



- Written by Dr.Mehmet Demircioglu
- Estimated Reading Time 24 Minutes
Hairline Design Needs Long Term Planning
Hairline design should be planned around the patient’s face, age, donor capacity, hair loss pattern, hair caliber, temple shape, and future hair loss risk. The best hairline is not the lowest line and it is not the straightest line. For patients who prefer a sharper lower outline, I explain the tradeoffs in low straight hairline planning. Forehead muscle movement can limit hairline lowering, and the line still has to look natural today and make sense years later. If the proposed line is the reason you feel uneasy before a booked date, second thoughts before hair transplant surgery should be reviewed before grafts are placed. The same future hair loss concern becomes central during a hair transplant in the 30s.
When I design a hairline, I do not begin with a fashionable shape or a fixed measurement. I begin with the question of what the patient can safely support with the donor hair available. A hairline can look attractive in a drawing and still be wrong if it spends too many grafts, ignores future thinning, or creates a front edge that is too sharp for the face.
Design guide
Plan the hairline and coverage safely
These pages help you judge whether the grafts are being used for natural design, safe coverage, and future hair loss.
This makes hairline design an important part of a FUE hair transplant. The recipient area may heal well, the grafts may grow, and the density may be acceptable, but if the front border is too low, too flat, too dense, too regular, or placed at the wrong angle, the result can still look artificial. That is the same reason a month eight hairline check looks at edge shape, graft direction, and texture instead of judging growth alone. If that mistake has already happened, removing transplanted hair may be part of repair planning, but it should not be treated as a simple reversal.
Practical goal of hairline design
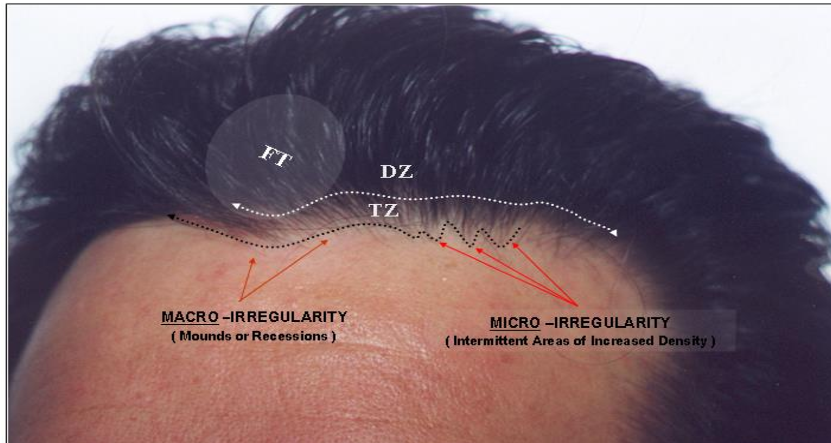
The practical goal is to rebuild the frame of the face without making the transplant visible. A natural hairline has a shape, but it also has softness. It has small irregularities, finer hair at the leading edge, careful density behind that edge, and a direction that matches the patient’s natural growth pattern. A related planning detail is nape hair for hairline transplants, where fine hair can help softness only if the lower donor border is reliable.
A good design should answer several questions before surgery begins. Where should the mid frontal point sit? How much temple recession should remain? Should the temple points be restored or left alone? How many grafts can be used at the front without weakening future options? How will the design look if the crown or mid scalp continues to thin? Those same questions become more concrete during Norwood 3 hairline planning, where corner closure can quickly become too aggressive. Before drawing the front edge, I also check whether the change is a mature hairline or receding hairline, because the answer changes how conservative the design should be. If eyebrow thinning, redness, or scarring clues appear with the front edge, I also review whether frontal fibrosing alopecia changes hairline transplant planning.
Those questions matter more than a dramatic mirror drawing. A hairline is not just a cosmetic outline. It is a long term surgical commitment. The same distinction applies to ARTAS hair transplant claims, because a robotic extraction device does not design the front border. They also matter more than AI hairline design advice, because a generated outline cannot spend donor grafts safely.
Hairline planning lens
Four checks before a hairline plan looks natural
A natural hairline is not only a low line or a dense line. It needs a soft front edge, the right graft mix behind it, natural angle and direction, and enough donor reserve for future hair loss.
Soft front edge
Will the first visible line look soft?
Single-hair grafts belong at the soft front edge, where harshness is easiest to notice.
Graft mix behind it
Are stronger grafts behind the edge?
The useful question is not only how many grafts are used. It is which grafts belong at each depth of the hairline.
Angle and direction
Does the angle follow nearby hair?
Naturalness depends on direction as much as density. A soft edge can still look wrong if the angle is wrong.
Future hair loss balance
Will the design still age well?
A hairline that looks dense today can become exposed if the surrounding native hair changes later.
The front edge should be planned before density is pushed behind it. If the first line is too heavy, the whole result can look less natural even when the grafts grow.
They can help behind the soft edge, where body is useful. They should not create a harsh first row or make the hairline look like a wall.
Hair that exits in the wrong direction can look artificial even at a modest density. Direction, lay, and graft choice have to work together.
A design that spends too much donor supply or sits too low may be harder to keep balanced later. Long term planning protects future options.
Use this as a planning frame, not a diagnosis of your hairline. The final design still depends on donor reserve, recipient area anatomy, hair type, and future hair loss risk.
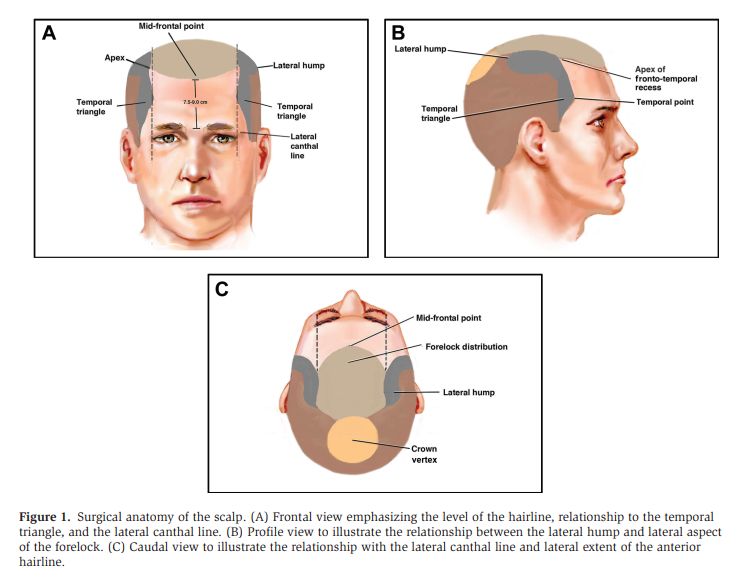
Front hairline position
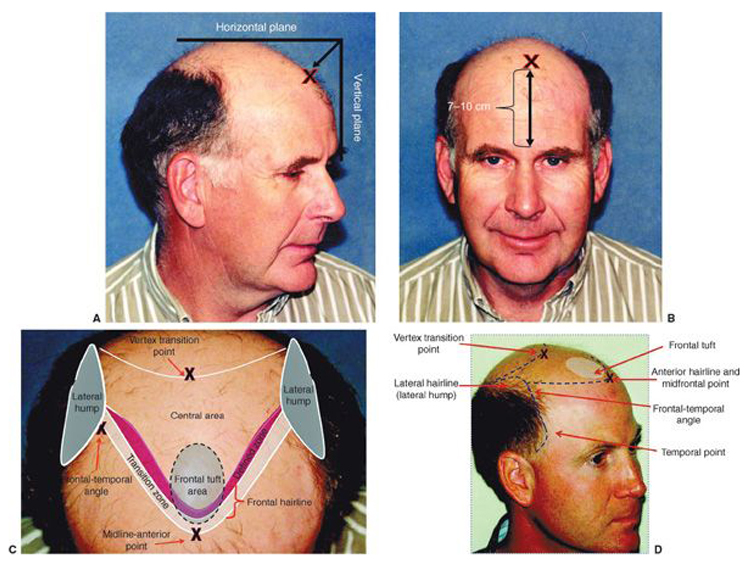
The front of the hairline is usually judged from the glabella, the area between the eyebrows, together with the upper third of the face, forehead shape, frontalis muscle, temple recession, and the patient’s natural facial proportions. A common reference is about 7 to 10 cm above the glabella, but I treat that as a reference, not a rule.
Some patients have always had a high forehead. Some have a mature adult hairline. Some have true recession caused by androgenetic alopecia. These are not the same problem. Lowering every patient to a youthful line can create an unnatural result and may waste grafts that will be needed later.
The safest design is often slightly conservative at the first surgery. If the result grows well and the donor area remains strong, refinement can sometimes be considered later. It is much harder to repair a line that was placed too low than to make a reasonable design slightly stronger in the future.
Younger men need the hairline decision to survive future thinning. If a patient is still losing hair behind the front, a low hairline can create a permanent island of transplanted hair with thinning behind it. The hairline may look good for a short time, but the long term picture becomes harder to manage.
Future hair loss changes the design
Hairline design should never be separated from the expected pattern of hair loss. Donor supply is limited, and the patient may later need coverage in the mid scalp, crown, or a repair area. A design that uses too many grafts at the front can make future planning weaker.
During consultation, I look at the patient’s current pattern, family history, age, miniaturization, medication plan, and donor area quality. This does not let anyone predict the future perfectly, but it helps avoid a design that only works in one photograph and fails as hair loss progresses.
With advanced baldness risk, I may protect the donor budget by avoiding an aggressive low line. With stable limited recession and a strong donor area, the design can sometimes be more detailed. The difference is not artistic taste alone. It is medical planning.
Donor supply is not unlimited. Every graft placed into the front is a graft that cannot later be used in the crown, mid scalp, or a repair area. I connect hairline design with donor area planning from the beginning rather than treating the front as an isolated cosmetic zone.
Patients who are unsure whether surgery is appropriate should first read about hair transplant candidacy, because the right hairline cannot be chosen until the patient is a good candidate for surgery.
Face shape and proportion guide the hairline
Facial proportion is useful, but it should not become a rigid formula. The forehead, eyebrows, temples, cheekbones, jaw, and skull shape all change how a hairline is perceived. Two patients can have the same measurement from the glabella and still need different designs.
A narrow face may look unnatural with a very broad flat front. A stronger jaw may tolerate a more angular adult frame. A softer face may need a gentler curve. A patient with deep temple recession may need the front line and temple transitions planned together, because filling only the center can make the sides look more exposed.
For women, the decision is often different. A female hairline transplant usually aims for softer facial framing rather than a masculine recession repair. I explain female hairline transplant planning separately.
For transgender patients who want a more feminine frame, the design also needs specific judgment about temple shape, forehead width, and softness. A feminine hairline transplant should not simply copy a standard male pattern.
Very low hairlines carry risk
A very low hairline can look exciting before surgery because it changes the face immediately in the mirror. But the mirror drawing does not show donor limits, future thinning, hair direction, graft survival, or how the design will look at age 40, 50, or 60.
The most common dangerous design is a low, flat, dense line offered to almost every patient. It may create a strong immediate promise, but it can look artificial after growth and can spend thousands of grafts in the wrong place.
I discussed this risk in more detail in low and flat hairlines. The key point is simple. A low line is not necessarily wrong, but it must be earned by the patient’s face, age, donor capacity, temple support, and long term plan.
If the front is lowered without supporting the sides, the hairline can look disconnected. If the corners are squared too strongly, the result can look drawn on. If the patient continues losing hair behind the transplanted line, the front may survive while the area behind it becomes weak.
Saying no to a requested hairline
A requested line has to change when it would spend grafts the donor area cannot safely spare, sit too low for future hair loss, need density the donor cannot support, or create a shape that will look artificial as the face and hair loss pattern changes.
A hairline drawing is not separate from donor planning. The front line, temple support, density behind the line, and possible crown loss all compete for the same limited graft supply. If the design ignores that, the patient may get a strong first impression and a poor long term plan.
When I raise or soften a proposed line, the reason is not taste. It is usually donor protection, natural angle, age, temple balance, or the need to protect lifetime graft options.
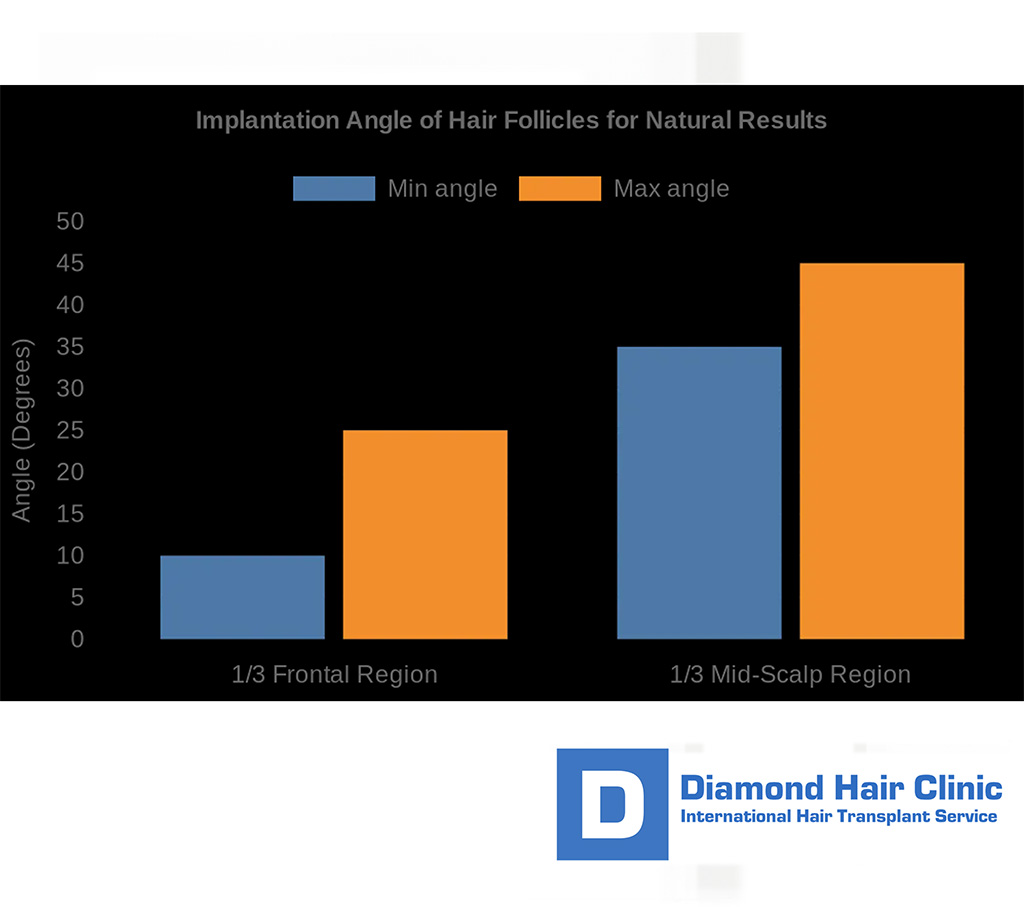
Angle and direction matter
Every graft grows in the direction created during the recipient area incisions. If the angle is wrong, the hair may grow upright, forward in the wrong way, or against the natural flow of the surrounding hair. Density cannot hide this completely.
In the frontal hairline, the hairs usually need a low forward angle with subtle direction changes across the curve. In the temple area, the angle becomes even flatter and the direction often moves down and back toward the ear. Temple point restoration is difficult.
Wrong direction is not just a styling problem. It can make a result look unnatural even when the grafts survive. Patients often feel that something looks off without knowing the cause. Many times the issue is the angle, the direction, or the transition between the frontal hairline and temples.
For patients who already have this problem, I explain the repair decision separately in the article about wrong hair direction after hair transplant.
Single hair grafts at the front
The leading edge of a natural hairline is not made of thick clusters. It is softer and more irregular. At the front, the first rows are usually created with single hair grafts, while grafts with two or three hairs are placed farther behind to create visual fullness. If one placed unit later seems to show another hair, that is a separate timing question from whether the front edge was planned with the right graft mix.
If thick grafts are placed at the very front, the line can look pluggy even when the surgery is technically clean. The patient may see growth, but the eye sees a border that is too heavy. This belongs among the reasons older or poorly planned results can look obvious.
A natural transition is created by combining fine graft selection, small irregularities, correct spacing, and careful density behind the front. It is not created by randomly scattering grafts. There should be planning behind the irregularity.
When the front edge has already been built with thick grafts, repair can be more complex. I discuss pluggy hairline repair separately.
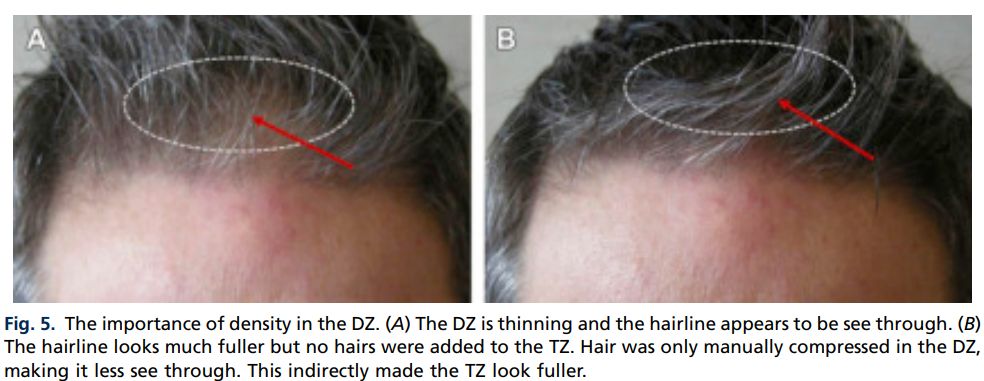
Hairline density planning
Hairline density should be high enough to frame the face, but not so aggressive that it damages growth, wastes grafts, or creates a wall like border. In many patients, a planned density around 35 to 45 follicular units per square cm can be a reasonable discussion point, but the correct number depends on hair caliber, skin contrast, graft quality, area size, and donor strength.
Patients often compare numbers without context. A hairline with fine blond hair on light skin may need different planning than dark straight hair on light skin or curly hair with strong coverage. The same density number can look very different from one patient to another. The same principle is expanded in blonde and red hair transplant planning for patients comparing light, copper, and red donor hair.
I also avoid placing too many grafts in a small area just to create a dramatic promise. Crowding can reduce blood supply around the grafts and may weaken survival. I explain that risk in the article about whether too many grafts in one area can damage a result.
The right density is a balance between natural appearance, safe growth, and donor management. More grafts are not always better.

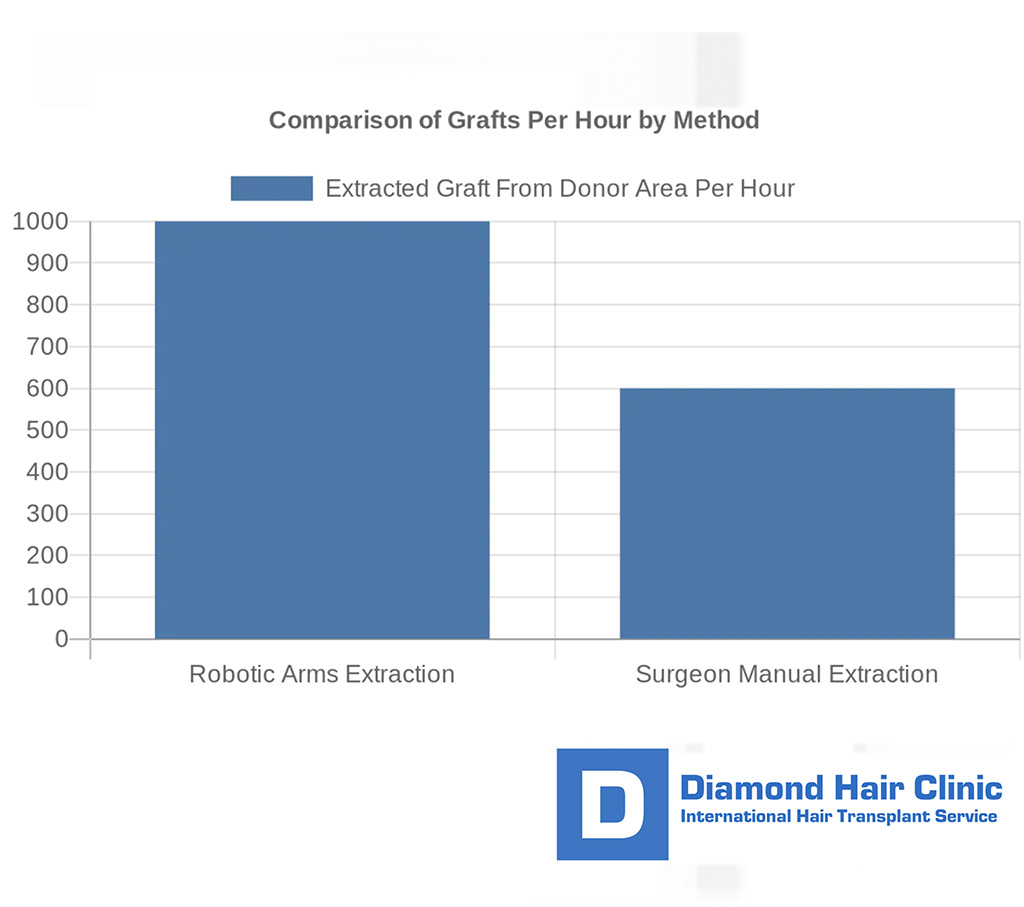
Technology cannot design the hairline for the surgeon
Technology can help with photography, measurement, magnification, planning, and documentation. It cannot replace surgical judgment. A hairline is not just a digital curve. It is a living design placed into skin, hair direction, blood supply, donor limits, and future hair loss.
Marketing that makes a device sound more important than the person making the decisions needs close reading. Sapphire blades, implanters, magnification, and planning tools can be useful, but they do not decide where the line belongs or how the grafts should be distributed.
For example, Sapphire FUE can be helpful in creating fine recipient area incisions, but it remains part of FUE. The value depends on how the surgeon uses the tool, not on the name of the tool alone.
Ask who designs the hairline, who creates the recipient area, and who is responsible if the design needs to be adjusted during surgery.

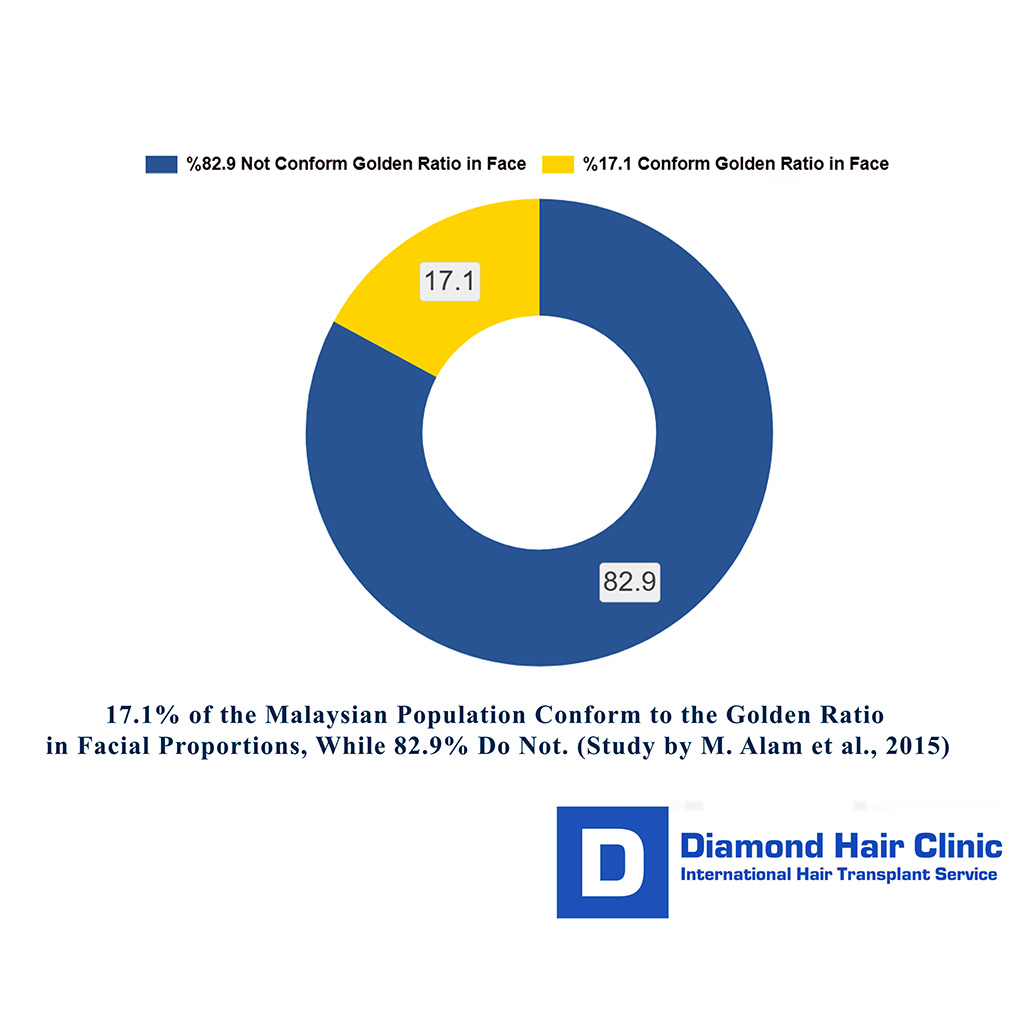
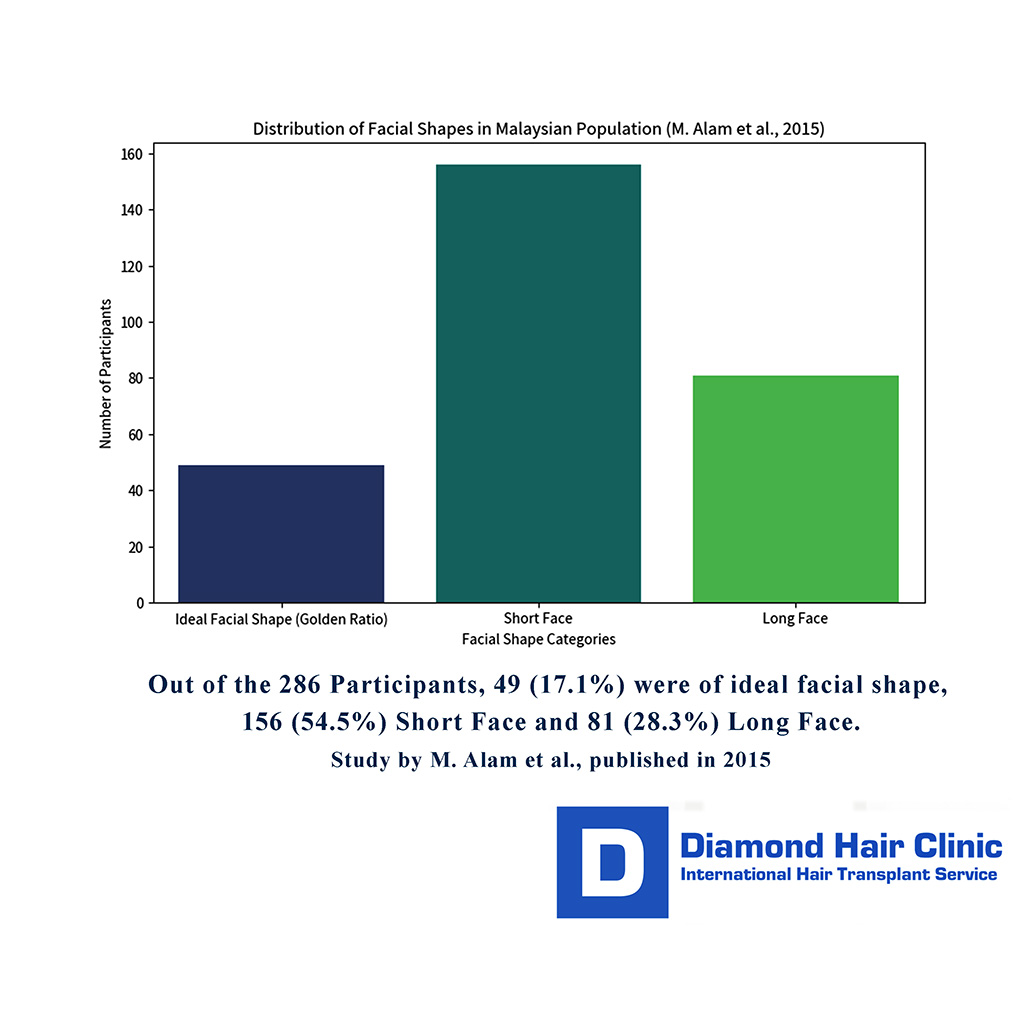
Golden ratio is a guide, not a rule
Facial proportion matters, but I do not treat the golden ratio as a command. Human faces are not identical and beauty is not a single mathematical template. Measurements can guide the discussion, but they should not force every patient into the same line.
The danger of strict proportion thinking is that it can make the design look correct on paper but wrong on the face. A patient with a naturally high forehead, strong family hair loss, or limited donor area may not be helped by forcing the upper third into a textbook measurement.
I use proportion as one part of the design. I also look at hairline memory, temple recession, eyebrow position, skull shape, hair type, donor capacity, and how the patient normally wears the hair. A natural result needs all of these pieces to agree.
Patient expectation must be discussed early. A person may ask for a teenage hairline, but the safer adult design may be a mature frame that looks natural and can be maintained safely over time.
Hair type and contrast change the plan
Hairline design changes with hair caliber, curl, color, and skin contrast. Fine hair usually creates a softer edge but may need more careful density planning. Coarse hair gives stronger coverage but can look heavier at the front if thick grafts are used too close to the border.
Curly hair can create excellent visual coverage, but the curl also makes angle control, graft handling, and exit direction more demanding. I explain Afro textured and very curly hair transplant planning separately.
Gray hair and mixed color hair also change the design. The contrast between hair and skin may be softer, but color variation can make uniform placement more visible if the grafts are not blended carefully. Patients with gray hair can read more about hair transplant with gray hair.
The same shape can look soft in one hair type and harsh in another, so I do not design hairlines from a template.
Natural hairline shapes
Several shapes can look natural when they belong to the patient. A gentle mature curve, a slightly stronger central forelock, mild temple recession, or a softer rounded frame can all be appropriate in different faces. The mistake is choosing the shape before understanding the patient.
Male hairlines often need some degree of mature temple recession. Removing that recession completely can make the result look artificial, especially as the patient ages. Female hairlines and feminine hairlines often need a different kind of softness, but even then the design must respect donor capacity and natural direction.
A natural hairline is also not perfectly symmetrical. Small differences between the two sides are normal. The goal is balance, not mirror copying. If the two sides are forced to match too exactly, the result can look designed rather than grown.
After surgery, patients may worry and ask whether an uneven hairline after transplant is normal. Sometimes it is swelling, scabbing, lighting, or intentional irregularity. Sometimes it is a true design issue. Timing and examination matter.
Temple point planning
Temple points can change the whole face, but they are one of the easiest areas to make unnatural. The hair is usually finer, flatter, and directed differently from the central frontal hairline. If temple grafts are too thick, too upright, too low, or too forward, the result can look obvious.
I do not restore temple points automatically. Some patients need only the frontal hairline. Some need a limited temple transition. Some should leave the temples more conservative to protect the donor area and avoid an artificial side frame.
Temple planning also affects the frontotemporal angle, which is the corner where the frontal line turns toward the side. If that angle is too square, too round, or placed without regard to the sideburn and parietal area, the face can look unbalanced.
Patients who need more detail can read about temple point hair transplant planning.
Artificial hairline warning signs
A hairline usually looks artificial for a combination of reasons. It may be too low for the patient’s age. It may be too straight. It may have thick grafts at the front. The density may be too uniform. The angle may be wrong. The temple points may be misplaced. The donor area may have been spent too aggressively to create an impressive front.
Another common problem is a visible gap between the transplanted front and the native hair behind it. This can happen during normal growth stages, but it can also reflect weak planning when native hair loss was not considered. I explain this in the article about a gap between transplanted and native hair.
Artificial results often begin before the operation, not during growth. If the design is wrong on the day of surgery, good growth cannot fully correct the visual problem. The design conversation deserves serious attention before any incisions are made.
Judge a strong result by naturalness, donor preservation, density, direction, and future planning. That broader judgment also depends on result quality after hair transplantation.
High forehead lowering with hair transplant
Hair transplantation can visually lower a high forehead by creating a new frontal frame with grafts. It does not physically move the scalp forward. Forehead reduction surgery is a different operation and should be evaluated separately when it is relevant.
Hairline design should start with what the donor can support, not with the lowest possible line. The amount of lowering has to fit donor capacity, future hair loss risk, temple shape, and natural density.
If the forehead is naturally high but donor supply is strong and the hair loss pattern is stable, careful lowering may be reasonable. If the patient is young, still thinning, or asking for a very low line, I become more conservative. The same request can be safe in one person and unsafe in another.
The final plan before surgery should explain what will be treated, what will be left alone, and what could still be refined later if the donor area remains strong.
Clinic model and hairline design responsibility
Hairline design is not a task that should be separated from the surgeon’s responsibility. The person who evaluates the donor area, plans the long term strategy, and understands the patient’s future risk should be involved in the design and recipient area decisions.
This matters especially for patients comparing clinics in Turkey. A high volume clinic may show a dramatic low line, a large graft number, and a quick package price. That does not tell the patient who designed the hairline, who made the incisions, or whether the donor area was protected.
Before choosing a clinic, patients should understand who actually performs the hair transplant and how the clinic protects donor capacity. For international patients, choosing a hair transplant clinic in Turkey can help separate marketing from medical responsibility.
My approach is slower and more careful because the hairline is the first thing people see and often the hardest thing to hide if it is wrong.
Use the 10 hairline design slides below to see how natural planning depends on age, donor reserve, graft choice, direction, face shape, and future hair loss. Swipe the carousel, use the arrows for one step at a time, or choose a number below the image to jump to that point.





Written hairline plan details
Before a patient accepts a hairline, the written plan has to show more than the drawn line. It needs to explain why that height was chosen, how many grafts are being spent in the front, whether temple support is included, and what donor reserve is being protected for future loss.
The first photos also have limits. A hairline can look clean immediately after surgery because the outline is visible, but growth, angle, density, and softness need time. Early photos should not be judged like final result photos.
Aftercare matters because the front line is exposed and easy to touch, style, or judge too early. Clear washing instructions, swelling guidance, scab care, and follow up photos help protect the design while it heals.
Reading the hairline during follow up
A hairline is not judged only from the first front photo. I look at healing, angle, direction, single hair placement at the edge, density transition behind the line, redness, styling, lighting, and whether native hair behind the transplant is still changing.
If the patient worries early, I separate normal recovery from design problems. Swelling, short shaved hairs, scabs, redness, or harsh light can make the line look sharper than it will later. Wrong direction, pluggy grafts, rows, or a hairline that sits too low are different concerns.
The written design gives follow up a reference. It helps the patient and surgeon compare the result with the agreed height, shape, soft edge, donor use, and areas intentionally left lighter.
Questions before accepting a hairline design
Before accepting a design, ask why the line is placed at that height, how many grafts are being used in the front, whether the temple points are being treated, what type of grafts will be used at the leading edge, and how the plan changes if hair loss continues.
Ask whether the design is based on your face or on a standard clinic template. Ask who will create the recipient area. Ask what happens if donor strength is lower than expected on surgery day. Ask whether medication, staged surgery, or a more conservative first session would be safer.
Also ask what the surgeon would avoid. A useful consultation should include limits. When the answer is only that everything is possible, the patient has not received enough protection. The design should make clear where density will be prioritized, where grafts will be saved, and why the chosen line is safer than a more dramatic alternative.
No patient needs to feel pressured to accept a hairline just because it looks dramatic in a mirror. The design should be explained clearly enough that the patient understands both the benefit and the cost of that choice.
Judge a proposed hairline by how it will age, not only by how it looks before surgery. A natural hairline is planned with discipline, proportion, donor protection, and surgical judgment. When those parts work together, the transplant has a much better chance of looking like the patient’s own hair rather than a surgical outline.
For patients with straight dark hair or strong contrast between hair and skin, broad design rules need a closer reading. In Asian hair transplant planning, hair shaft, contrast, direction, temples, and donor reserve all become part of the consultation.