


Scalp Eczema Needs a Quiet Scalp Before Grafts
A hair transplant can sometimes be possible with scalp eczema. But I do not operate through an active flare with open skin, wet crusting, spreading redness, bleeding from scratching, or itching you cannot control. Mild controlled dryness is a different situation from inflamed skin that is being rubbed, scratched, or reacting to products.
I first separate two questions. Is eczema causing temporary shedding or breakage, or is eczema present on a scalp that also has male or female pattern hair loss? Those are not the same problem, and they should not be planned as the same operation.
I judge the timing from the current skin surface, the real cause of the hair loss, the donor area, and whether you can protect the recipient area from scratching during the first healing days.
Scalp eczema changes the surgery decision
Scalp eczema changes the decision because the skin barrier may already be irritated before surgery begins. The same skin barrier logic applies when someone has a sunburned scalp before a hair transplant. FUE creates many small openings in the donor and recipient areas. That is normal surgery, but the skin still has to heal predictably.
The diagnosis name is not the only issue. The details that change the plan are active inflammation, broken skin, infection risk, and scratching behavior. A dry but settled scalp can be workable. A scalp that is cracked, wet, repeatedly scratched, or reacting strongly to products is much less controlled. I plan hair dye before hair transplant cautiously when dye or developer has ever caused itching, burning, or dermatitis.
The word eczema is also used loosely. One important differential is scalp ringworm before hair transplant, where fungal infection must be cleared before FUE is planned.
Atopic eczema, contact dermatitis from hair products, seborrheic dermatitis, psoriasis, folliculitis, and early scarring alopecia can all create redness, flakes, itching, or soreness. A quick photo should not become the diagnosis.
When the diagnosis is unclear, a focused review of itchy scalp and hair transplant timing can help separate mild dryness from a flare that needs treatment first.
After surgery, white flakes after hair transplant gives the narrower recovery stage triage for flakes, residue, and warning symptoms.
For that reason, an eczema history should lead to a better examination, not automatic rejection. Sometimes the scalp only needs treatment and time. In other cases, the diagnosis changes the whole plan.
Eczema should make surgery wait during active irritation
I delay surgery when the scalp has open cracks, bleeding from scratching, wet crusts, painful patches, pus, spreading heat, severe scaling, or itching you cannot control. I also slow the plan down after a recent topical medication change, a product reaction, or a rash that has not been properly diagnosed.
The recipient area needs protection in the first days after surgery. Scratching at night, rubbing towels aggressively, picking flakes, or trying random creams from the internet can disturb the same area we need to keep stable.
I also review the donor area. If eczema affects the back or sides of the scalp where grafts would be taken, extraction may be less predictable. Donor management is already important in every case, and skin inflammation adds another reason to be selective with graft use.
Waiting does not mean the opportunity is lost. Often, proper dermatology treatment and a stable scalp routine can make the surgical field much safer within a reasonable period.
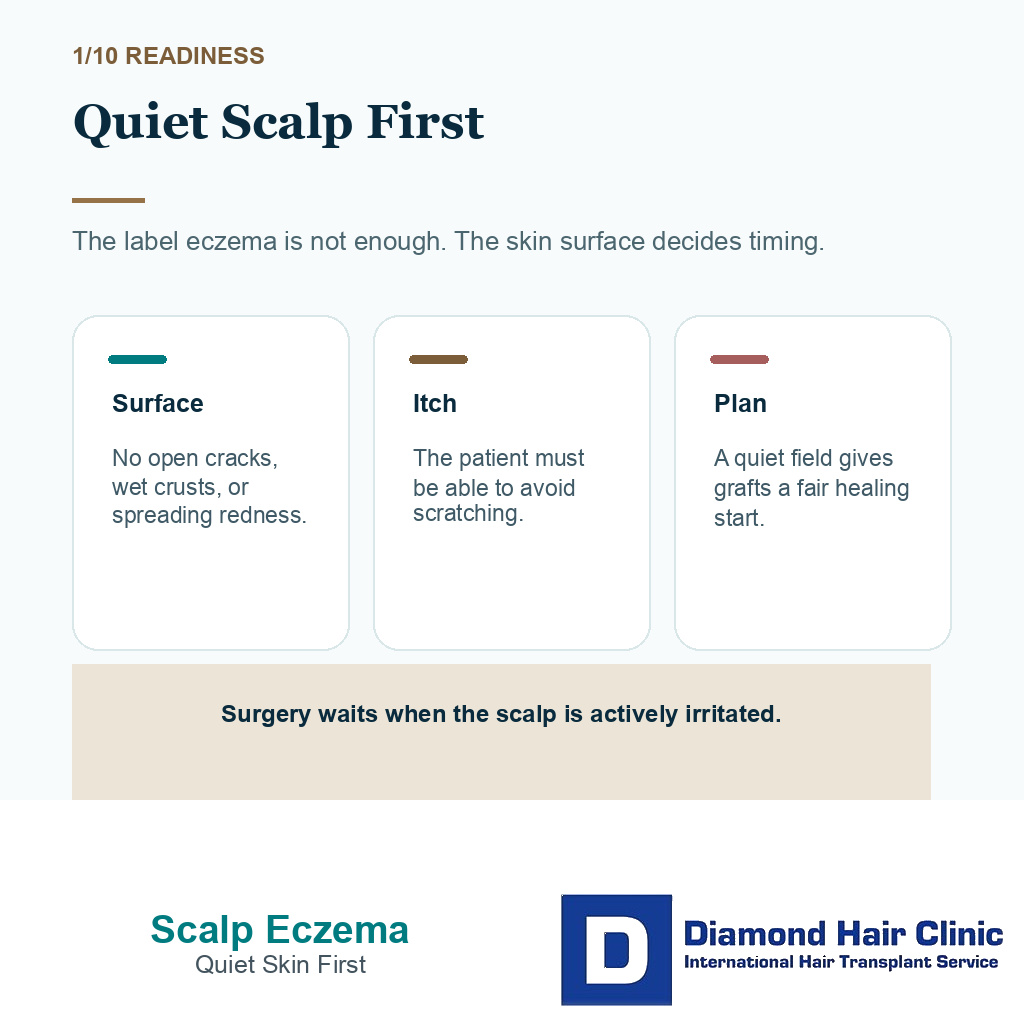
The scalp should be quiet before surgery
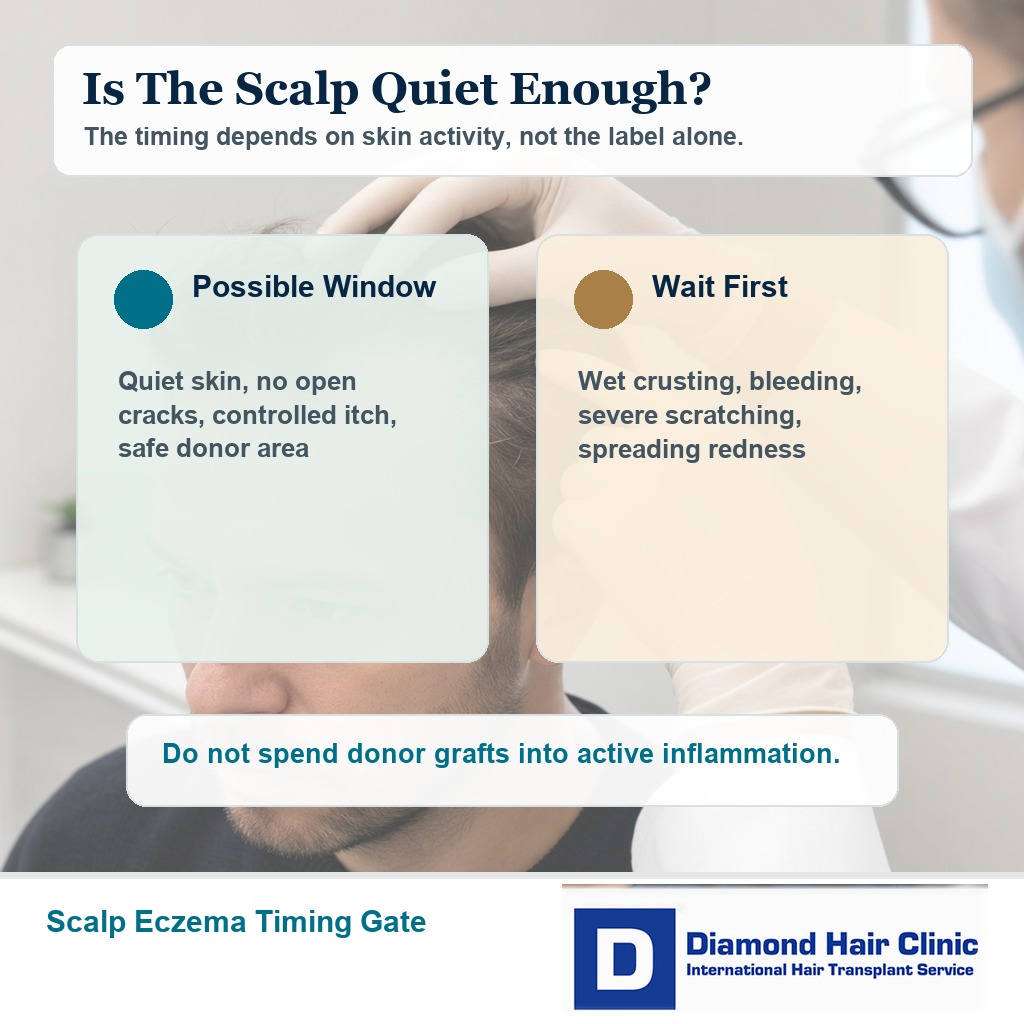
The scalp should be consistently quiet before surgery, not only improved for one or two good days. There should be no open skin, no wet crusting, no active infection, no severe itching, and no rapidly changing rash in the donor or recipient area.
For mild eczema that is controlled, dry, and not being scratched, surgery may still be discussed. For unstable eczema, the better sequence is diagnosis, treatment, observation, and then surgical planning.
The exact waiting period depends on the behavior of the skin. A mild flare that responds quickly may only need a short delay. A scalp that has been repeatedly inflamed, cracked, or treated with stronger medication needs a longer stable period before I spend donor grafts there.
This is similar to the timing logic I use for seborrheic dermatitis before a hair transplant and scalp psoriasis before a hair transplant. The diagnoses are different, but the surgical question is similar. Is the skin stable enough to operate responsibly?
Eczema treatment should be stable before surgery
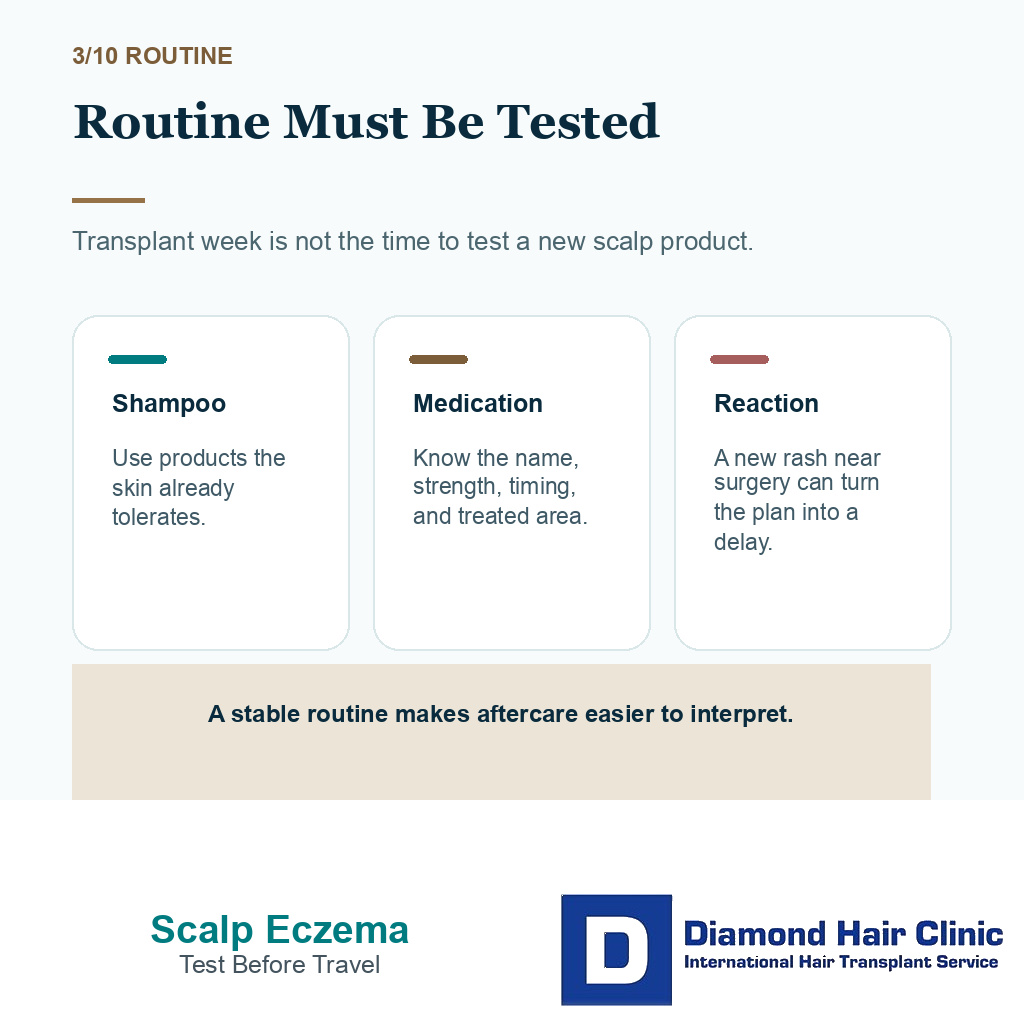
The scalp routine should already be tolerated before we reserve a surgical date. Transplant week is not the right moment to test a new lotion, strong shampoo, home remedy, hair dye, or steroid solution for the first time.
If a dermatologist has prescribed treatment, I need the name, strength, frequency, and exact area of use. Is it applied to the donor area, the planned recipient area, or both? The same principle applies to broader medication before a hair transplant. The issue is not only whether a product is allowed. The issue is whether the scalp is predictable enough for surgery.
The way treatment has been used matters. A short, supervised steroid solution to settle a flare is different from repeated unsupervised use whenever itching appears. The first may prepare the scalp. The second can hide the fact that the skin is still unstable.
For one person, the right plan may be to continue a familiar treatment until close to surgery and pause only what the clinic or dermatologist asks them to pause. For another, the safer plan is to delay the operation until the flare has stayed quiet for longer. I decide from the actual scalp behavior, not from the label eczema alone.
I use these 10 slides to keep eczema control, scalp quietness, medication timing, and graft safety in the same decision. Swipe sideways, use the arrows, or choose a number below the image.


Eczema can cause hair loss that does not need surgery
Eczema can be associated with temporary shedding, breakage, or thinning because of inflammation, rubbing, scratching, or irritation from products. If the follicle is still alive and the loss is reversible, a transplant is not the first answer.
This distinction protects the donor area. You may look in the mirror and see an empty area, but the cause may be active inflammation rather than permanent pattern hair loss. Using grafts too early can waste donor capacity on an area that may improve once the scalp is treated.
Repeated scratching can also break hairs and worsen irritation in the same patch. The first useful step is to settle the skin and stop the scratch cycle, not to cover the patch immediately with grafts.
When the hair loss follows a clear androgenetic pattern, eczema may be a timing issue rather than the main diagnosis. That is when the broader question of hair transplant candidacy becomes important.
Scalp products may cause contact dermatitis
Contact dermatitis can happen when the scalp reacts to a product, dye, adhesive, topical medication, shampoo, fragrance, preservative, or vehicle ingredient. This matters before hair transplant surgery because people often use minoxidil, topical finasteride, styling products, concealers, oils, dandruff shampoos, and cosmetic treatments while trying to manage hair loss.
If the rash appears exactly where a product is applied, or if it started after a new product, I need that checked before surgery. Otherwise you may keep applying the trigger during recovery and then blame the transplant for a skin reaction that was already being provoked.
Product irritation can also confuse the growth timeline. Itching, flakes, and shedding after surgery may come from normal healing, dermatitis, a medication vehicle, folliculitis, or a product used too early. The surgery may not be the cause, but the symptoms still make recovery harder to read.
If contact dermatitis is suspected, patch testing or dermatology review may be more valuable than changing hair transplant technique. The operation needs planning around a scalp routine you can actually tolerate.
Itching can threaten graft safety
Itching after surgery can be normal while the scalp heals, dries, sheds scabs, and starts to recover sensation. The unsafe part is not mild itching by itself. The unsafe part is scratching, picking, rubbing, or using strong products too early.
During the first 10 to 14 days, the grafts mainly need protection from friction and trauma. With eczema, I need a realistic prevention plan before surgery if you already scratch without noticing, especially at night.
The practical difference is behavior. Feeling itch but following instructions is different from repeatedly breaking the skin by scratching. The second situation needs to be stabilized first.
A light accidental touch is not the same as repeated scratching until the skin breaks. Panic can make people inspect the area again and again, and repeated inspection can become another form of trauma.
Eczema adds one extra layer. Itching after a hair transplant can overlap with baseline itch, so the plan should not assume a perfectly settled scalp after surgery.
Warning signs need medical review
Before surgery, medical review is needed if the eczema area is spreading, painful, wet, crusted, bleeding, infected, or not responding to usual treatment. Review is also needed if you have patchy hair loss, shiny scar like skin, loss of follicle openings, eyebrow loss, burning, or tenderness. Those signs can point to diagnoses beyond ordinary eczema.
After surgery, increasing pain, spreading warmth, pus, bad smell, fever, grey or black tissue, persistent wetness, or bleeding caused by scratching should not be treated casually. These signs need proper medical contact.
Not every red area is infection. Not every flake is dangerous. The useful distinction is whether the scalp is slowly settling or clearly getting worse.
How to recognize an infected hair transplant and folliculitis before a hair transplant both explain why bumps, pus, and active inflammation need more caution than ordinary dryness.
Scalp products matter before and after surgery
Eczema often leads to product stacking because the itch feels urgent. That can make the scalp harder to read. Before surgery, the routine should be stable, well tested, and already tolerated by your skin.
Do not start a strong new shampoo, steroid lotion, oil, dye, peel, antiseptic, or home remedy close to the operation unless your doctor has instructed it. A reaction in the final days before surgery can turn a planned operation into a delay.
After surgery, the recipient area should follow the clinic’s washing protocol first. Medicated shampoos and eczema treatments return only when the skin is closed enough and the clinic agrees. Ketoconazole shampoo after a hair transplant follows the same timing principle for dandruff treatment.
I am careful with products that promise fast soothing but leave heavy residue. The scalp may feel less itchy for a few hours, but occlusive or irritating products can make washing, inflammation, or folliculitis harder to manage.
Risky clinic promises around scalp eczema
No clinic should promise a normal result without first judging the scalp. Eczema may be mild and well controlled, or it may be active enough to change timing. A clinic that moves straight to graft numbers before asking about flares, scratching, medication, product reactions, and donor area involvement is skipping important information.
The way the promise is made matters. If the answer is only “FUE is safe” or “we can do it anyway,” the explanation is too thin. A proper answer explains whether surgery is appropriate now, whether treatment should come first, and what would make the plan less safe.
Photos alone are also limited. A photograph can show flakes or redness, but it may not show itch severity, broken skin, follicular openings, active scratching, or whether the diagnosis is correct. Planning a hair transplant from photos alone becomes especially risky when a medical scalp condition is involved.
When the scalp is not ready, delaying surgery should remain on the table. A delayed operation can still be a good operation. A rushed operation on active skin can spend grafts in the wrong environment.
Consultation details should include eczema history and treatments
Bring clear photos of the scalp during a flare and during a quiet period, your diagnosis if you have one, the names and strengths of creams or lotions you use, shampoo details, hair dye or product history, and any dermatologist notes. If you have had patch testing, biopsy, or treatment for psoriasis, seborrheic dermatitis, folliculitis, or scarring alopecia, bring that too.
I need to know how often you scratch, whether the itch wakes you at night, whether the skin ever cracks or bleeds, and whether products make it worse. These details are not small. They tell me how safe the first 10 to 14 days after surgery may be.
Basic medical screening may matter if eczema is part of a broader health picture or if you use medicines that affect healing, infection risk, or skin thickness. Screening is not bureaucracy when there is a real medical reason, especially when judging blood tests before a hair transplant.
The consultation should also define the goal. Are we treating permanent pattern hair loss, an area scratched for years, thinning caused by inflammation, or a mixture? The answer changes whether surgery is useful, delayed, or avoided.
Operating now or waiting depends on scalp control
Active inflammation, cracking, wet skin, infection, or uncontrolled scratching means the skin needs treatment first. If the scalp is quiet, the diagnosis is clear, the hair loss is permanent enough to justify grafts, and the donor area is safe, surgery can be considered carefully.
The decision should protect the donor area, not only fill the visible thinning. Donor grafts are limited. They should not be used before the skin and diagnosis are ready.
Eczema also changes aftercare in a practical way. Gentle washing, avoiding trauma, and knowing when to restart products matter more than buying many scalp treatments. The broader hair transplant aftercare routine should be adapted to your skin, not ignored.
My recommendation is to slow the plan down until the scalp is stable enough to give the grafts a fair environment. If that takes treatment first, it is not a failure. It is the decision that protects both the result and the donor area.