


Removing Transplanted Hair and Repair Planning
Transplanted hair can sometimes be removed or reduced, but the safe method depends on what is actually wrong. A few misplaced hairs, a transplanted hairline that is too low, wrong direction, thick grafts, and raised skin texture are not the same problem. When the front edge itself is the issue, bad hairline graft removal needs a narrower plan than general hair removal.
Electrolysis can be useful for individual unwanted grafts or a small visible row. Laser hair removal may reduce some hairs, but on a transplanted hairline it is less predictable and can affect skin color or texture. Surgical graft removal, camouflage grafting, or staged repair may be better when the real problem is design, direction, scarred skin, or donor planning. A focused guide to laser hair removal for transplanted hair explains when that option is reasonable and when it is too blunt for hairline repair.
Before any hair is removed, I need to understand why the hair looks wrong, how the skin has healed, and whether removal will make the next repair easier or harder. A patient may look in the mirror and think, “I just need these grafts gone.” I understand that reaction. But removal is not an eraser. If the method creates scars, pigment change, empty shine, or an uneven front edge, the correction can become harder than the original problem.
What makes transplanted hair different from ordinary hair removal?
Transplanted hairs are not random cosmetic hairs. They were placed surgically into skin that has already gone through incisions, swelling, scabbing, healing, and sometimes scar formation. The angle, depth, and grouping of those grafts may be different from the surrounding native hair, so I do not treat the area like ordinary body hair removal.
The scalp also has a visual memory. Even if a hair is removed, the skin may still show tiny surface changes, dots, shine, redness, or texture from the original implantation. In some patients this is minor. In others, especially after dense low hairlines, thick grafts, or repeated surgery, the skin itself becomes part of the repair problem. The aim is not only to remove hair. The aim is to leave a forehead and hairline zone that can still look natural under daylight.
Before choosing a method, I separate three questions. Which hairs should disappear? Which hairs should be softened or thinned? Which hairs should stay because they can help a future repair? Removing the visible shaft, weakening a follicle, extracting a graft, and redesigning a hairline are separate decisions.
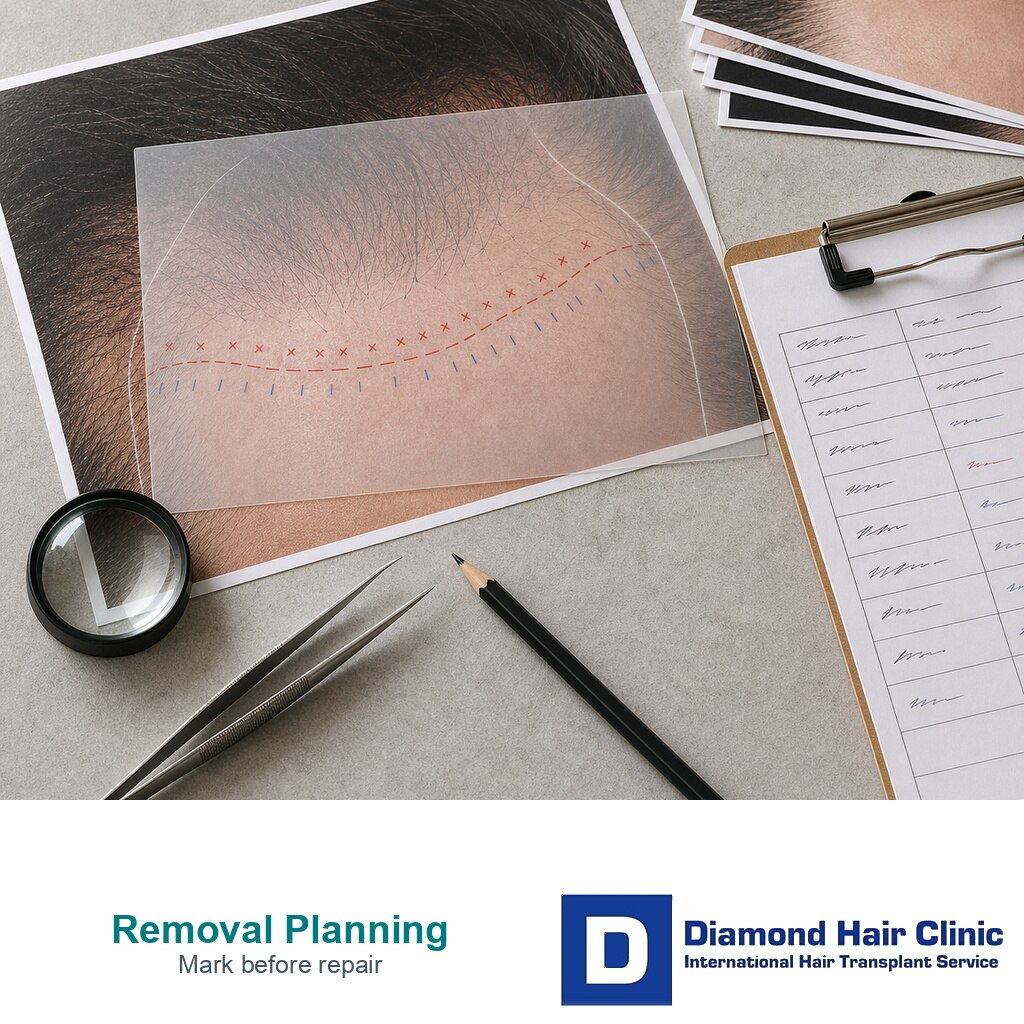
The proposed keep zone and remove zone should be marked on photos before any treatment starts. The person doing the treatment should not be choosing hairs casually while the patient is already in the chair. Removing too much can create a bare scarred zone. Removing too little can leave the same artificial edge.

The right option depends on the defect, the skin, and the future repair plan.
Electrolysis can help when the target is precise
Electrolysis can help when the target is precise. I consider it when a patient has a small number of low grafts, scattered hairs below the intended line, a few thick hairs at the front edge, or a visible row that needs softening rather than a full surgical revision. It works one hair at a time, so it can be useful when the surgeon wants to preserve nearby useful grafts.
Because electrolysis treats each follicle directly, it can still be considered when hair color or skin contrast makes laser less reliable. The tradeoff is that the operator must be able to target transplanted grafts precisely, ideally from a marked plan, because destroying a useful follicle removes that option from the repair plan.
I also explain that electrolysis is a removal decision, not a way to rescue grafts. If a transplanted hair follicle is successfully destroyed, that hair is not available later for redistribution into a better hairline.
The advantage is control. If only a few hairs sit below the intended line, electrolysis may allow gradual removal while we watch how the skin and shape respond. That is different from trying to clear a whole low band. A staged approach can be especially helpful when the patient is emotionally distressed and wants an immediate fix, because the first step should still protect future options.
The limitation is time and skill. Transplanted scalp hairs can be coarse, deep, angled, or clustered. Several sessions may be needed. Skin can become irritated if treatment is too aggressive, too early, or done by someone who does not understand hair transplant anatomy. A first conservative session can sometimes teach us how the skin reacts before a wider removal plan is attempted. If the unwanted area is large, dense, or structurally misplaced, electrolysis alone may become slow, patchy, and frustrating.
Laser hair removal is less predictable on transplanted scalp hair
Laser hair removal can reduce hair growth by targeting pigment in hair follicles, but it should be understood as reduction, not a promise that every transplanted follicle will be erased in a clean line. The result depends on hair color, skin color, device settings, hair cycle, and operator judgment. On the scalp after a transplant, I am more cautious because the patient is often treating the most visible part of the face, the frontal hairline.
Laser can be attractive because it sounds faster than electrolysis. But speed is not the same as precision. It may weaken some hairs more than others, leave uneven regrowth, or thin hairs in a way that does not match the desired hairline design. In darker skin types, recently tanned skin, or skin with irritation, the laser type, energy, cooling, and spacing between sessions matter because the risk of pigment change and burns is higher. If laser is discussed, the target zone should be marked, the expected reduction should be stated clearly, and the skin should be checked after the early sessions before pushing the plan wider. The forehead is not the place for casual testing.
I do not say laser has no role. In selected cases it may be discussed with a qualified laser specialist, especially when the target area is broad and the patient understands the uncertainty. The surgeon and laser specialist should agree which zone is being reduced before treatment starts. When the issue is a few misplaced grafts, a sharp front row, or a small low patch, electrolysis or surgical removal may offer better control.
Does a low or straight hairline need redesign first?
A low or straight transplanted line is one of the hardest situations. The problem may not be too much hair. It may be the shape. Natural hairline design depends on age, face shape, temple support, hair caliber, donor reserve, and future loss risk. If the first design ignored those factors, removing hairs without redesigning the line can leave a different unnatural shape.
I first mark the line that should probably remain and the zone that may need thinning or removal. Then I ask whether the temples need correction, whether the central forelock should be softened, whether thick grafts are causing a pluggy look, and whether the patient has enough donor hair for a future repair. Removal and repair planning often become one decision here.
Some low hairlines need selective removal below the correct line. Some need pluggy hairline transplant repair with soft single hair grafts. Some need camouflage behind the line rather than removing everything in front. Some cannot be made perfect without spending too much donor hair. The responsible choice depends on the scalp in front of me, not on the wish to erase the first operation.
Use these 10 graft removal slides to compare diagnosis, electrolysis, laser limits, surgical repair, skin risk, donor value, and route choice before removing useful grafts. Swipe sideways, use an arrow, or choose a number below the image.




Surgical repair can be better than removing hairs one by one
Surgical repair may be better when the unwanted grafts are dense, deeply placed, contain several hairs, are wrongly angled, or are sitting in scarred skin. In those cases, removing one hair at a time can be too slow or may leave the main problem unchanged. A surgeon may need to remove selected grafts, redistribute useful grafts, revise the front edge, or plan camouflage around a new hairline.
Repair after a bad hair transplant starts with diagnosis. A patient can have good growth and still have a bad design. Another patient can have weak growth but acceptable placement. Another may have wrong hair direction after hair transplant, where the hair exits the scalp at an angle that fights the native pattern. These are different problems.
If the first row is too thick or too upright, adding more grafts behind it may only make the hairline darker. If the low line is the real problem, camouflage alone may spend donor grafts without correcting the position. If the skin has raised texture, surgery may need to be staged slowly. The repair method should match the defect, not the patient’s understandable wish for the fastest visible change.

Before removing grafts, check whether the next repair will still be possible.
Skin risk must be checked before removal
Before electrolysis, laser, or graft removal, I check the skin for redness, raised scars, pitting, shine, infection history, keloid tendency, inflammation that looks like acne, poor healing, skin tone, recent tanning or sun exposure, and any sign that the skin is still unsettled. If the main concern is raised or indented hairline texture, that needs its own review before any removal plan. I also ask about photosensitizing medicines, recent peels or laser, and whether previous small injuries left dark marks or raised scars. If the transplant is recent, waiting may be the better decision because the hair and skin can still change.
The skin risk is not theoretical. Electrolysis can irritate skin or, if performed poorly, cause infection or small scars. Laser can cause burns, crusting, pigment change, or texture change when settings, skin type, or after treatment instructions are wrong. Surgical graft removal can leave small scars or uneven surface if too many grafts are removed too aggressively. These risks may be acceptable in selected cases, but they must be chosen deliberately.
This is also why I ask patients not to test a random patch at home, pluck grafts repeatedly, burn hairs, use depilatory creams near the hairline, or start treatment before the operating clinic or a repair surgeon reviews the case. A few weeks of impatience can create months of harder repair work.
Should hairs be removed before a second transplant?
I first ask whether the misplaced grafts block the next design. If they block the correct hairline, removal may be needed before a second surgery. If they can be incorporated into a softer design, removal may waste useful hair. If the donor area is already limited, every usable graft matters. I also check whether the hairs are mature enough to judge. Removing grafts during early panic can erase hairs that might later have been used to soften the repair. A second hair transplant should spend grafts only when the goal is clear enough to justify the donor cost.
Donor damage changes the repair plan. A patient who already has overharvested donor area concerns cannot treat repair as an unlimited menu. If the donor has been weakened, the plan may need to prioritize the most visible defect and accept limits elsewhere. Removing hairs from the front while ignoring the donor reserve can leave the patient with a cleaner forehead but fewer ways to rebuild coverage.
The order matters. A surgeon may choose removal first, then healing, then redesign. Or the plan may be camouflage first with no removal. Or it may be no surgery for now, especially if the first transplant is still maturing. Timing is part of the treatment.
Photos and records that help repair planning
For a repair review, I need the original graft number, photos before surgery, photos immediately after surgery, current photos in normal light, photos with wet hair, donor photos, medication history, and the timeline month by month. A hair transplant plan from photos can begin the discussion, but a repair decision often needs direct examination because skin texture, graft angle, and donor quality are hard to judge through pictures alone.
Records also protect the patient from repeating the same mistake. If the first clinic placed too many grafts too low, I want to understand why. It may have been patient pressure, clinic pressure, poor design, weak donor planning, or a misunderstanding about future hair loss. I want to see whether the original marked line, graft placement photos, and current mature photos tell the same story. If that reason stays unclear, the second plan can repeat the same logic with different tools.
When a patient feels a poor hair transplant result needs refund or repair, I keep the emotional, financial, and surgical questions separate. The refund argument is about the agreement. The repair plan is about what the scalp can safely tolerate now.
Avoid home removal before a repair review
Do not pluck transplanted hairs repeatedly to see if they will weaken. Plucking may remove the visible shaft for a while, but it does not create a controlled repair plan and can irritate the follicle or skin. Careful trimming changes hair above the skin. Plucking, depilatory creams, IPL, laser, and electrolysis act on the skin or follicle, and that difference matters in an already operated hairline. Do not use facial depilatory creams on the transplanted hairline. Do not shave aggressively over irritated skin. Do not pick at bumps, crusts, or raised areas. Do not use home IPL or laser devices on a transplanted hairline, and do not treat a low hairline with unplanned laser sessions because another patient’s case sounded similar.
Also avoid making a decision that is hard to reverse during the early panic stage. A hairline can look wiry, harsh, or too dark before maturation. If the worry is that one front graft appears thicker later, first review why a hairline graft can show another hair later before choosing removal. That does not mean every worried patient needs to wait forever, but it does mean the final plan should be based on the mature defect when possible. Many repair decisions are more reliable around 12 months, unless there is a clear medical problem or a severe structural issue that needs earlier observation.
If the skin is painful, hot, draining, dark, spreading in redness, or worsening quickly, that is a medical review issue, not a cosmetic hair removal issue. Health signs come before appearance.

Home removal attempts can irritate skin, waste useful grafts, and make repair planning harder.
Deciding between removal, camouflage, and repair
I decide by asking what will leave the patient with the most natural long term appearance and the least future damage. If only a few hairs are low, electrolysis may be enough. If a broad low band was transplanted, selective surgical removal or staged repair may be needed. If the hairline is slightly harsh but in a reasonable position, softening and camouflage may be better than trying to erase it.
Comparable cases matter too. Hair transplant results from patients with similar hair are more useful than ideal photos from very different scalps. Fine straight hair, coarse dark hair, curly hair, high contrast between skin and hair, and strong future hair loss risk all change the repair calculation. A method that looks acceptable on one scalp can look obvious on another.
The final plan should name the target hairs, the reason for removing them, who will perform each step, the likely number of sessions or stages, the skin risks, the donor reserve, and the fallback if the first stage is not enough. It should also say what will not be touched yet. When the plan cannot answer those points, I slow it down. The patient has already lived with one decision that was hard to revise. The next plan should reduce the visible problem without creating a new one.