


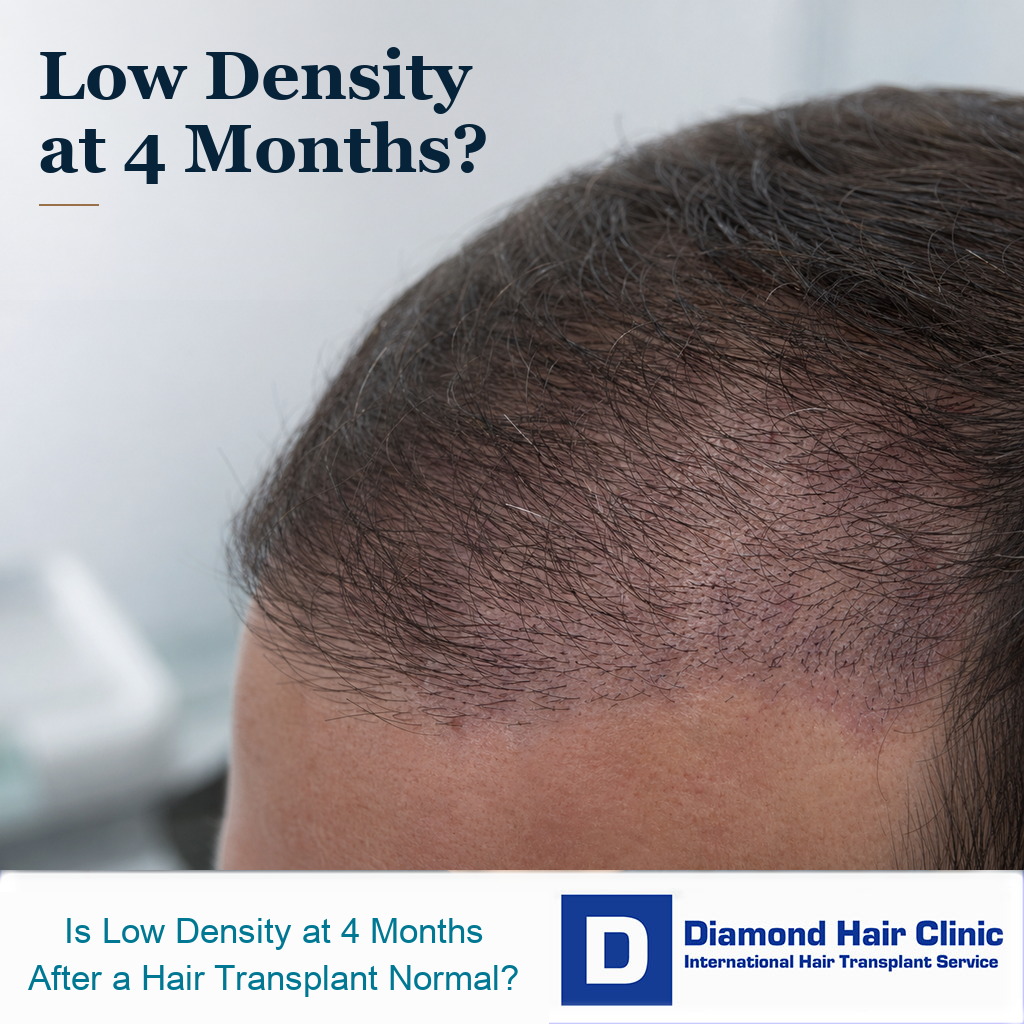
Low Density at Month Four and Growth Trends
At four months, many patients are still between shedding and visible growth, so one bad mirror moment can exaggerate the concern. This is different from looking sparse after the first wash, which belongs to the early healing period. It is also different from early native hair shock loss after FUE, where existing recipient hair may shed around the transplanted zone.
Month four is still early for final density, even though it is late enough for you to expect some proof that growth has started. It is a trend checkpoint, not a verdict. At this point, the useful question is whether the area is beginning to wake up, whether the skin looks healthy, and whether the pattern is improving from month to month.
If you are comparing the next checkpoint, a month five hair growth check should still focus on trend, skin calmness, and new short hairs rather than final density.
This is the stage when many people start checking too closely. You may compare both sides of the hairline, take photos under strong bathroom light, or worry that one area already looks too thin.
The right response depends on the recipient area, how the grafts were placed, how the donor area was used, whether native hair is stable, and whether the pattern is improving rather than staying completely inactive. If the original concern was the day one placement pattern, compare this with graft rows after FUE instead of judging density alone.
Fine early sprouts in healthy skin are very different from no visible activity, heavy inflammation, or a day one pattern that already looked sparse. Later, if the new transplanted hair feels wiry or coarse, that is also a different assessment from early low density at month four. If the question is whether those sprouts are baby hair, retained stubble, or native miniaturization, review baby hairs after a hair transplant before judging density.
The month number matters, but the clinical picture matters more. The review should look at where the thinning is, whether the area was densely implanted, whether native hair was present there, and whether the concern is graft emergence, weak visual coverage, or ongoing native hair loss around the grafts.
Panic photos alone are not enough to judge a transplant at month four. Even so, not every concern should be dismissed with one generic reassurance. Some cases need time. Others need a proper review of the surgical plan, day one placement, and healing course before reassurance means anything.
Month four often feels uncertain
Month four is difficult because it sits between the ugly stage and the visible improvement stage. You are no longer immediately after surgery, but you are still far from the final result.
By this time, most early scabs are gone, redness may be softer, and you may already have lived through shedding, or worried because there was almost no shedding after the transplant. Naturally, you want visible proof that the operation worked.
This is when the mind becomes very sensitive. One side may look stronger. One temple may appear empty. The hairline may look thin in photos even while tiny new hairs are starting to emerge.
Comparing yourself with someone else’s month four photo can mislead you. Hair caliber, graft number, hair color, skin contrast, curl, medication use, and photography conditions all change what early density looks like.
The ugly duckling phase does not end on the same day for everyone. Some patients start looking better early. Others stay visually awkward for longer and then improve strongly later.
The emotional problem is that month four gives you just enough growth to judge, but not enough growth to judge fairly. That gap creates a lot of unnecessary fear.
Friends and family can make this stage harder. They may expect the transplant to look better already, and a casual comment can make you feel that something is wrong.
Most people around you do not understand the growth cycle. They see a cosmetic procedure and assume the visible change should be quick. Hair transplantation does not work that way.
You also become more skilled at detecting problems after surgery. Before the transplant, you may not have noticed small differences between the left and right hairline. After surgery, every shadow, thin patch, and uneven angle can feel important.
The scalp is still in an early growth stage
After a hair transplant, many transplanted hairs shed before the new growth begins. This shedding can be frightening, but it is a common part of the process.

The early phase is part of shedding of transplanted hair. For this question, the key point is that the visible hair shaft can fall while the follicle remains alive under the skin.
At month four, many follicles are only beginning to wake up. Some may already be producing visible hair. Some may be producing very fine hairs that are easy to miss. Some may not be visible yet.
Early hairs are usually thin, short, and soft. They do not yet have the caliber, length, or texture that gives real coverage. You may see hair starting and still feel disappointed with the density.
Density at month four is not judged only by counting visible hairs. Small emerging hairs, healthy skin, appropriate direction, and monthly change all matter more than one close photo.
Hair transplant growth does not switch on all at once. It returns slowly. The result usually builds through several stages, and the early stages rarely look elegant.
At month four, the new hairs may not yet behave like normal hair. They can stand in odd directions, appear wiry, or look softer than the surrounding native hair. This can make the density look worse than it really is.
Scalp condition also matters. Quiet skin with mild dryness is very different from skin with repeated pimples, crusting, heat, pain, or irritation. The skin environment does not tell the whole story, but it helps show the healing quality.
Sometimes the weak point is not low graft growth. It may be native hair shock loss or continued native hair miniaturization around the grafts. That is a different problem, and it needs a different conversation.
Use the carousel below to judge density by timing, hair caliber, photo consistency, scalp health, native hair changes, original plan context, zone differences, and repair timing. Swipe the carousel, use the arrows for one step at a time, or choose a number below the image to jump to that point.
A fixed density percentage is not useful at month four
A fixed percentage such as 40 percent or 50 percent of the final result is too crude for month four. Some people show visible early growth by then, while others only have fine short hairs that do not create real coverage yet.
The deciding detail is whether the scalp is healthy, whether tiny new hairs are appearing, whether the weak area matches the day one placement, and whether the trend from month four to month six is moving forward.
If there is almost no visible growth at month four, I still do not call the result failed automatically. The area should be documented, compared with day one photos, and watched carefully over the next two to three months.
Without meaningful change by month six, or when one area remains completely inactive while other areas improve, the review should become more detailed. The distinction is whether a hair transplant has failed or is being judged too early. A month six density check gives that next comparison point before repair planning becomes serious.

One side can grow slower than the other
Uneven growth is one of the most common reasons for panic. You may see the left side growing while the right side looks empty, or feel that one temple has more hairs than the other.
Often, this difference is temporary. Hair follicles do not all restart evenly. Even in the same scalp, one zone may wake earlier while another zone catches up later.
There are also technical and anatomical reasons why zones can behave differently. The skin may have healed differently. The angle of lighting may expose one side more. You may part the hair in a way that makes one side look weaker.
False reassurance is not helpful either. If one area had noticeably fewer grafts placed, if the day one photos showed a gap, or if there was trauma, infection, necrosis, or severe crusting in one zone, then uneven growth deserves closer review.
The useful detail is not to panic from one photo. The useful detail is to compare consistent photos over time and understand whether the weaker side is slowly improving.
If a weaker side remains completely inactive while the other side continues to develop, clear photos and surgical details become important. Timing matters, but documentation matters too.
Another detail is easy to miss. The two sides of the hairline may not have had the same starting condition. One side may have had more native hair, more miniaturized hair, or more empty skin before surgery.
If one side had weaker native hair before the operation, it may look worse during recovery even if the transplanted grafts are growing. What looks like an uneven transplant can partly come from the original pattern.
Before surgery photos are important. Without them, you and the clinic may argue from memory, and memory is not reliable when emotions are high.
Low density can still look normal at month four
At month four, thin coverage can still look normal when small new hairs are visible, the scalp is healthy, and the overall trend is moving in the right direction. You may dislike the appearance, but the biology may still be on schedule.
At this stage, I expect many hairs to be fine. I expect imperfect coverage. I expect the result to look weaker under harsh light, with wet hair, or when the hair is cut too short.
I do not reduce this to whether the result looks dense yet. I first look for signs that early growth has started and that the recipient area still looks capable of continuing to mature.
This month four concern connects to the broader question of why some hair transplant results look thin. Density is not only about the number of grafts. It is also about hair shaft thickness, curl, color contrast, placement angle, and native hair support.
If you have fine hair, dark hair against light skin, or a large recipient area, early growth may look thinner than expected. That does not necessarily mean the operation failed.
In most cases, months five, six, seven, and eight are much more informative than month four. The result begins to gain more visual weight as the hairs lengthen and thicken.
It is also normal for the first hairs to look scattered. The eye wants a continuous wall of coverage, but early growth usually appears in small irregular areas before it blends together.
At this stage, I would not reduce this to whether the area already looks full. It is whether the process has started. A thin beginning can still become a much stronger result.
For many patients, month four is closer to the opening phase than the final result. Understanding that makes the waiting period less frightening without pretending every concern is meaningless.
Signs that need more caution at month four
The pattern becomes more concerning when the weak area matches an obvious planning problem. For example, if the graft placement looked sparse from the beginning, the final density may also be limited.
Early photos can be very useful. If we can judge a hair transplant from day one photos carefully, we may understand whether the weak point is delayed growth or whether the original implantation pattern was too light.
Severe infection, black scabbing, major trauma, aggressive picking, or prolonged inflammation in the recipient area also changes the conversation. These are not small details. They can affect healing and possibly growth.
Another concern is a mismatch between the promised result and the actual surgical plan. If a clinic promised very high density but spread a limited number of grafts across a large area, you may be expecting something the surgery never had the ability to produce.
A result that ages well depends on more than early coverage. It depends on natural design, donor preservation, appropriate density, survival, hair direction, and how well the plan fits the future hair loss pattern.
Patience is important, but patience should not be used to hide poor planning. You can wait for biology while still collecting proper photos and asking clear questions.
A clinic that refuses to discuss the concern at all is another warning sign. An ethical clinic should not promise that every problem will solve itself without looking at the case. A proper review is part of responsible medical practice.
Sometimes the issue is not graft survival but design. A hairline can grow and still look weak if the grafts were placed too far apart, if the transition zone is poor, or if the front was lowered too aggressively for the available donor supply.
Separate growth from density. Hair may be emerging while the density still looks low because the hairs are short, fine, and not yet layering. That is different from a mature result where the hair has grown but the graft distribution was too light for the size of the area.
Photos, lighting, and hair length need consistency
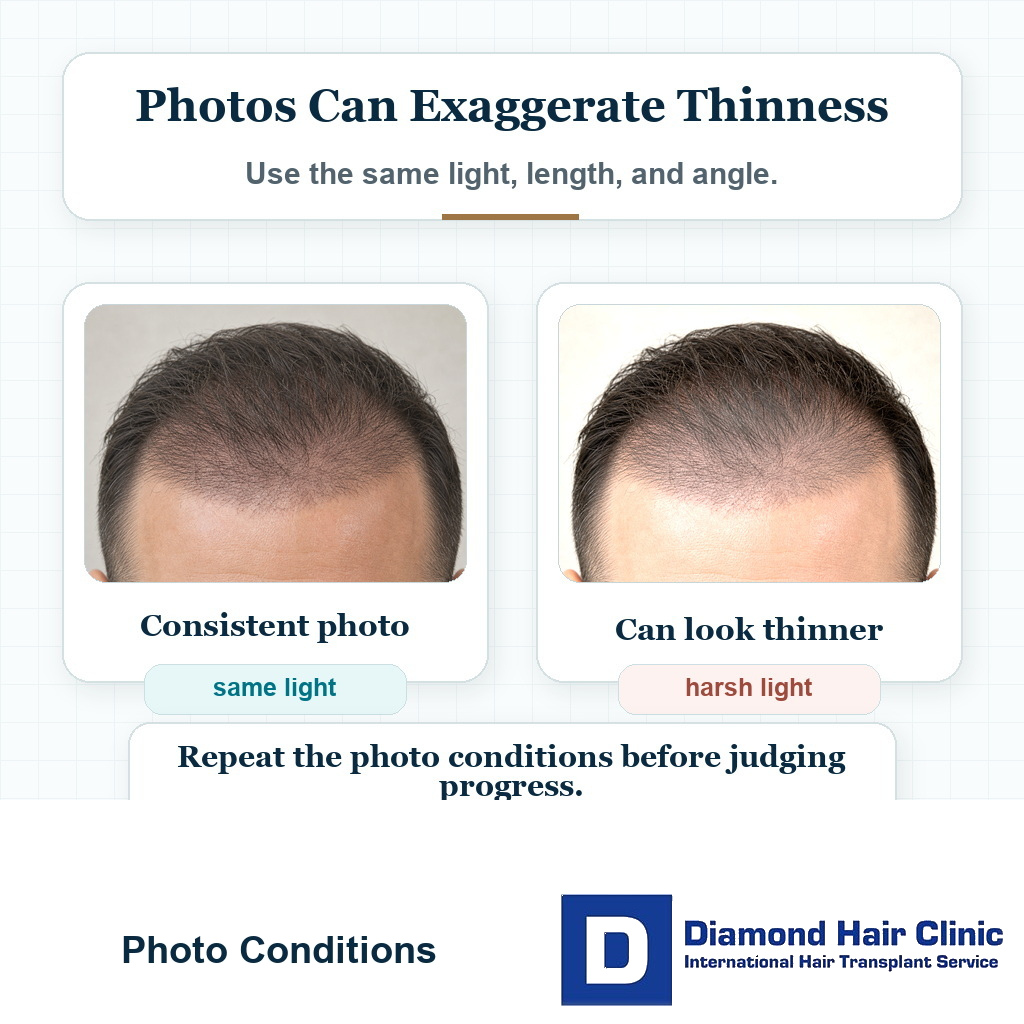
At month four, photos can be useful, but they can also create unnecessary panic. A hair transplant at month four may look acceptable in soft daylight and very thin under a bathroom spotlight.
Wet hair is even more unforgiving. When hair is wet, the strands separate, the scalp reflects light, and early density looks weaker. This does not always represent how the hair will look in normal daily life after maturity.
Take consistent photos. Use the same room, same light, same distance, same hair length, and same angles. Random photos taken under different conditions are very difficult to compare.
That problem is part of harsh light and wet hair. The short version is that light can expose every limitation, especially before the hair has thickened.
Hair length also matters. Very short hair can make low density more obvious because the hairs do not overlap enough to create coverage. Longer hair, when grown naturally, may improve the visual effect without any new follicles appearing.
For month four, steady documentation is better than obsessive inspection. Take photos every few weeks, not every few hours. The scalp changes slowly, and the mind can become exhausted from checking too often.
Photos with the hair dry and gently combed are more useful than a single wet close up. Even a reasonable early result can look frightening when the flash is too close to the scalp.
Progress should be compared like with like. A dry photo in soft daylight should be compared with another dry photo in similar light. A wet photo under a strong light should not be used as the only evidence of failure.
Ten emotional photos from ten different angles often give less information than one consistent photo set. The purpose is to see the trend, not to punish yourself with the harshest possible image.
The crown usually needs more patience than the front
Crown hair transplant planning needs more patience than the front. The crown can look thin from above even when growth is happening, because the whorl pattern opens the hair in different directions.
The crown also consumes many grafts for a modest visual change. A small improvement can matter, but it may not look as dramatic as frontal hairline restoration.
At month four, crown growth can be especially disappointing because the hairs are short and cannot yet layer over the curved scalp. The lighting from above makes this worse.
If the crown was treated with limited grafts, the original goal matters. Sometimes the goal is improvement, not full coverage. Sometimes the front was prioritized, and the crown was intentionally left lighter.
Medication and native hair stability also matter in crown cases. If the surrounding crown hair continues to miniaturize, the transplant may grow while the overall area still looks weak.
The crown may improve later, but it needs judgment with a different standard from a small hairline case. A crown that looks thin at month four does not carry the same meaning as a mature crown that still has poor coverage.
The crown also changes dramatically with hair length. Very short hair in the crown may reveal scalp even when there are many growing hairs. Slightly longer hair can create more layering and make the same area look stronger.
Expectation also matters. A crown transplant should rarely be planned as a return to teenage density, especially when donor supply must also protect the frontal area and future needs.
Practically, the crown is a strategic decision. If too many grafts are used there too early, there may be fewer options later when the front or mid scalp needs support.
Between month four and month eight
Between month four and month eight, the useful work is steady follow up. Take clear monthly photos, keep the scalp healthy, and avoid harsh styling, heavy cosmetic products, or using hair fibers too early if they make you rub, scrub, or inspect the area more.
If medication was part of your plan, do not change it randomly during this emotional period. Native hair stability can affect the final appearance around transplanted hairs. That same judgment applies to medication before a hair transplant.
Minoxidil, finasteride, dutasteride, or another medical treatment should be reviewed with a qualified doctor. Starting, stopping, or changing doses because of anxiety can make the timeline harder to understand.
Between month four and month eight, the hair usually gains more length and caliber. Some people see a major change around month six. Others improve more gradually toward month nine or month twelve.
Do not schedule a repair too early unless there is a serious complication or an obvious technical problem. Month four may justify documentation and a careful review. It usually should not justify a repair deposit or a second surgery plan. A premature repair plan can lead to unnecessary donor use and emotional decision making.
The better approach is to document, wait, and reassess at meaningful milestones. For many people, the story at month four is not the final story.
During this period, scalp health matters. Treat dandruff or irritation, and ask for guidance if bumps that look like folliculitis appear. A clean, quiet scalp makes follow up easier and reduces unnecessary worry.
Nutrition, sleep, smoking habits, and general health also influence how you feel during recovery. They may not magically create graft growth, but poor general habits can make healing and anxiety worse.
Weekly comparison is usually too tight. Hair grows slowly, and weekly checking often creates the illusion of no progress. Monthly comparison is more realistic.
Repair discussions need more growth evidence
You should talk to your surgeon earlier if there are warning signs. These include persistent inflammation, pain, infection, black scabbing, obvious gaps in the original placement pattern, or a donor area that looks aggressively depleted.
You should also ask for a review if one area shows no meaningful progress over several months while other areas improve clearly. This does not always mean failure, but it deserves documentation and explanation.
For most cases, the need for a second procedure needs judgment closer to the mature result. The hair needs enough time to show its real density, texture, and survival.
If the result remains thin after maturity, the next decision is not simply whether a second hair transplant is worth it. The first question is whether the donor area can support another surgery and whether the original problem can be improved without creating a new one.
Repair planning must be more careful than first surgery planning. There may be scar tissue, unusual angles, depleted donor zones, or a hairline that needs correction before adding density.
At month four, low density often deserves patience. At month twelve, persistent low density deserves a serious explanation.
Wait long enough for biology, but not so passively that poor planning escapes review. Your surgeon should help you understand the difference.
If you are at month four now, do not make an emotional decision from one bad mirror moment. Document properly, keep communication open with your clinic, and judge the result at the right time.
Intelligent context still matters. The number of grafts placed in the weak area, whether the area was fully bald or mixed with native hair, whether healing problems occurred, and whether the donor was used responsibly all affect how the result should be read.
These questions are not signs of panic. They are signs that you are taking the result seriously, and that kind of clear thinking belongs in proper follow up.