


Hair Transplant Planning From Photos Alone
A hair transplant plan can begin from photos, but photos should not be treated as the final surgical plan. Photos can help me understand the visible pattern of hair loss, the general shape of the hairline, the condition of the crown, and the patient’s main concern. That same comparison is why I ask patients to look for results from patients with similar hair characteristics before relying on a gallery. A polished online result can start the same conversation, but social media hair transplant results still cannot replace donor and hairline assessment. Photos are even more limited when the question is menopause hair loss and hair transplant candidacy, because the donor and diagnosis still need clinical review.
What photos cannot show reliably is just as important. They cannot fully show donor quality, miniaturization, scalp condition, hair caliber, graft survival potential, or whether the requested result is safe for the future. This is especially true with a deeper inflammatory scalp condition such as dissecting cellulitis, because photos may not show whether the skin is quiet enough for surgery. Hair pulling related patches create the same problem because broken hairs, scalp texture, and stability all need closer assessment. Hair color can create another blind spot, especially when gray or white donor hair is difficult to judge from casual images. A scalp mole in the planned transplant area is another detail that may need direct skin examination.
Practical guide
Plan the trip around
the medical decision
A remote photo plan is only one part of safe travel planning. Use the route that matches what you need to understand before arranging flights, payment, or follow-up.
A photo based plan should stay provisional until the scalp or facial hair area is examined properly. This matters even more when a patient wants to plan a hair transplant before a wedding or asks for mustache hair transplant planning from close up photos, because the deadline can make a photo based estimate feel more certain than it really is. This does not make online consultation useless. It simply means that photos should start the medical assessment, not finish it.
It is natural for patients to want a clear answer before traveling, paying a deposit, taking time away from work, or arranging a trip to Istanbul. Many patients send photos and expect a fixed graft number, a final price, and a definite surgery plan. The practical order is to review the deposit decision before booking, because the danger begins when a clinic turns a few photos into certainty about the outcome or a rushed surgery date.
A useful plan leaves the patient clearer, not just more eager to book. A photo review should not turn an early impression into certainty. It should clarify what may be possible, what may be risky, what still needs examination, and whether medical checks such as blood tests are still needed before surgery. If the remaining unknowns are important, pausing before hair transplant surgery is better than pretending a photo estimate is final. That clarity is also needed before trusting a robotic hair transplant claim, because the machine name cannot replace candidacy and donor review.
Reading a remote photo set before travel
When an international patient sends photos, I do not look only for the area that bothers them most. I first separate the visible complaint from the surgical limit. The hairline may be the emotional concern, but the donor area, crown pattern, mid scalp thinning, age, medication history, and previous surgery history decide how much can be done safely. This is especially important in Norwood 4 or 5 hair transplant planning, because photos can understate the donor and crown tradeoff.
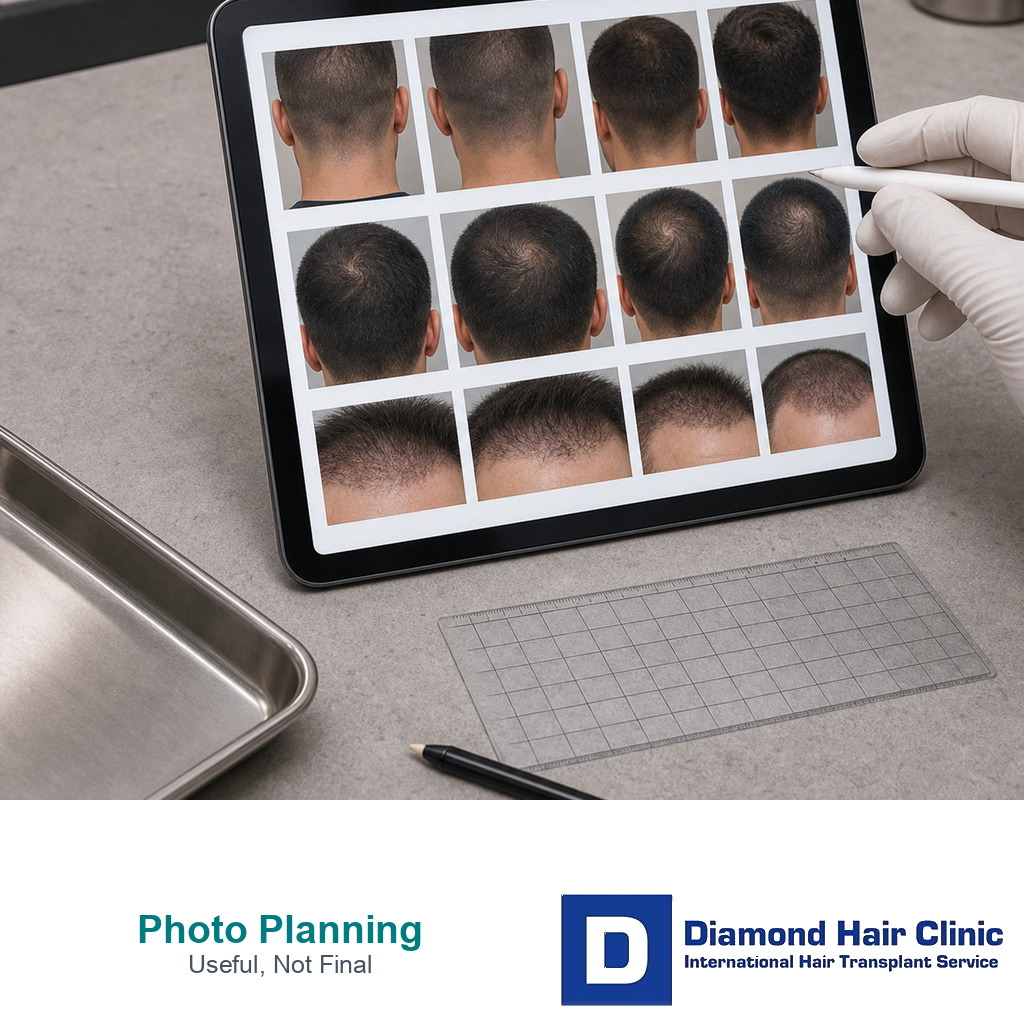
The photo set should be taken on the same day, in clear light, without filters, fibers, concealer, wet styling, or extreme angles. I need front, top, crown, both temple, both side, and donor area views. Donor photos are usually better when another person takes them from the back and both sides, because mirror photos often hide miniaturization and old extraction marks.
If there was previous surgery, scalp injury, skin disease, medication use, or a visible scar, I want that information before travel. A photo review becomes weaker when the most important limitation is kept outside the frame.
A useful remote review usually has two answers. One answer is what seems possible if the donor area confirms well in person. The other answer is what would make me reduce, delay, or refuse the plan after examination. Both answers belong in the case review before travel, before flights or payment make the decision feel fixed.
A remote plan also has to explain what is still provisional. If I cannot judge donor capacity, miniaturization, scalp condition, or hair caliber well enough from the photos, I say that directly rather than turning the photo review into a final promise.
What can photos show before surgery?
Clear photos are useful because they show whether the main concern is the hairline, temples, mid scalp, crown, or a combination of areas. They can also show whether the patient is asking for a small refinement or a more advanced reconstruction. If fibers or scalp concealer are being used, send a clean set as well because hair fibers before a hair transplant can make photo estimates too optimistic. The same caution applies when photos are taken while a patient is still comparing a hair system or hair transplant.
Start by understanding the pattern. Frontal hair loss, crown involvement, weakness behind the frontal area, and the difference between a naturally high forehead and progressive male pattern hair loss all change the plan.
These questions matter because the visible complaint is not always the real surgical problem. A patient may send me close photos of the temples because that is what bothers them in the mirror. A careful review may show that the mid scalp is thinning as well. If that is ignored, the surgery may create a front that looks stronger for a short time while the area behind it continues to weaken.
Photos can also help me start a conversation about expectations. Some patients want a modest natural improvement. Some want a very low, very dense, very youthful hairline. Some do not realize how much donor hair would be required to reach what they are imagining.
The first value of photos is not that they give a final answer. Their value is that they help the consultation ask better questions. The same boundary applies to AI hair transplant planning. The output is useful only when it leads to better surgeon questions, not fixed certainty.
Photos are the beginning of an assessment. They can help show whether a patient may be a good candidate for a hair transplant, but they do not replace clinical judgment. A patient is not only a picture of hair loss. Age, donor area, hair caliber, family history, previous treatments, and the long term pattern all matter.
Photos that make consultation more useful
If a patient wants a more useful remote consultation, the photos should be clear and taken in good light. Send photos from the front, both temples, both sides, the top, the crown, and the donor area at the back and sides of the scalp, especially before making a major pre surgery haircut change.
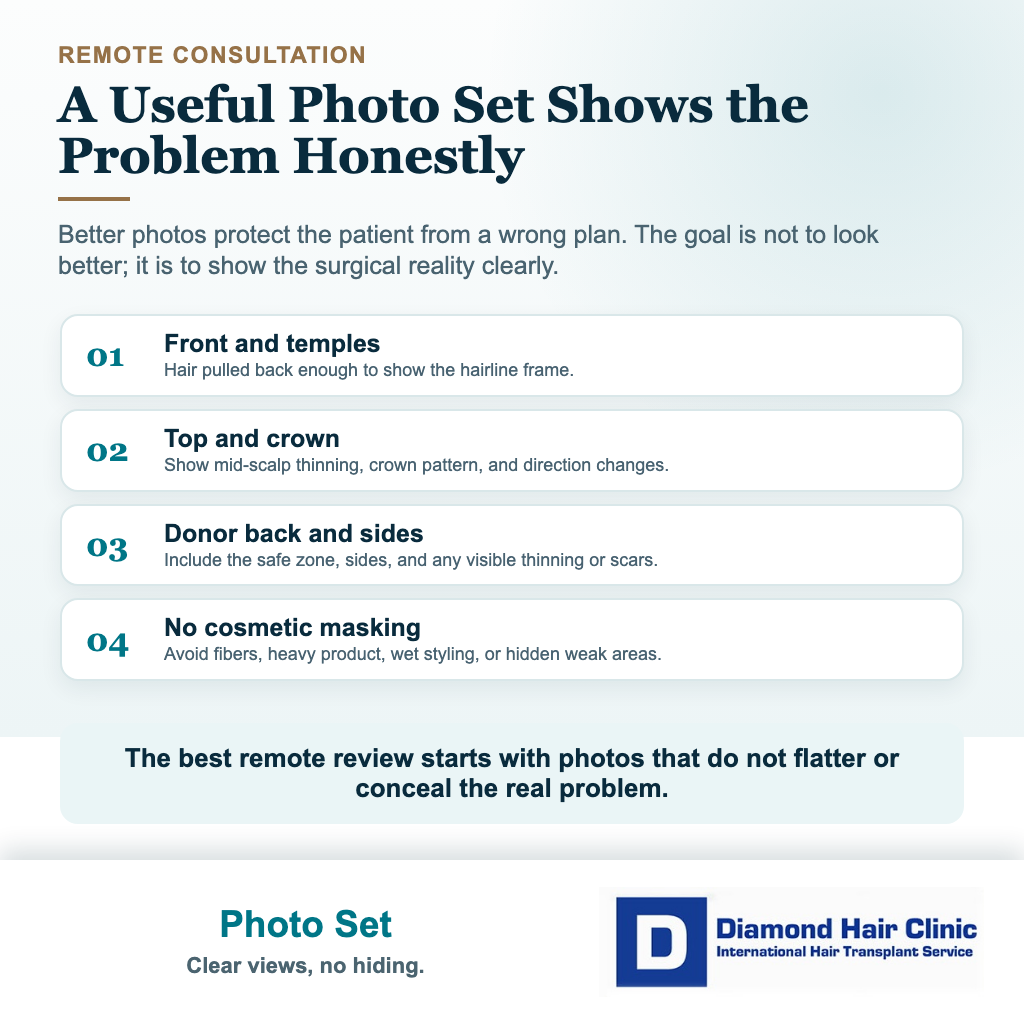
The hair should not be heavily styled, covered with fibers, wet with product, or arranged to hide the weak areas. The purpose is not to make the patient feel exposed. Clear photos protect the patient from a wrong plan.
A photo with the hair pulled back can be very useful for judging the hairline and temples. A photo from above can show whether the mid scalp is also thinning. Crown photos should be taken from more than one angle because the crown can look very different depending on lighting, hair direction, and the natural swirl pattern.
Donor photos should include the back and both sides because donor hair is not one flat block. The area above the ears, the lower donor border, and the central back of the scalp may not all have the same strength. If only one attractive donor photo is sent, the consultation may miss real limitations.
Send age, family hair loss history, previous treatments, medication use, previous hair transplant history if there is one, and the main goal. Without this information, even good photos can lead to an incomplete assessment.
The better the information, the clearer the remote consultation can be. A useful photo consultation is not just a scalp check. It also needs the story behind the photos.
What can photos not show clearly enough?
Photos often hide the details that decide whether surgery is wise. Lighting can make hair look thicker or thinner. Wet hair can reveal weakness that dry styled hair hides. A short haircut can make the donor area look clean even when the density is not strong. A dark room can hide miniaturization. A bright bathroom mirror can exaggerate it.

Photos often miss miniaturization. Miniaturized hair is hair that is still present but has become thinner, weaker, and less reliable. It matters because transplanting among weak native hair is not the same as transplanting into a completely bald area.
If the existing hair is unstable, surgery may need to be smaller or delayed, and medical treatment may need to be discussed first. In some patients, it is safer to confirm whether the surrounding hair can be stabilized before using grafts in that area.
Photos also do not show scalp quality well enough. The scalp has to be checked for oiliness, inflammation, scarring, irritation, or another condition. A patient may think they have ordinary male pattern hair loss, but sometimes the story is more complex. A condition such as alopecia areata, or any wrong diagnosis, can turn a technically possible surgery into a poor decision.
Another limitation is hair caliber. Thick hair gives more visual coverage than fine hair, even with the same number of grafts. Curly hair behaves differently from straight hair. High contrast between dark hair and light skin makes thinning easier to see. These details affect planning, but they are often distorted by camera angle, flash, styling products, and image compression.
The missing detail is direct examination. The donor area needs to be seen in real life, the direction of hair growth needs to be examined, and the proposed recipient area must be checked for fragile native hair.
A remote consultation can be helpful, but it cannot give the same certainty as a proper surgical evaluation.
Plans based on photos should stay provisional
A hair transplant plan from photos alone should stay provisional because surgery uses a limited resource. Donor hair does not behave like a product that can simply be replaced if the first plan is wrong. Once grafts are removed, they are spent from the patient’s lifetime graft supply. Once a hairline is placed too low, repair can be difficult. Once too many grafts are used in one direction, future planning becomes smaller.
A remote graft estimate should not be treated as a promise. It may be a reasonable early estimate, but it is still an estimate. The final plan should depend on donor quality, safe extraction limits, recipient area size, hair shaft thickness, hair loss stability, and the patient’s long term needs.
Patients often ask why one clinic says one number and another clinic says something very different. The answer is not always that one clinic is right and the other is wrong. Sometimes they are simply using different assumptions. One clinic may plan only the hairline. Another may include the mid scalp. Another may try to cover the crown. Another may be selling a large package. When graft numbers differ between clinics, compare what each number is trying to cover.
From photos, it is easy to say a number that sounds confident. It is harder to explain why the number may need to change after examination. But that clarity protects the patient.
If I estimate a range remotely, the patient still needs to understand that the range must be confirmed before surgery. Certainty should come from evaluation, not from sales pressure.
A provisional plan is not a poor plan. It is a careful plan. It tells the patient what seems possible while leaving room for the truth that can only be seen when the scalp is examined closely. That is the difference between a consultation that respects surgery and a quote that treats surgery like a package.
Graft numbers from photos can be misleading
Graft numbers look precise, so patients naturally trust them. A clinic may say 2,500 grafts, 3,500 grafts, or 4,500 grafts, and the patient feels they have received a serious medical plan. But a number without reasoning is not enough.
A remote graft number has two sides. One side is the visible area that needs coverage. The other is the donor capacity that must pay for that coverage. Photos usually show the first side more clearly than the second.
The right graft number depends on the size of the area, the desired density, the hairline design, the crown pattern, donor strength, hair caliber, and the need to protect grafts for later years. If these details are not discussed, the number may be more of a sales figure than a surgical plan.
Calculating graft numbers is not only about how many grafts can be placed. The real decision is how many grafts can be used without weakening the donor area or closing off future options. That difference changes the whole plan.
More grafts can sometimes improve coverage, but more grafts can also create unnecessary trauma, donor thinning, poor future options, or an unnatural design if the plan is not disciplined.
Photos can make this confusion worse. If the hair is styled forward, the area may look smaller. If the hair is wet or pulled back, the area may look larger. If the crown is not photographed properly, it may be ignored. If donor reserve is not shown clearly, a large graft number may be offered without knowing whether the donor can safely support it.
The number has to match the goal. A small temple correction does not require the same thinking as advanced hair loss. A crown case is not the same as a frontal hairline case. A young patient with ongoing loss is not the same as an older patient with a stable pattern.
The same number can be reasonable in one case and irresponsible in another. The logic behind the number matters more than the number alone. If a patient only remembers the number, they may shop for the biggest one. If they understand the reasoning, they can judge the plan more intelligently.
Donor area judgment before surgery
Donor hair is a limited surgical resource. It must provide hair for the current surgery, possible future hair loss, and sometimes repair work if a previous surgery was poor.
Photos can sometimes show obvious weakness, such as thinning above the ears, a narrow safe zone, retrograde loss, scars, or visible patchiness. But many donor concerns are more subtle. A donor area can look acceptable in a photo and still be limited when examined closely.
Before surgery, density, hair caliber, safe extraction zones, contrast, hair direction, scalp condition, and donor stability all need evaluation. Donor reserve is not just the back of the head. It is the foundation of the whole operation.
A strong donor area does not mean unlimited surgery. It only means the surgeon has more room to plan carefully. Even in a strong donor, extraction should be distributed intelligently. In a weak donor, the plan may need to be smaller, more conservative, or postponed.
Remote planning can be dangerous when it becomes too certain. A patient may receive a high graft quote without anyone truly studying the donor area. They may feel encouraged because the clinic sounds sure of itself. But certainty does not protect the donor. Planning protects the donor.
Telling a patient that donor capacity is limited is kinder than pretending everything can be covered. This can be disappointing in the beginning, but it is kinder than using grafts aggressively and leaving the patient with visible donor depletion later.
Photos can start the review, but this slide sequence shows how to use them without treating them as the final surgical plan. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.



Hairline planning needs more than a photo drawing
A hairline drawn on a photo can look attractive, but it can also be misleading. A line on a screen does not show where hairline lowering should stop near the forehead muscle, how the temples frame the face, how dense the hair needs to be, or how the design will age.
Natural hairline design is not only about placing the line lower. Proportion, age, facial structure, future loss, hair direction, temple recession, and density transition all matter. The frontal rows must look soft. The angle of growth must be correct. The hairline should belong to the patient’s face, not to a generic template.
A very low line drawn across the forehead needs caution. The desire is understandable. Hair loss can make a patient feel older than they are. But a teenage hairline on an adult face can look unnatural, and it may consume grafts that are needed later.
A hairline discussion should go beyond the first mirror reaction. The drawn line may look nice today, but the useful question is whether the design will still look natural when the patient is older and if native hair behind it continues to thin.
Photos can show the requested shape, but they cannot replace real design. In person, facial movement, forehead muscle activity, temple structure, hair angle, and the way the patient’s hair behaves without perfect styling can be assessed. These details shape the final design.
A natural hairline should not only photograph well. It should live well. It should look natural under daylight, in wind, with wet hair, and when the patient is not thinking about their hair at all.
When is an online consultation still useful?
An online consultation can be very useful as a screening step, not as the final surgical decision. It can help determine whether surgery may be worth exploring, whether the patient needs better photos, whether the hair loss pattern looks stable, and whether the expectations seem realistic. It can also save a patient from traveling when the basic situation already suggests that surgery is not wise.
Remote review matters when the patient is traveling from abroad. Many patients cannot visit Istanbul only to hear that they are not ready for surgery. A careful remote review can prevent unnecessary travel, unnecessary deposits, and unrealistic hope.
The concern begins when the online consultation becomes too certain too quickly. If a clinic gives a fixed high graft number after a few casual photos, promises full coverage, pressures the patient to book, and avoids discussing limitations, that is a warning sign. That is not careful planning. That is a sales process wearing medical language.
A useful online consultation explains what can be seen and what cannot be confirmed yet. It asks for proper photos, age, family hair loss pattern, previous treatments, medication tolerance, expectations, and medical history, including issues such as high blood pressure.
If crown coverage is part of the concern, the conversation should also include the limits of a crown hair transplant, because the crown can use many grafts and still look thinner than the patient expects.
Some patients may need medical treatment before surgery. Others may need a smaller first session. Some may be better served by waiting. A remote consultation is useful when it helps the patient understand these possibilities before becoming emotionally committed to a date.
So yes, photos and online consultation can help. They should start the decision, not finish it.
Who should confirm the plan before surgery?
The final plan should be confirmed by the surgeon who is responsible for the medical and artistic decisions of the operation. A coordinator can collect photos, organize travel details, explain logistics, and help the patient communicate. But a coordinator should not be the person making the final decision about hairline design, donor limits, recipient area density, or when to stop.
It matters because many weak plans sound very organized before surgery. A patient may receive a graft number, a hotel plan, a surgery date, and a price, but still not know who will make the surgical decisions. That is not enough. The plan needs to make clear who performs the hair transplant surgery and who controls the steps that determine the result.
If the final examination changes the plan, the explanation should come from surgical judgment, not from sales pressure. A lower graft number, a more mature hairline, or a decision to delay crown work can feel disappointing, but those changes may protect the patient. The useful detail is whether the change makes the result safer and more natural in the long term plan.
Warning signs of a weak plan based on photos
Pause if a clinic gives a fixed high graft number from a few casual photos, promises full coverage without discussing donor limits, ignores the crown or mid scalp, or pushes the patient to book quickly before the plan has been properly explained.
Be cautious if the clinic does not ask about age, family hair loss history, medication use, previous surgery, donor area photos, or expectations. These details are not small details. They can change the whole surgical plan.
A poor remote plan usually sounds very confident but explains very little. A stronger consultation may sound less dramatic, but it will explain what can be seen, what cannot be confirmed yet, and what must be checked before surgery.
Another concern is when the clinic treats uncertainty as weakness. In hair transplantation, uncertainty is sometimes appropriate. If the photos are not enough, the responsible response is not to pretend. It is to ask for better photos, explain the limitations, or reserve the final plan for the in person examination.
This matters for patients considering surgery abroad. In Turkey, many patients compare packages, hotels, transfers, and graft numbers before they understand the surgical plan. The red flags of Turkish hair transplant clinics matter here because a confident message can still hide weak medical planning.
Treating a remote plan as final before examination
Before trusting a plan made from photos, separate provisional guidance from a final surgical decision. An ethical clinic should be comfortable saying that the final decision depends on examination. If the clinic acts as though photos alone are enough for complete certainty, that should make you pause.
The donor area should be described with more attention than a quick look at the back of the head. The plan should check for weakness, retrograde thinning, scarring, fine hair caliber, or a limit that should make the surgery smaller. The surgeon should confirm this in person before the final decision.
The graft number should be tied to actual areas, not left as a vague total. The plan needs to say whether it covers only the hairline, the frontal third, the mid scalp, the crown, or a staged combination. Many misunderstandings happen because one number is heard as full coverage.
Ask whether the clinic considered diffuse thinning. This matters when the hair still looks present but weak across a wider area. Transplanting into diffuse thinning requires more caution than simply filling a bald temple.
Ask whether medication before a hair transplant should be considered. Medication decisions differ, and some patients cannot or do not want to use certain treatments. But the discussion matters. If ongoing loss is ignored, the surgery may solve one visible area while the surrounding native hair continues to weaken.
The final decision should belong to the person medically responsible for the surgery. A clinic name, package name, or technique name does not tell the patient enough. If the donor or hairline plan changes on surgery day, the reason and the responsible surgeon need to be clear.
If the final examination changes the plan
Sometimes the final examination confirms the remote plan. Sometimes it changes it. A change after examination can be protective when it reflects donor quality, scalp findings, or a more realistic hairline design.
The graft number may need to be reduced if donor reserve is weaker than expected. The hairline may need to be adjusted if the requested position is too low or too aggressive. The crown may need to be delayed if using too many grafts there would weaken the frontal result.
In some patients, surgery may even need to be postponed if the scalp condition, donor quality, or hair loss pattern is not suitable. This is disappointing for a patient who already arranged travel, but it is still better than performing a surgery that should not be done.
The purpose of the final examination is not to protect the first estimate. It is to protect the patient.
A careful plan should be flexible enough to change when the real scalp gives better information than the photos. A clinic that refuses to adjust the plan after seeing better evidence is not being consistent. It may simply be protecting the sale.
When is waiting for in person assessment wiser?
It is wiser to wait, or to be declined for hair transplant for now, when the plan depends on details that photos cannot show clearly. This includes weak donor area, possible diffuse thinning, young age, unstable hair loss, previous surgery, scar tissue, scalp disease, unrealistic hairline requests, or advanced baldness where graft distribution must be very strategic.
It is also wiser to wait if two or three clinics gave very different plans and none explained the difference. A second opinion before a hair transplant can protect the donor area before committing. Confusion is not always a bad sign. Sometimes confusion is the signal that the case needs a more careful review.
If a patient is being pushed toward a large surgery quickly, pause as well. Urgency is not a medical argument. A limited time discount does not make the donor stronger. A package offer does not make a low hairline safer. A busy clinic calendar does not prove that the plan is right.
Patients researching Turkey often compare price, hotel, transfer, graft number, and social media results. Those details matter in practical terms, but they do not replace surgical judgment. If you are trying to choose a hair transplant clinic in Turkey, pay attention to how the clinic handles uncertainty. A careful clinic will not be afraid to tell you what cannot be promised from photos.
Waiting does not always mean delaying surgery for years. Sometimes it means waiting until the surgeon examines you properly. Sometimes it means taking better photos. Sometimes it means stabilizing hair loss first. Sometimes it means accepting a smaller first surgery instead of trying to solve every area at once.
Speed can feel comforting before surgery and expensive after surgery. In hair transplantation, a careful pause can protect the donor area, the hairline, and the long term plan.
Making a clearer decision before committing to surgery
Before committing, it helps to know the plan in plain language, not as a collection of impressive numbers. The conversation should make clear which area will be treated first, what will be left for later, how the donor will be protected, and what may happen if hair loss continues.
The decision should not depend on one flattering photo, one large graft number, one generated preview, or one quick message. It should come from a consistent explanation that connects the hairline, donor area, crown, native hair, age, medication discussion, and future risk. If you use an AI hair transplant simulation, use it to explain your preference, not to replace donor and hairline assessment.
The patient also needs to know what is still provisional. A plan from photos can guide the first conversation, but the final examination may show weaker donor density, active miniaturization, scalp disease, or a crown that needs a different strategy.
Before paying a deposit, the patient needs clarity on what should be clear before you book a hair transplant. The plan needs to explain what is being treated, what is being left alone, who is responsible for the key steps, and what may change after examination.
A remote plan should not sound more complete than it is. The job is not to perform the largest surgery that can be sold from a screen. It is to choose the operation that still makes sense when the scalp, donor area, and long term pattern are examined carefully.
If a clinic can explain only the number, the package, and the date, the plan is not ready yet. A more protective plan explains what is still provisional, what must be checked in person, and why the final decision protects the donor area as well as the visible result.