



Seborrheic Dermatitis and Hair Transplant Surgery
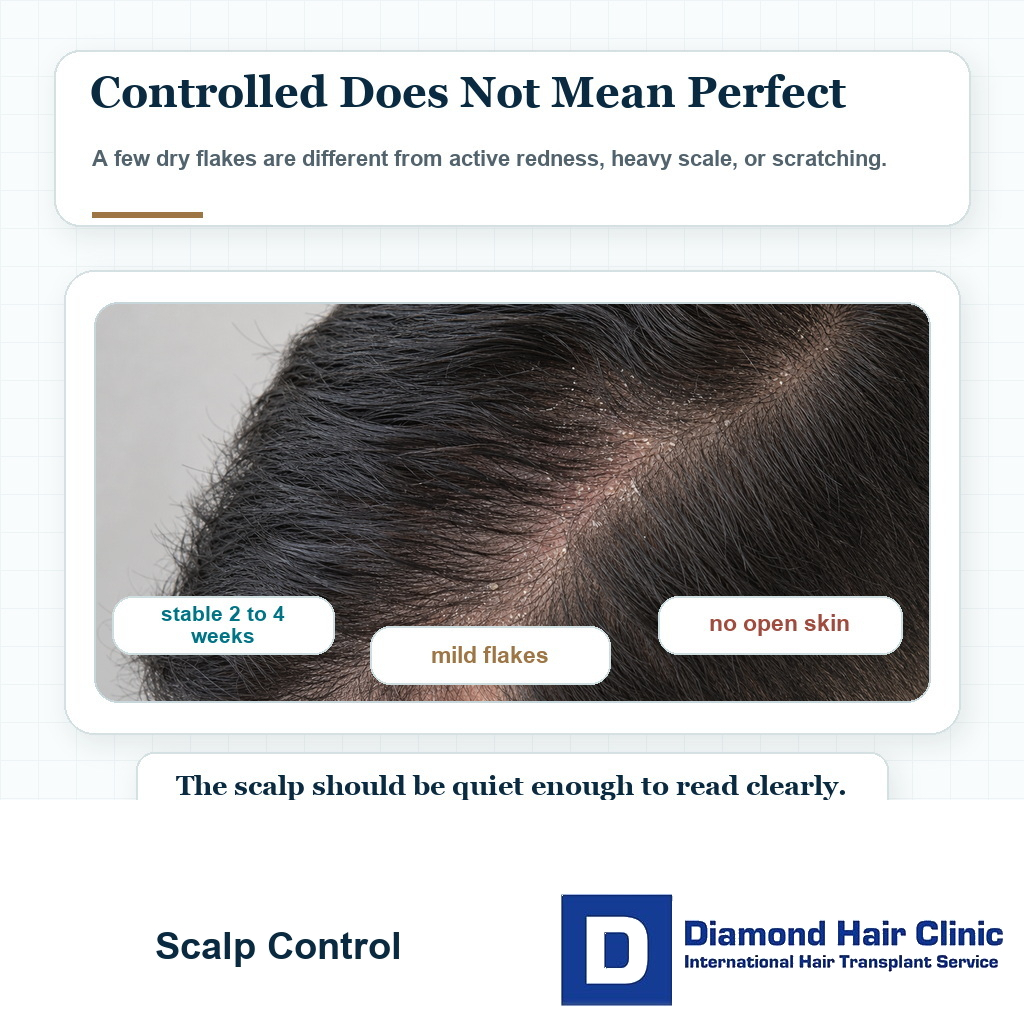
A hair transplant may be possible with seborrheic dermatitis, but not through an active flare. Mild, controlled flakes are different from heavy scale, redness, broken skin, crusting, infection, or itching that makes you scratch. Similar caution applies when I assess scalp eczema, because the real surgical question is whether the skin is quiet enough for surgery.
In most cases, the scalp should stay settled for at least 2 to 4 weeks before surgery. After surgery, strong medicated or dandruff shampoos should usually stay away from the recipient area for the first 14 days. Stronger or prescription products often need a longer pause, sometimes closer to 3 to 4 weeks, unless there is a clear medical reason and the clinic has instructed otherwise.
The diagnosis is only the starting point. If scaling or broken hairs raise a fungal concern, tinea capitis before hair transplant needs treatment before graft planning rather than a routine dermatitis assumption. I need to see whether your scalp is stable enough for clean surgery, careful graft placement, and predictable healing. I apply a similar timing principle when discussing hair transplant with vitiligo, but the concern there is pigment stability rather than flakes or oiliness.
Seborrheic dermatitis is common and tends to come and go. Many patients live with it for years before thinking about surgery. Some have only mild flakes. Others have redness, oiliness, itching, thick scale, and repeated flares that make the scalp reactive.
The condition does not have to disappear forever before surgery. The plan is built around control, timing, and maintenance, because seborrheic dermatitis can settle and then return when the scalp routine is poor or the skin becomes irritated again.
On examination, the condition of the scalp matters more than the name of the condition. A settled scalp and an inflamed scalp are very different surgical situations. Recent dye or bleach can change that examination, so hair dye before hair transplant belongs in the same scalp readiness discussion before surgery.
Scalp condition control before surgery
The condition should be controlled before surgery. I do not need a perfect scalp, because real skin is rarely perfect, but I do need the scalp quiet enough for safe planning and clean graft placement.
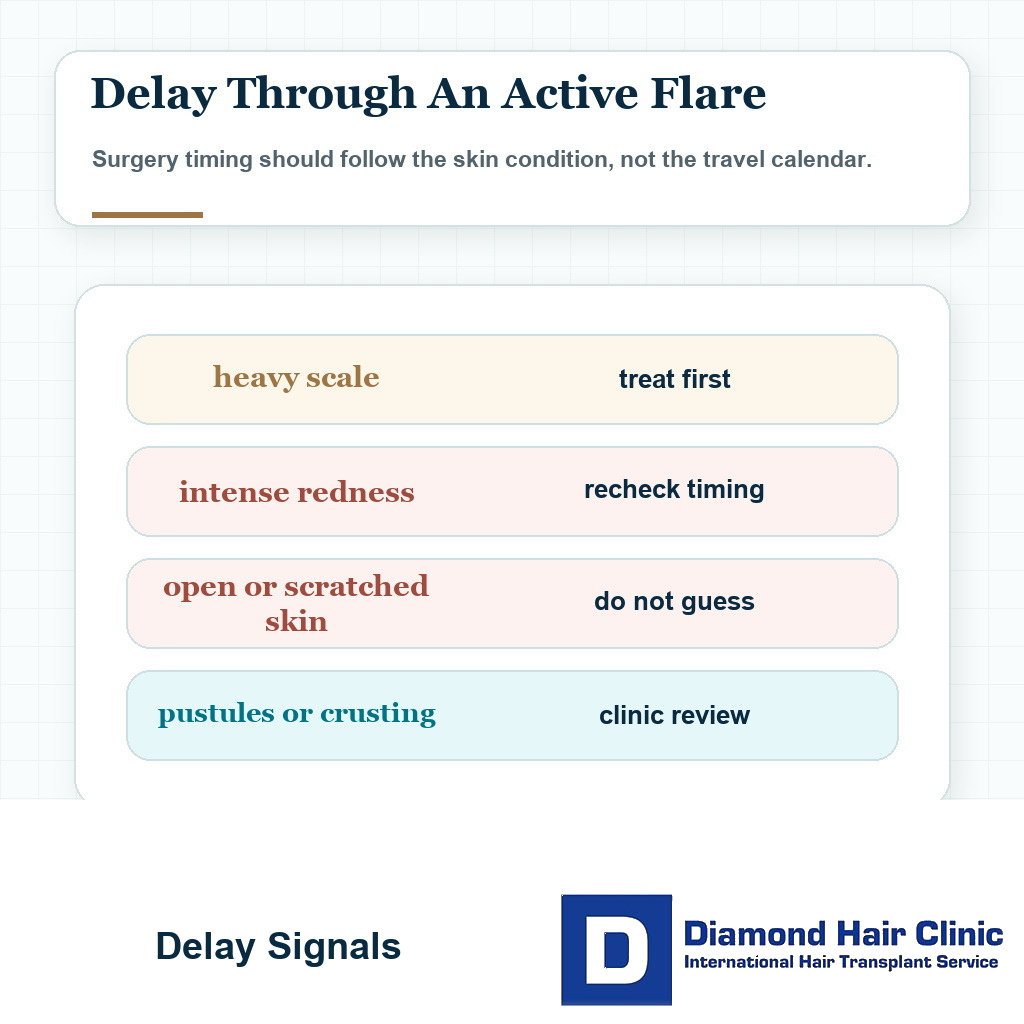
In consultation, the signs I look for include active redness, thick scaling, tenderness, scratching marks, folliculitis, oily crust, and infection. If these signs are strong, the wiser decision is usually to treat the scalp first. When crusting and pustules come with patchy scarring loss, I do not treat it like dandruff. folliculitis decalvans timing before hair transplant becomes the safer reference point.
This is part of candidacy in general. A patient may want surgery, but the surgeon has to decide whether the timing is right. That same timing question is part of deciding who is a good candidate for a hair transplant.
A few dry flakes after shampooing are not the same as an active seborrheic flare. The concern rises when flaking comes with redness, oiliness, soreness, constant itching, pustules, broken skin, or heavy scale. Stress, unsuitable products, sweating, oil buildup, and overtreatment can all make a reactive scalp worse. If the main symptom is itch, I use the same timing logic explained in itchy scalp before hair transplant surgery before deciding whether the skin is ready.
If you come to surgery with an irritated scalp, you may also be more likely to scratch, rub, worry about redness, and misread normal healing signs. A controlled scalp does not guarantee the outcome, but it removes one avoidable source of confusion.
The practical decision is direct. Do not rush surgery on a scalp that is already asking for medical attention. Treat the skin first. Then plan the hair transplant.
Scalp control before surgery
Before surgery, I like to see a scalp that has been stable for at least 2 to 4 weeks. That point does not mean zero flakes under every lighting condition. It means no aggressive flare, no open areas, no heavy scaling, and no constant urge to scratch.
If you cannot stop scratching for one day, that matters. If you need strong shampoo every day or the scalp becomes red and flaky very quickly, that also matters.
Before committing, be clear about the dermatitis pattern. Bring the details that change surgical timing, including whether it is controlled with a simple routine, whether it affects the donor area, recipient area, or both, and whether minoxidil, fibers, styling products, or sweat tend to trigger it.
If the rash also affects the eyebrows, ears, beard area, or sides of the nose, share that with the clinic. Those areas do not decide the surgery by themselves, but they help me understand the condition’s pattern and how reliable the current treatment routine is.
The consultation should happen before travel or payment decisions. A patient who is unsure whether their scalp is ready should not be pushed into surgery by sales pressure. This broader preparation mindset is part of what to know before you book a hair transplant.
Sometimes dermatology input before surgery is the right step. This is not a rejection. It is good planning. You should arrive for surgery with the scalp in its best possible condition.
A delay of a few weeks can feel frustrating, especially if travel is already in your mind. In reality, a delay that improves scalp health can protect the whole operation. A better timed surgery is usually more valuable than a faster surgery.
Dandruff, itching, and graft survival
Mild controlled dandruff by itself does not necessarily mean the grafts will fail. But strong inflammation, heavy scratching, infection, and poor aftercare can create problems that no serious surgeon should ignore.
Graft survival depends on many factors. These include graft quality, handling, placement, blood supply, recipient area condition, donor management, aftercare, and the general health of the scalp. The diagnosis is only one part of the picture.
Every flake does not kill grafts. That would be too dramatic and not clinically useful. But an inflamed scalp should not be ignored either.
The recipient area needs a stable environment for implantation and healing. If the skin is inflamed and you are scratching, the early recovery becomes less predictable. The weaker point is not only biological. It is also practical, because itching can lead to touching, rubbing, and accidental trauma before the grafts have settled.
Aftercare matters even more in these patients. Hair transplant aftercare protects the early healing period, especially the first 10 to 14 days.
The donor area also needs checking. The back and sides of the scalp can be involved too, not only the top. If the donor skin is irritated, extraction and healing deserve extra caution.
The case cannot be judged from one word like dandruff. The real questions are what kind of flaking it is, how severe it becomes, how often it appears, which zones are involved, and what you tend to do when it itches.
Flares that should delay surgery
Surgery should usually be delayed if there is heavy scaling, intense redness, open skin, bleeding from scratching, pustules, crusting, infection, strong pain, or uncontrolled itching. Recent treatment changes also make me cautious when the patient does not yet know whether the scalp is improving or worsening.
Another reason to delay is uncertainty. If a patient cannot tell the difference between normal flakes and an active flare, careful scalp examination or dermatology input is better than guessing.
Timing matters too. If a flare appears very close to surgery, you may be tempted to apply strong products aggressively in the final days. That can irritate the skin further. It can also create dryness, redness, or sensitivity that complicates the surgical field.
A stable scalp before surgery gives everyone a clearer picture. It makes the operation and the early recovery easier to read.
If the scalp is actively inflamed, surgery becomes less clean from a planning point of view. The density plan may be harder to judge, the skin response may be more reactive, and you may become anxious over every crust, flake, and red spot afterward.
Some patients try to hide the condition because they fear the clinic will cancel the operation. That is a mistake. It is much harder for me to protect a scalp problem I do not know about.
If the condition is active, tell your surgeon before surgery. A careful clinic will not shame you for it. The right response is to assess it properly and plan around it.
Preparing the scalp before the operation
Control the condition with a sensible routine before surgery. For many people, this involves a dermatologist, a medicated shampoo, a gentle maintenance shampoo, and avoiding products that trigger irritation.
I avoid changing several strong products at once just before surgery. If the scalp improves or reacts, one clear change at a time makes it easier to see what helped and what irritated the skin.
If you use ketoconazole, selenium sulfide, salicylic acid, zinc pyrithione, or another treatment, your surgeon should know. The exact product and timing matter. Some products can help before surgery but be too strong for the fresh recipient area immediately after surgery.
If you are sensitive to products, look carefully at shampoos, oils, styling creams, fragrances, and leave in formulas. Harmful ingredients in hair products matter here because scalp irritation is not always caused by the disease itself. Sometimes the product routine is making it worse.
If minoxidil seems to trigger flaking or irritation, this should also be discussed before surgery. Some patients tolerate it well. Others react to the solution, foam, alcohol base, propylene glycol, or frequency of use.
Timing around minoxidil should be individualized. Stopping minoxidil before a hair transplant needs planning rather than improvisation.
Preparation does not mean sterilizing the scalp into perfection. The aim is to bring inflammation down, reduce itching, and make the surgical day more predictable.
If you have a severe flare, I may prefer that you control it first, send updated scalp photos, and only then confirm the final surgery date. This is not delay for its own sake. It is careful surgery.
Restarting medicated shampoo after surgery
For most patients, I avoid strong medicated shampoos or harsh dandruff products on the grafted area during the first 14 days unless I have specifically advised it. The recipient area is healing, crusts are forming and separating, and the washing routine should be gentle.

A flare still needs guidance. If itching or flaking becomes strong early, contact your surgeon instead of applying products randomly.
Medicated shampoos can usually return gradually after the surface has healed and the early graft protection period has passed. For some patients this may be after 2 weeks. For others, especially if the skin is reactive, it may be safer to wait longer or restart only on non grafted areas first.
A maintenance shampoo used on intact skin before surgery is different from applying the same product to fresh grafts, scabs, or irritated recipient area too early.
The exact timing depends on the operation, the condition of the scalp, the product, the strength of the medication, and how the healing looks. I slow down around universal instructions copied from one patient to another.
If you need treatment after surgery, ask clearly which product, which area, which day, how long to leave it on, and how often to use it. These details matter.
Patients also need to understand that baby shampoo forever is not a treatment plan for this condition. Gentle shampoo may be helpful early, but later the scalp may need its real maintenance routine again.
A staged return is usually the cleanest path. Protect the grafts first. Then treat the scalp intelligently. Do not sacrifice the early healing period because of panic, and do not let inflammation run uncontrolled because of fear.
Medication planning after surgery also matters. Some patients receive antibiotics after a hair transplant, pain medicine, anti swelling medicine, or other instructions from their clinic, and they may also have scalp treatments from a dermatologist. These should not be mixed casually without guidance.
If you already use a prescribed scalp treatment, bring the name and photos of the product to your consultation. Precise timing is not possible if the clinic does not know what you are using. That practical timing belongs with the wider plan for medications after a hair transplant.
Comfort is not the only goal. The scalp may itch before it is safe to use the old routine. Communication is better than improvising with a strong shampoo or cream too early.
The 5 slides here connect seborrheic dermatitis control with scalp comfort, infection risk, and surgery timing. Swipe sideways, use an arrow, or choose a number below the image.
Surgery can trigger a flare
Surgery can sometimes trigger or reveal a flare, especially in patients who already have a reactive scalp. This does not necessarily mean the transplant caused a new permanent disease.
The early recovery period changes the scalp routine. You may pause medicated shampoo, wash more gently, avoid usual products, sweat during travel, sleep differently, and feel more stress. Any of these can make a seborrheic tendency more visible.
Tell me about the condition before surgery. When the scalp history is clear, the early washing routine, treatment restart, and follow up plan can be adjusted without confusing a predictable flare with a surgical complication.
If a flare appears, make the message specific. Show clear photos, explain what you used before surgery, and do not scratch or apply strong products to the recipient area without approval.
If the condition appears during recovery
If a flare appears during recovery, do not panic and do not scratch. Contact your clinic, send clear photos, and describe the timing, symptoms, products used, and whether the concern is in the donor area, recipient area, or surrounding native hair.

Several different things can look similar after surgery. Crusts are not the same as dandruff. Normal redness is not always dermatitis. Pimples are not always infection. Dryness from washing is not always a seborrheic flare.
Visual follow up matters. A surgeon needs to see what the patient is calling dandruff, redness, scabs, or pimples. Redness, scabs, and pimples after a hair transplant can help patients separate common healing signs from problems that need attention.
If the flare is mild and the grafts are past the most vulnerable period, management is usually easier. If the flare is early, intense, or associated with scratching, a more controlled plan is safer.
Sometimes the concern is not the scalp condition alone. It may be folliculitis, irritation from a product, reaction to sweat, poor washing technique, or touching the scalp too much.
Do not self diagnose too confidently after surgery. A photo, a message, and a guided adjustment are often better than a week of experimenting.
The main rule is clear. Do not scratch the recipient area. If the itch is strong, ask for guidance. Protecting the grafts matters more than winning a fight with one itchy spot.
Scalp inflammation and donor recipient planning
Scalp inflammation can affect both the donor and recipient areas. People often think only about the top of the scalp, but the donor zone may be involved too.
The donor area is not just a place where hair is taken. It is a limited resource that must heal well and still look natural after extraction. This long term importance is why I pay close attention to the hair transplant donor area.
If the donor skin is inflamed, extraction planning deserves more attention. The surgeon may need to avoid irritated areas, reduce unnecessary trauma, and make sure you understand that donor healing can also itch or flake.
The recipient area also needs attention. Inflamed skin can be more reactive. This may affect comfort, redness, crusting, and the way recovery feels during healing. It may also make early follow up harder to interpret.
Surgical planning also has to ask why the scalp is inflamed. A chronic scalp condition, irritating medication, diffuse thinning, an unstable hair loss pattern, or poor washing because you are afraid to touch the scalp can all change the decision.
Medication decisions may also matter. Some patients with this condition are also trying finasteride, minoxidil, or both. Others want surgery without long term medication. Keep that decision separate from the scalp flare question, because seborrheic dermatitis control and native hair preservation are not the same problem.
A good plan looks at the whole scalp, not only the empty area. Hair restoration is not just filling a space. It is designing a result that can survive real skin behavior, ongoing hair loss, and future needs.
Questions to ask before committing
With this condition, I start with the actual state of the scalp. I assess whether the skin is calm enough for surgery, whether the donor or recipient area is involved, and whether the condition has been controlled for long enough to make healing predictable.
During consultation, I want the explanation to be concrete about what would make surgery reasonable and what would make a delay wiser. This may include the severity of flaking, redness, itching, inflammation, product irritation, or the need for dermatology treatment before travel is confirmed.
Product timing also matters. Some shampoos or scalp treatments can help before surgery, while others may need to stop around the operation. The exact answer depends on the product and your scalp, so the advice needs to come from someone who has actually evaluated the case.
Ask who will assess the scalp and who will perform the surgical steps. It matters because a reactive scalp needs judgment, not just a technical routine. That is one reason the question of who performs hair transplant surgery matters.
If the clinic gives only a quick yes without examining the scalp, be careful. Do not look for the clinic that says yes the fastest. Look for the surgeon who can explain when yes is safe, when no is wiser, and what must happen before surgery becomes reasonable.
Planning around seborrheic dermatitis
Treat the scalp condition as part of the surgical plan, not as a small side note. Control the scalp before surgery, document the condition clearly, use products thoughtfully, and keep communication open during recovery.
If your scalp is controlled, your donor is suitable, your hair loss pattern is appropriate, and your expectations are realistic, this diagnosis does not necessarily exclude you from surgery. Many people with this condition can still be considered.
If your scalp is actively inflamed, the better answer is patience. Treat first. Reassess. Then operate when the skin is settled.
This matters especially for patients traveling from another country. Do not hide a flare because flights and hotel dates are already arranged. Send photos early and ask for advice, because a few realistic messages can prevent a poor decision on the day of surgery.
Do not judge your scalp only on the best day of the week. If the condition looks calm for one day and then returns strongly two days later, the plan is not stable yet. A transplant is not planned for your best hour. It is planned for the real behavior of your scalp.
A few weeks later, with a ready scalp, is better than quick surgery on skin that is already irritated. This is the difference between rushing a case and managing it properly.
The real decision is wider than graft count. The skin, donor area, recipient area, and patient all need to be ready for surgery.
This only works when both sides are clear with each other. You tell me what your scalp does on bad days and what products you use. I assess whether the timing is safe, whether dermatology input is needed, and how the early washing plan should change.
When we do that, the decision becomes much clearer. You are not only asking whether surgery can be done despite the diagnosis. You are asking whether your scalp is controlled enough for surgery to be done responsibly.