Thin Hair Transplant Results Have Different Causes
A hair transplant can look thin for several different reasons. Sometimes the result is still maturing. Sometimes harsh light, wet hair, fine hair, strong scalp contrast, or a wide treated area makes the scalp show more than expected. Sometimes the donor area could not safely support more density. And sometimes the surgical plan or execution really was weak. A separate review of blonde and red hair transplant planning helps patients understand when lighter color helps softness and when fine caliber still limits coverage.
The first job is not to decide good or bad from one close photo. The first job is to separate normal visibility, patient-specific limits, and true surgical weakness. Those situations can look similar when you are worried, but they lead to very different decisions.
I also want the comparison to be fair. Compare the result with hair transplant results from hair like yours, not with a polished gallery case from a different donor area, hair shaft thickness, curl, skin contrast, pattern of loss, and coverage goal.
First Separate Normal Visibility From a Real Weak Result
Once a person starts studying hair transplants, he begins to see details he never noticed before. The first millimeters of the hairline, the spacing between hairs, the way light reflects from the scalp, and the difference between dry hair and wet hair all become more obvious.
That new awareness does not mean the concern is fake. It means the concern needs better sorting. A transplant can look slightly airy in difficult conditions and still be a good result. Another transplant can look thin because the donor was limited, the hair was fine, or the area was too broad. A third result can look thin because the clinic spread grafts badly, rushed the recipient area incisions, overused the donor, or created a hairline that looks artificial.
The useful split is simple. If the hair looks natural in normal daily life but shows some scalp when wet, parted, flattened, or placed under bright overhead light, that is different from a mature result that looks transparent, row like, patchy, or unnatural in ordinary conditions too.
Scalp Visibility Is Not the Same as Failure
Some scalp visibility does not prove a failed transplant. Hair is not a solid sheet. It moves, separates, reflects light, and changes with length, moisture, styling, and angle. Native hair can show scalp under strong light as well, especially when it is short, wet, or pulled apart.
The whole impression matters when a result looks thin. Does the hair frame the face? Is the front soft enough? Does the result suit the patient’s age and likely future hair loss? Does it look acceptable at normal social distance, or only in one carefully arranged photograph?
Many worried patients test a transplant in ways they never tested their original hair. They stand under bathroom light, wet the hair, pull it apart, take close photos, and then compare that image with a clinic’s best after photo. That kind of test can reveal a real weakness, but it can also exaggerate a result that is still reasonable.
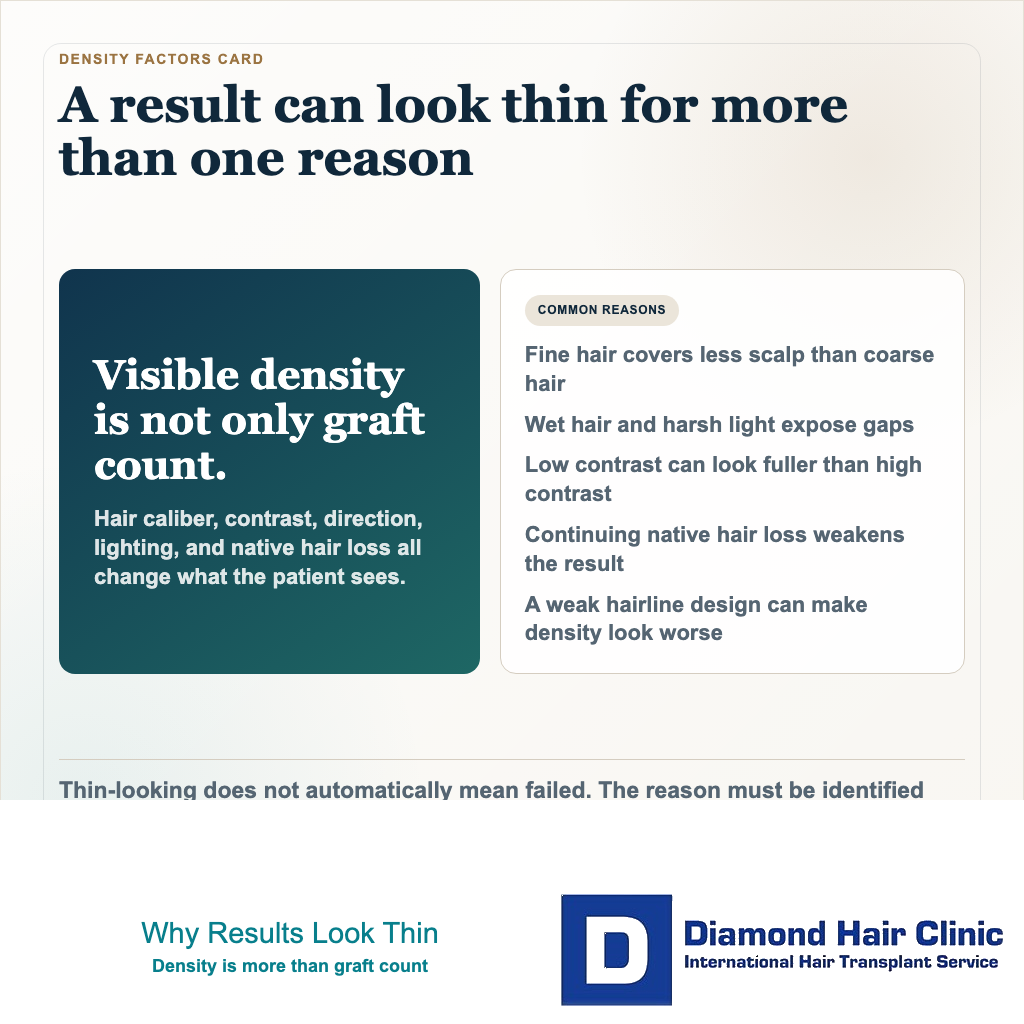
Graft Number Is Only One Part of Visible Density
Many patients think density is mainly a graft number question. The number matters, but it is not the full explanation. Visible density comes from graft count, hair count inside each graft, hair shaft thickness, curl, color contrast, recipient area size, angle, direction, distribution, and native hair support.
Visual density can be misleading when it is reduced to one figure. The same density can look strong in a compact frontal zone and weak when it is stretched across a large frontal, mid scalp, and crown area.
Distribution matters just as much. If grafts are placed in obvious rows, or if too much area is treated with too little priority, the scalp can look more see through even when the total graft count sounds acceptable. A number can impress on paper and still fail in the mirror.
Hair Type Can Make a Good Result Look Lighter
Hair caliber is one of the biggest reasons two good surgeries can look different. Coarse hair gives more visual coverage than fine hair. Wavy or curly hair often overlaps the scalp better than very straight hair. Lower contrast between hair and skin usually hides spacing more easily than dark straight hair on pale skin.
A patient with fine hair, very straight hair, and strong scalp contrast may show more scalp even if the grafts grew well. Another patient with thicker, wavier, lower contrast hair may look fuller with a similar or even smaller graft number. That difference may come from the starting material, not from a better surgical plan.
Result comparisons need context. Before judging a case, I want to know the hair shaft thickness, curl or straightness, scalp contrast, donor strength, size of the treated area, and whether the crown or mid scalp was included. Without those details, many comparisons become unfair from the beginning.
Donor Limits Can Make a Responsible Plan Look Less Dense
A hair transplant does not create new hair. It redistributes a limited supply from the donor area. Once grafts are removed, they are gone from that exact donor location. So the donor area has to be treated like a lifetime budget, not an endless supply.
Sometimes the responsible plan is not the densest plan a patient imagines. In a broad Norwood 4, 5, or 6 pattern, the donor may not be strong enough to create high density across the hairline, mid scalp, and crown without leaving the donor area thin or patchy later.
That can be frustrating, but it is important. A careful surgeon may deliberately build a stronger frontal frame, protect donor reserve, and avoid chasing fantasy density everywhere. The result can look lighter than the patient emotionally hoped, yet still be more responsible than an aggressive plan that damages the donor and still fails to look full.
There is a difference between underplanning and disciplined planning. Underplanning leaves the important visual problem unresolved without a good reason. Disciplined planning improves what matters most while protecting the donor area and future options.
If the first operation built a stronger front but left the mid scalp or top visibly transparent, the next question is whether a second transplant can help a thin top after hairline surgery without wasting donor reserve.
A Hairline That Looks Thin May Be a Design Problem
Many people describe a hairline as thin when the real problem is design. The eye judges the front edge first. If that edge is too straight, too sharp, too low, too repetitive, or too dense in the wrong way, the whole result can feel weak even if many grafts survived.
At the hairline, I want single hair grafts at the front, a soft transition behind them, natural direction, and controlled irregularity. A natural hairline should not look like a drawn border. The recipient area incisions have to respect angle, direction, density distribution, and the patient’s face.
Rows are especially damaging here. A row like pattern is not only a density issue. It is a pattern issue. The scalp may look more transparent because the eye reads repetition instead of natural variation. That is where hairline design and recipient area planning become central.
If the mature result is thin because the design is artificial, simply adding grafts may not be the right first answer. A repair review has to define whether density, angle, hairline position, graft type, donor damage, or several issues together are driving the thin look.
Harsh Light and Wet Hair Need a Fair Test
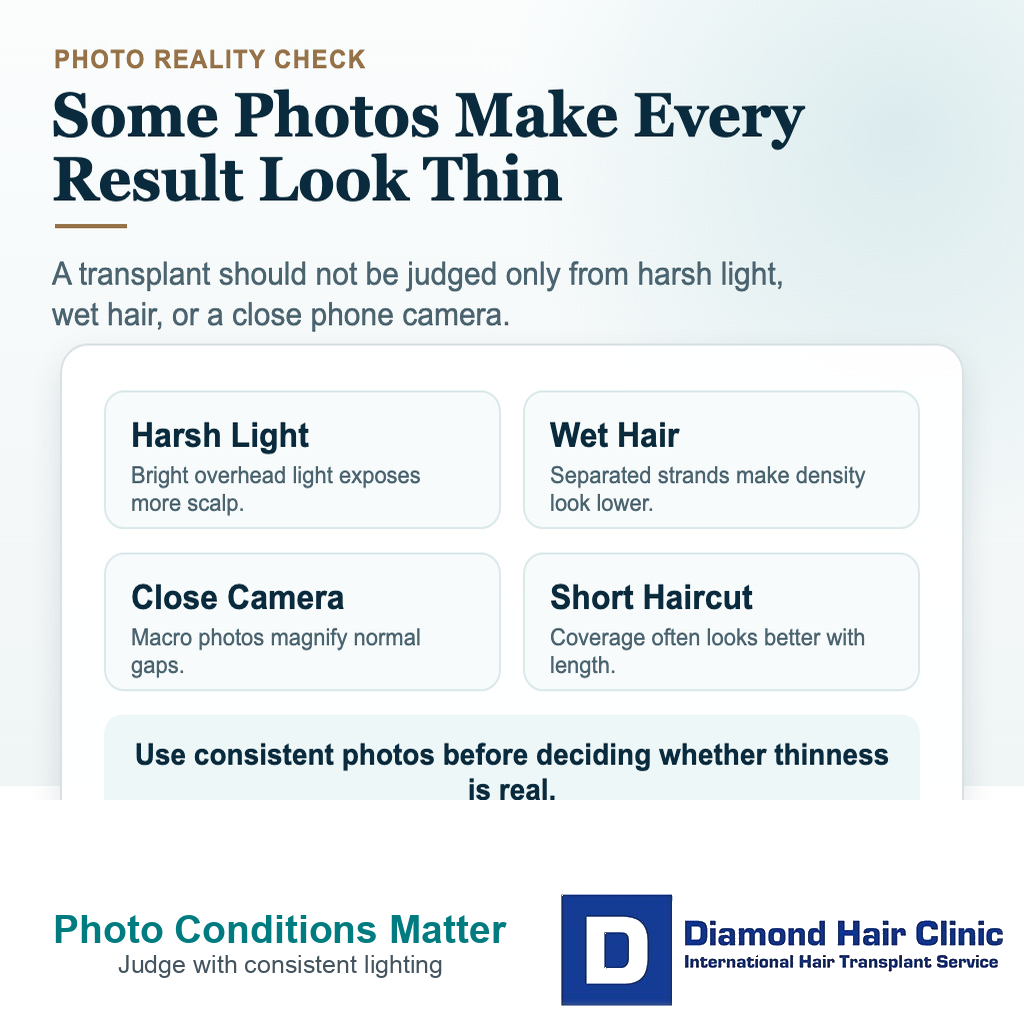
Wet hair clumps together and exposes more scalp. Flat hair shows more spacing than textured hair. Strong overhead light reflects from the scalp. Short hair gives less overlap. A close phone photo can make a normal amount of spacing look dramatic.
Those conditions are useful for inspection, but they should not be the only way a result is judged. The fair test is dry and wet, styled and unstyled, normal room light and daylight, close view and normal social distance. A single harsh image is evidence, not a verdict.
The concern becomes stronger when the result only looks acceptable in perfect styling, soft light, or one flattering angle. The same principle sits behind harsh light and wet hair. A good result does not need impossible density, but it should not collapse completely the moment conditions become ordinary.
Native Hair Loss Can Weaken the Background
Sometimes the transplanted grafts are not the main reason the result looks weaker. The native hair behind, between, or around the grafts may still be miniaturizing. When that background hair declines, the whole area can look lighter even if many transplanted hairs are still present.
A transplant that looked well blended at first can later look more separated as native hair changes. Surgery moves donor hair into the recipient area, but it does not freeze the rest of the scalp. The native hair can continue to thin with androgenetic hair loss.
Medical treatment may be part of the discussion when the patient is suitable. Finasteride, dutasteride, minoxidil, PRP, or other support options are not the same decision for every patient. If a patient wants a hair transplant without finasteride, I still need to plan around the possibility that vulnerable native hair may keep changing.
The key distinction is graft survival versus native hair progression. If you do not separate those two, you may blame the transplant for a change caused by hair that was never transplanted.
Early Growth Needs Timing, Not Panic

Early growth can look thin, uneven, and immature. The hair does not return in one smooth line. Some areas start earlier, some look quiet longer, and early hairs often need time to gain length, caliber, and texture.
A low density look at 4 months is not judged the same way as a mature result. At 6 or 7 months, I look for movement, new fine hairs, better coverage in the same lighting, and whether the same weak area is slowly changing. A patient who is still thin after 7 months needs trend review, not automatic repair planning.
For many frontal and mid scalp cases, the 12 month point gives a much clearer judgment. Crown work, slow growers, and texture changes can need closer to 15 to 18 months before the final density judgment is fair. Waiting does not mean ignoring bad signs. Static empty areas, unhealthy skin, visible rows, wrong direction, donor damage, or an unnatural hairline still deserve review.
The timing question is whether the result is changing. Slow improvement is different from no meaningful movement. A result that keeps improving should not be treated the same as a result that looks structurally wrong.
Use the 10 thin result sorting slides below to separate timing, harsh light, wet hair, hair caliber, scalp contrast, donor limits, coverage area, hairline design, native hair loss, and the evidence to send before repair talk. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.