donor cannot safely provide.
Medication and future hair loss affect the decision
Future hair loss should never be ignored in a third hair transplant. Transplanted hair may remain stronger than native miniaturizing hair, but surgery does not stop the biology of androgenetic hair loss. If the surrounding native hair continues to thin, the patient may feel that every result becomes temporary.
Medication decisions are personal and should be made with proper medical guidance. Some patients tolerate finasteride, dutasteride, minoxidil, or a carefully chosen plan. Some do not. Some have side effect concerns, medical history issues, or anxiety around medication. The surgical plan must respond to that reality.
If a patient cannot or will not use medical treatment, the third surgery often needs to become more conservative. Aggressive density in unstable areas, an immature hairline, or crown work may be the wrong choice if the loss pattern is still changing.
The question of hair transplant without finasteride becomes even more serious after previous surgeries. The issue is not only the transplanted grafts. Native hair still creates the overall illusion of density.
Future hair loss can make a technically successful transplant look weaker over time. The grafts may survive, but the hair behind them may continue to shrink. This can create gaps, islands, or a result that needs more surgery than the donor can safely provide.
A third surgery candidate needs to be realistic about the next ten years, not only the next twelve months. A plan that looks natural as the patient ages matters more than a density promise for the next year. If the patient is still losing hair quickly, the best decision may be to stabilize, observe, and avoid spending the last reserve too soon.
The plan does not have to force every patient into medication. But it must account for what happens if hair loss continues.
Warning signs before another surgery
The first warning sign is a clinic that promises a large third session without carefully examining the donor. A high graft number may sound reassuring, but in a third hair transplant it can also be a warning that the remaining supply is being treated as unlimited.
The second warning sign is a plan based only on photographs. Photos can help the first conversation, but they cannot replace close examination. Donor density, hair caliber, scalp contrast, scar pattern, miniaturization, and the real behavior of the hair in different lighting all need review.
The third warning sign is pressure. If a clinic uses urgency, discounts, or fear to make the patient decide quickly, the consultation has moved in the wrong direction. A third operation deserves time. It deserves an unhurried review of what happened before and what can still be done safely.
The fourth warning sign is no discussion of alternatives. Sometimes the best plan is not surgery. Sometimes it is medication, observation, a different hairstyle, scalp micropigmentation, or accepting that the donor should not be touched again. A useful consultation should include the possibility of saying no.
The fifth warning sign is treating the crown, hairline, midscalp, and donor supply as separate problems. They are not separate. They are one system. Spending grafts in one area changes what can be done elsewhere.
Two surgeries at different clinics with no clear record of graft numbers, technique, extraction pattern, or growth create extra uncertainty. When that happens, the history has to be reconstructed from the scalp itself. That takes careful examination and realistic limits.
If nobody explains what will be left after the third surgery, the consultation is incomplete. The remaining donor reserve matters as much as the planned graft number.
Another graft number needs donor context
Before accepting another graft number, it helps to know how the surgeon reached that number. A third surgery should not be planned from a quick look or a recycled estimate. The donor reserve, recipient area, hair caliber, previous extraction pattern, and future needs all have to be reviewed together.
This is the same reasoning behind how a surgeon calculates graft number, because patients are often given numbers without being shown the reasoning behind them.
For a third hair transplant, the number must have a purpose. It may be meant to improve frontal density, soften the crown, repair old work, or camouflage a transition zone. A number without a purpose is not a plan.
It helps to know the tradeoff. Sometimes a smaller operation gives most of the visual benefit with less donor risk. Sometimes extra grafts add only a small cosmetic gain while increasing donor depletion.
This is where I want the surgeon’s judgment directly in the plan. The hairline design, recipient area incisions, donor strategy, and decision about when to stop cannot be treated as routine steps. This matters especially for younger patients, diffuse thinners, crown dominant cases, and patients who already used many grafts in the first two surgeries.
One revealing detail is what the surgeon would refuse to do. A clinic that says yes to everything may feel comforting in the moment, but a surgeon who can say no may be protecting you from a permanent donor problem.
The decision can be proceed, wait, or stop
The decision depends on three conditions. Is there a clear benefit? Is the donor plan safe? Is there a realistic end point? If those three conditions are present, the discussion can continue. If one is missing, the plan should not be pushed forward.
You may proceed if the donor remains strong, the previous results are mature, the design is natural, the goal is specific, and the improvement is worth the graft cost. The surgery does not need to be large. In fact, many good third procedures are smaller than the patient first imagined.
You may need to wait if the last surgery is still maturing, if medication has recently changed, if shedding is active, if the crown is still evolving, or if your concern is based mainly on difficult lighting and short hair. Waiting is not failure. Sometimes waiting is the choice that protects the final result.
You may need to stop if the donor is too weak, the expectations are too high, the old design cannot be improved safely, or the remaining grafts would be better saved for a future problem. This can be hard to hear, but it can also be the most responsible answer.
When deciding whether someone is a good candidate for a hair transplant, technical possibility is only the beginning. The safer judgment is whether surgery is wise for that patient, at that time, with that donor reserve and that future risk.
By the third operation, the patient often has fewer grafts left, more emotion invested, and less tolerance for another mistake. The plan should become smaller and more exact instead of chasing a bigger number.
Think of it practically. If another surgery can make your result more natural, more stable, and easier to live with while protecting the donor, it may be worth considering. If it only gives a temporary feeling of action while spending grafts you may need later, it is not the right plan.
The third surgery should leave you with a more stable result, not more dependence on future correction. The strongest result is not the most dramatic promise. It is the result that still looks natural years later, under normal light, with realistic hair length, and with a donor that was respected.