



Graft Number Planning in Hair Transplant Surgery
The number on a quote sheet is not where the plan begins. I first map the recipient area and then ask what the donor area can safely give. The simple calculation is recipient area in cm2 multiplied by the planned density for that zone. The surgical plan changes after hair caliber, curl, color contrast, donor strength, age, crown involvement, future hair loss, and expectations are reviewed. That is especially clear in blonde and red hair transplant planning, where the same graft number can look different once pigment and shaft caliber are considered together.
For example, a 60 cm2 frontal area planned at 35 grafts per cm2 would need about 2,100 grafts. The same area planned at 45 grafts per cm2 would need about 2,700 grafts. Those numbers sound precise, but they are only the starting point. The right graft number is the number that improves the visible problem without wasting donor reserve. Because donor hair does not grow back after FUE, every removed graft has to belong to a lifetime donor budget.
What Should You Check Before Accepting a Graft Quote?
A serious quote should explain which areas are being treated, the approximate surface area, the planned density, donor capacity, crown strategy, and future reserve. If the quote only gives a number and a price, you still do not know the real plan.
The first number is usually a range before examination. If photos suggest 2,500 to 3,000 grafts, that range may become more precise after shaving, drawing the hairline, checking miniaturization, and measuring the donor area. When two clinics give different graft numbers, the useful comparison is not which number is larger. It is which clinic can explain the map behind the number.
The Starting Calculation
First, I estimate the size of the area that truly needs grafts. Then I choose the density for each zone. A compact hairline refinement needs a different plan from a large crown or a wide frontal and mid scalp case.
You may hear 30, 35, 40, or 45 grafts per cm2. These are density figures, not guarantees. The same density can look strong in one case and thin in another, so I treat whether 45 grafts per cm2 is enough as a planning question, not a universal promise.
I also separate peak density from average density. A selected part of the frontal hairline may receive more density, while the transition zone, mid scalp, or crown may receive less. If one density number is used for the entire head, you need to ask exactly where that number is being used.
The calculation also has a time and handling limit. A safe plan is not only how many grafts can be removed today. It also depends on how long the operation will take, how well grafts can be sorted and protected, how evenly extractions can be distributed, and whether quality can be maintained until the last graft is placed.
Sometimes that calculation leads to a staged hair transplant plan rather than spending too much donor reserve in one operation.
Why Is the First Quote Only an Estimate?
Good head photos show the pattern, direction, hair length before surgery, crown position, and whether the hairline looks reasonable. They still do not measure everything. Donor density, hair shaft thickness, miniaturization, scalp quality, and how the hair behaves when wet, parted, or shaved all need a closer review.
I ask for clear photos from several angles before giving an early range. A hair transplant plan from photos needs context, not only a top view image and a requested graft number.
The estimate becomes more reliable during examination. The donor area can be checked with magnification, the recipient area can be drawn properly, and the hairline can be measured against the face. A clinic that gives an exact fixed number from weak photos is giving confidence before it has enough evidence.
The first quote should also leave room for medical clarity. Sometimes the shaved examination shows more miniaturization than the photos suggested. Sometimes donor strength is lower than expected. Sometimes the requested hairline is too low for the donor reserve. In those situations, a smaller or differently distributed plan can be safer than forcing the original number.
What Does the Graft Number Actually Mean?
A graft is a follicular unit. It may contain one hair, two hairs, three hairs, and sometimes more. This means 1,000 grafts does not mean 1,000 hairs. If the average is two hairs per graft, then 1,000 grafts means about 2,000 hairs.
This changes expectations. A case with many grafts containing two or three hairs can create more visual coverage from the same graft count than a case with mostly grafts containing one hair. Hair caliber also matters. Thick hair covers more scalp than very fine hair.
I keep this distinction clear because clinics sometimes use graft count as if every graft is equal. They are not equal. A plan using 2,500 grafts with strong hair caliber and good average hair count can look fuller than a higher number in a person with very fine hair, high skin contrast, and a large recipient area.
Donor Capacity Comes Before the Wish List
Donor hair comes from the back and sides of the scalp, and that reserve is limited. A hair transplant redistributes hair. It does not create new hair. So the calculation must begin with what the donor area can safely give, not only what the recipient area would ideally receive.
Donor capacity depends on follicular unit density, total safe donor surface, hair caliber, hair count per graft, skin and hair contrast, curl, previous surgery, scarring, and whether there is thinning inside the donor area. The donor area in hair transplant surgery is not only the place hair comes from. It is the limit that decides how ambitious the plan can be.
A 4,000 or 5,000 graft plan needs donor evidence. The number sounding common is not enough. Some cases can support a larger session. Some cannot. A weak donor area, diffuse thinning, retrograde thinning, or previous overuse can make a lower number safer. The page about hair transplant with a weak donor area is relevant when the donor supply is uncertain.
If the case may need more work later, I think in terms of lifetime graft planning. Using too many grafts early can make a future crown, mid scalp, or repair plan harder.
The extraction pattern matters as much as the total. If too many grafts are removed from one narrow zone, the donor area may look patchy even if the total number does not sound extreme. I use broad, randomized distribution that respects the safe donor area and avoids a visible extraction pattern.
A graft quote should be checked before surgery with the treated map, density target, donor reserve, hair quality, zone priorities, high number risks, safer reductions, future loss, formula limits, and written proof. Swipe sideways, use the arrows for one slide at a time, or choose a number below the image.


How Does the Recipient Area Change the Number?
The recipient area is not one flat surface. A small frontal corner, the frontal third, mid scalp, and crown each ask for a different density and different distribution. A crown can consume many grafts because the whorl spreads coverage in a circular pattern.
The goal also matters. A hairline that frames the face may give a stronger visible improvement than trying to thinly cover every bald area. Often, I prioritize the front before the crown because the frontal frame affects the face more directly. That same limit applies when deciding hairline or crown first.
If the recipient area is too large for the donor supply, the graft number alone cannot solve the problem. The plan has to choose priorities. In some cases, that means hairline and frontal framing first. In others, the crown may be delayed, reduced, or planned with more modest expectations.
Hair Caliber, Curl, and Contrast Change Coverage
Hair caliber is one of the main reasons two people with the same graft number can look different. Coarser hair creates more visual coverage. Fine hair often needs more grafts to create the same impression, but the donor area may not allow that.
Curl and wave can also improve coverage because the hair occupies more visual space. Skin and hair color contrast matters as well. Black straight hair on light skin shows scalp more easily than wavy dark blond hair on medium skin. The same graft density can therefore look different in two cases.
Ethnic background can influence average hair caliber, curl, and hair count per graft, but individual measurement is more important than ethnic assumption. I may consider those patterns, but I do not calculate a patient from ethnicity alone. The scalp in front of me is the real evidence.
This is also where before and after photos can mislead. A result may look dense because the hair is thick, long, wavy, and low contrast against the skin. Another result may look thinner with the same graft number because the hair is straight, fine, short, and dark against pale skin. The count is only one part of visible fullness.
Hairline and Crown Need Different Planning
The hairline needs softness, irregularity, angle control, and grafts containing one hair at the front. A natural hairline is not a dense line of grafts. It has to match the face, age, temple pattern, donor reserve, and future hair loss. This point is part of hairline design.
The crown is different. It has a swirl pattern and often needs many grafts to create moderate coverage. A crown can look thin under harsh light even with a reasonable number of grafts. Crown hair transplant planning needs more caution in young men or anyone with limited donor supply.
The number is only useful when you know where the grafts will go. A quote for 3,000 grafts does not mean much unless you know whether those grafts are planned for the hairline, frontal third, mid scalp, crown, or all of them.
When Can a High Graft Number Become Dangerous?
Large graft numbers can help when donor supply is strong, the case is appropriate, and the surgical team can handle the grafts carefully. They become dangerous when the number is used as marketing. The concern with too many grafts is not only the total. It is where the grafts are taken from, where they are placed, and whether the tissue can support the plan.
Donor area overharvesting can leave the back and sides patchy, transparent, or visibly thinned when the hair is cut short. It can also make future repair harder.
High density placement can be risky if grafts are packed beyond what the tissue can support. The recipient area needs blood supply. If a clinic tries to create a number that looks impressive on paper but ignores tissue limits, survival may suffer and the final result can look worse than a more moderate plan.
Large numbers can also hide fatigue and handling problems. Grafts need to be extracted, counted, sorted, protected, and placed with direction control. If the clinic treats the number like a production target, quality can fall as the day becomes longer. Graft count should never be separated from who performs the important steps and how many people are being treated that day.
Cases Where I Reduce the Graft Number
I reduce a graft number when the cosmetic gain does not justify the donor cost. This can happen when the crown request consumes too much donor hair, the proposed hairline is too low, the donor area shows miniaturization, or active hair loss needs control before surgery.
A lower number can be the safer plan when it protects the donor area. It may mean treating the front first, leaving the crown for later, or choosing a smaller session so there are still options if native hair continues to thin.
If the number changes after examination, the reason needs to be written plainly. The plan should show the treated area, the expected graft range, the part left untreated, and why the new number is safer. A graft number change on surgery day must not feel like a surprise sales decision.
Future Hair Loss and Age Change the Calculation
Future hair loss changes graft planning. A 25 year old with active recession and crown thinning should not be planned like a 48 year old with a stable frontal pattern. Younger patients may need donor reserve for later. If too many grafts are used early, there may be no good option when hair loss progresses.
Medication response can also change the calculation. If native hair stabilizes with finasteride, dutasteride, minoxidil, or another appropriate plan, the surgical demand may become lower. If medication is not possible or not tolerated, the design has to be more careful from the beginning.
Candidacy matters before graft count. Many people focus on how many grafts they need, but the first surgical question is whether they are good candidates for a hair transplant at this stage.
Can a Norwood Scale Formula Estimate Grafts?
The Norwood scale can help describe the pattern of male hair loss, but it cannot calculate grafts accurately by itself. Two men can both look like Norwood 3 and need different numbers because their hairline height, temple recession, hair caliber, donor strength, and density expectations are different.
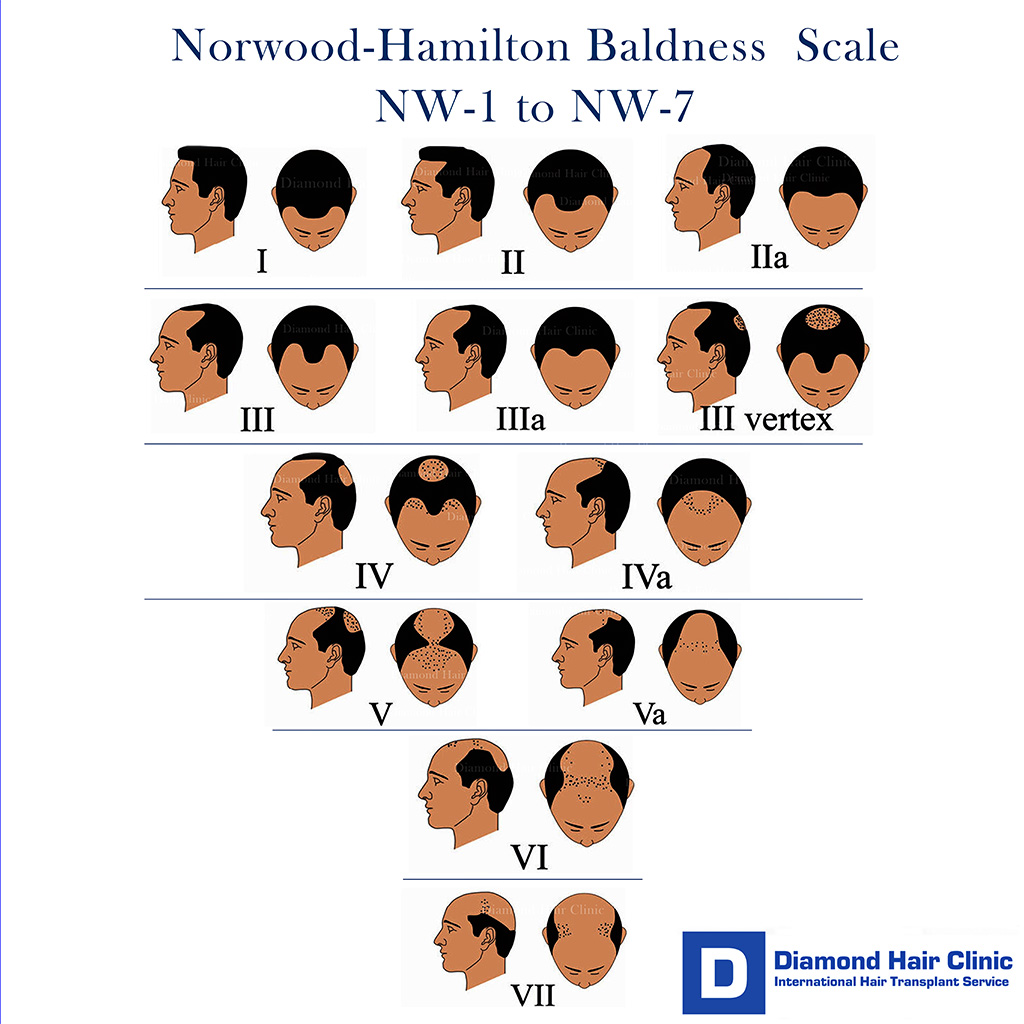
I would not use a formula such as Norwood stage multiplied by 1,100 as a surgical plan. It may give a very rough self check, but it can easily overestimate or underestimate the real need. Norwood 3 hair transplant planning may need around 1,500 grafts in a small corner case or around 3,000 grafts in a broader frontal case. The drawing and measurement matter more than the label.
Online calculators have the same limitation. They can help you understand the size of the decision, but they cannot see donor miniaturization, hair shaft diameter, crown whorl shape, scarring, or whether the planned hairline is too aggressive. A calculator can start a conversation. It cannot approve surgery.
For examples, the pages on whether 1,000 grafts can be enough, whether 2,000 grafts are enough, and whether 3,000 grafts are enough show why the same number can be small, reasonable, or insufficient depending on the area.
Written graft plan proof before surgery
A graft quote is useful only when the patient can see how the number was reached. I want the written plan to name the priority area, the estimated surface, the density goal, the donor limits, the hairline or crown strategy, and the part that may need to wait.
The plan also needs a refusal boundary. If shaving or magnification shows donor miniaturization, unstable loss, poor graft quality, or a lower safe reserve, the number has to come down. The safer decision may be a smaller front first plan, medication before surgery, or no operation at that time.
After surgery, follow up has to compare the result with the plan that was actually performed. Slow growth, uneven density, crown thinning, or donor concerns cannot be judged from the quote alone. They need the surgery notes, photos, graft distribution, and the timeline.
When I would not put the quote into a surgery plan?
I do not turn a quote into a surgical plan when the donor review is incomplete, the requested area is too wide, the hairline is too low, or the crown demand would empty the reserve needed later.
The written number also needs a safety boundary. The note has to say whether the front, midscalp, crown, scar, or repair area is the priority and what has deliberately been left for later.
After surgery, follow up uses that written plan as the reference. If the patient worries about density or growth, I compare the photos with the original treated area and the number that was actually safe to place.
Surgery Day Changes Need an Explanation
The graft number can change after shaving, donor examination, hairline drawing, and close inspection of miniaturization. A small change can be medically normal. For example, the frontal corners may need slightly more density, or the donor area may be weaker than expected and the plan should be reduced.
A surgery day change should be explained before the plan continues. It becomes concerning when it is large, unexplained, linked to pressure, or tied to a sudden extra payment after the patient is already in the clinic.
The explanation should show whether the change protects density, donor safety, hairline naturalness, crown strategy, or future reserve. If the explanation is only that more grafts are always better, be careful.
How Should You Judge a Graft Quote?
A good graft quote explains the pattern, recipient area, density target, donor assessment, hairline design, crown plan, and future reserve. It should also explain what will happen if the examination changes the number.
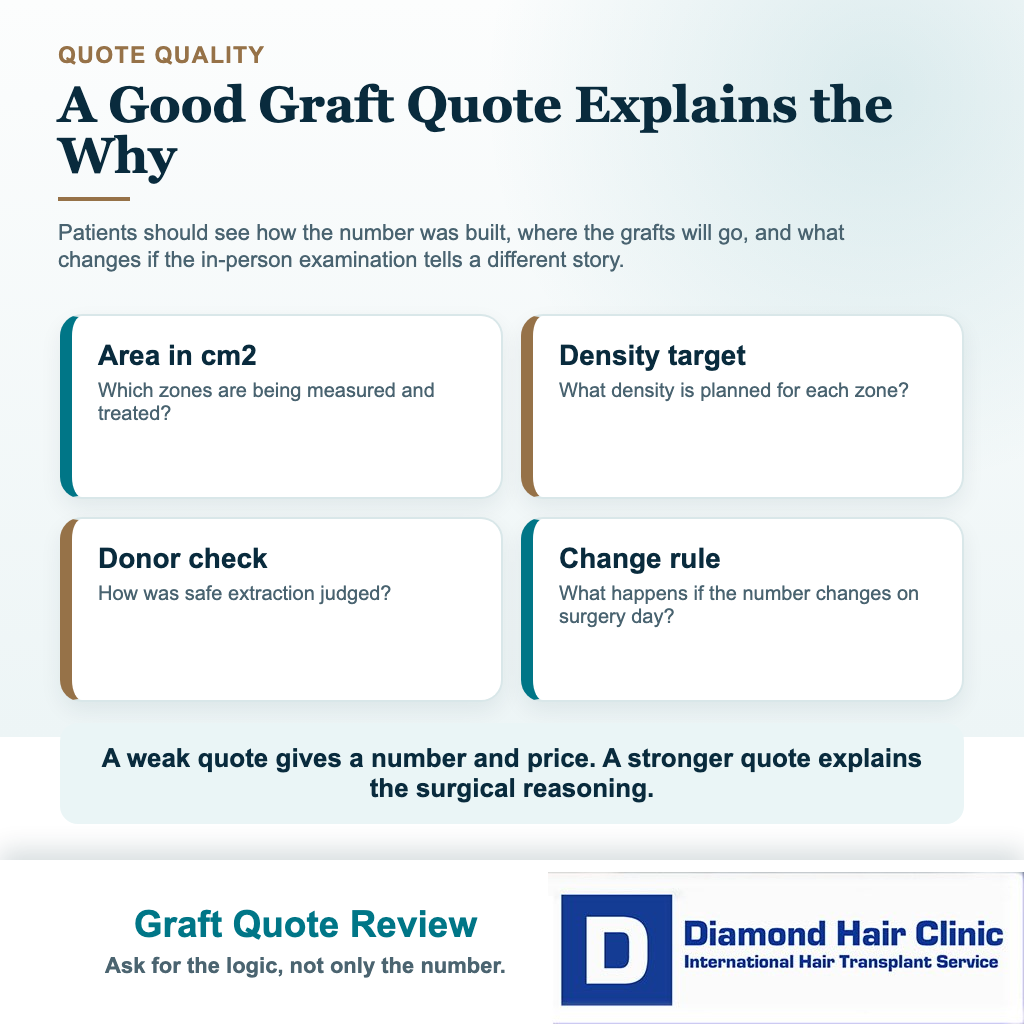
A weak quote usually gives only a number and a price. It may say 4,500 grafts without explaining where the grafts will go, how donor strength was measured, whether the crown is realistic, or how the result may look if future hair loss continues.
If two clinics give very different numbers, the higher number is not always better and the lower number is not always safer. Ask each clinic to explain the area in cm2, planned density, donor capacity, and future strategy. The page about why some hair transplant results look thin is useful when you are trying to understand why graft number alone does not predict fullness.
Also ask what happens if fewer grafts are safer than expected. A clinic that can reduce the plan when the donor area requires it is showing judgment. A clinic that can only increase the number may be treating graft count as sales language rather than surgical planning.
When I calculate grafts, the number sits inside the whole surgical plan. You need to understand what it can achieve, what it cannot achieve, and what donor cost it requires. A natural result comes from measurement, judgment, and careful distribution, not from chasing the largest number on a quote sheet.
Graft calculation is not just arithmetic when hair shaft, contrast, and hairline design are part of the decision. In Asian hair transplant planning, donor reserve and front row softness affect the graft plan before the number is accepted.