Smaller Hair Transplant Sessions Can Protect the Long Term Plan
A lower graft number can protect the donor area when it serves a clear long-term plan, but session size alone does not make surgery safe. A smaller session helps when the target is limited, the donor area needs protection, the hair loss pattern is still changing, or the first result should mature before more grafts are spent. It becomes a weak plan when each operation only chases the newest visible gap without a clear long-term design.

Session size is not the first question. What matters is whether the session makes the next decision easier. I look at the size of the thinning area, donor strength, age, hair caliber, crown involvement, medication stability, future hair loss risk, and the level of coverage you can realistically accept. A good first operation should improve the main concern now while keeping the donor area useful later.
A smaller session can be the better plan
A smaller session can be the better plan when control matters more than speed. This may apply to early temple recession, a narrow frontal weakness, a small refinement after previous surgery, or a pattern that is not stable enough for a more ambitious first operation.
The main issue is the lifetime graft budget. Donor hair is not borrowed from the back of the scalp. Once a follicular unit is removed, that exact unit has been spent from that donor location. The remaining donor must still look natural after this surgery and after any future surgery.
Staging also helps when the front and crown are competing for the same donor supply. I may need to decide which area should come first, because the frontal frame often gives more visible value per graft, while the crown can consume many grafts and still look modest under strong light.
I separate a staged plan from an incomplete plan. A staged plan has a reason, a sequence, and a reserve. An incomplete plan treats one small area because nobody has explained the bigger pattern, the crown risk, or the donor limit. A review of the one year FUE result helps decide whether the next step is planned staging, repair, or observation.
A small first session can be useful
A small first session is useful only when the target is genuinely limited. A small 1000 graft session may soften temple recession or refine a narrow hairline weakness. It cannot rebuild the frontal third, mid scalp, and crown. A 2000 graft plan can do more, but it still needs a defined target.
I also consider a smaller first step when someone is young, the future pattern is still unclear, or medical treatment before a hair transplant has only recently started. There, an aggressive hairline can look good for a short time and then become isolated as native hair continues to thin behind it.
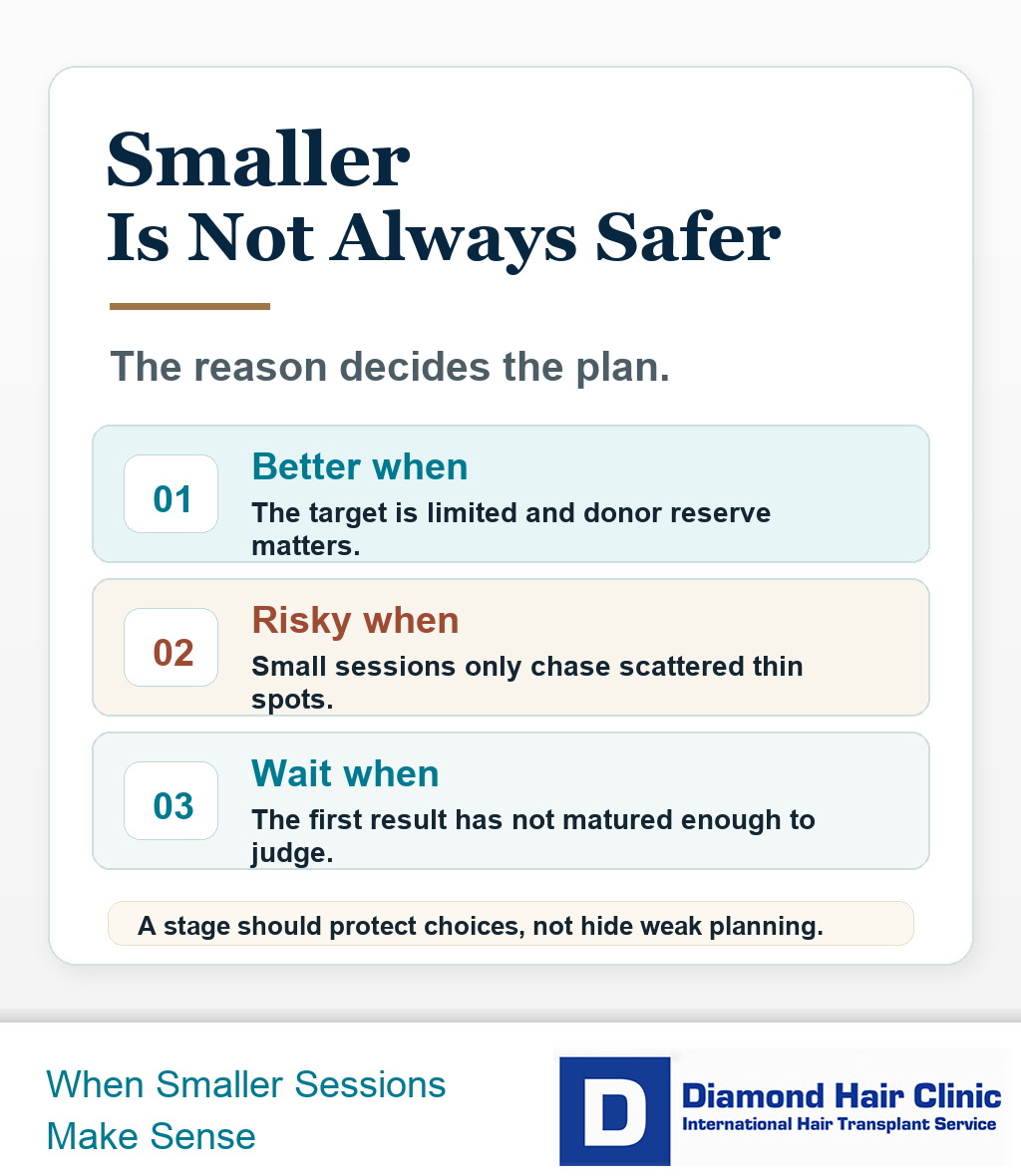
A smaller plan is strong when it protects options. It is weak when it avoids diagnosis, donor measurement, or a direct discussion about what may be needed later. Fear of a big change is understandable, but fear should not draw the surgical map. The scalp, donor reserve, and future loss pattern should.
One larger session is sometimes better
One larger session can be better when the loss pattern is stable enough, the donor area is strong, the target area is broad, and the surgical team can keep quality consistent from the first graft to the last. Splitting the work too much can create repeated healing periods without giving enough connected coverage. If the clinic is considering that longer day, long hair transplant session planning should be reviewed before assuming one session is kinder.
A broad frontal and mid scalp deficit may not benefit from a tiny operation that creates one small island of improvement. If the recipient area needs a connected design, a larger but still controlled session may be the more logical first step. A 5000 graft session can be appropriate, but only when donor strength, surgical time, graft handling, and realistic coverage goals support it together.
The mistake is thinking small always means safe. A poorly planned small session can waste grafts. A well planned larger session can be appropriate. The number alone does not decide safety.
Repeated small operations also mean repeated shaving decisions, recovery periods, shedding phases, travel, time away from work, and new anxiety while waiting for growth. If a more complete first stage can be done safely, splitting it into too many small procedures may not be kinder.
Session size alone does not protect the donor area
No. A smaller session protects the donor area only when extraction is disciplined. The grafts still need to be taken from the right zone, spread evenly, and recorded as part of the lifetime plan.
A low graft count can sound reassuring, but I still look at where the grafts come from. A small session can cause visible thinning if too many grafts are removed from one narrow zone, if the extraction pattern is uneven, or if the surgeon uses unstable donor borders. The donor area has to remain natural at the hair length you may actually wear.
I take overharvesting the donor area seriously even in moderate cases. Donor safety is a plan, not a number. The extraction map, safe zone, spacing, punch choice, hair caliber, and future reserve matter as much as the total count.
Too many small sessions can waste donor reserve
Yes. Too many small sessions can waste donor reserve when each one reacts to the latest visible concern instead of following one long-term design. The donor may become patchy, the extraction pattern may lose balance, and the top may still not have a coherent plan.
A staged plan should still know the destination. I want to know which zones matter most, how much donor capacity must be protected, what happens if the crown expands, and whether the first session still looks natural if the second session is delayed or never happens.
A small correction is different from a series of disconnected decisions. If every minor concern becomes another operation, the donor can be spent without producing a result that feels finished. The smaller the session, the clearer the reason should be.
Recovery may be easier after a smaller transplant
Sometimes recovery is less visible after a smaller transplant, but it is not invisible. A smaller recipient area may mean fewer scabs, less shaving, and less early redness. The scalp still goes through healing, washing, shedding, and a period when the change may be visible under close light.
If the main reason for choosing a smaller session is to hide the surgery, the plan can become distorted. Surgery should be sized around the clinical and cosmetic goal first. Work schedule, privacy, and shaving preference can influence the plan, but they should not replace the surgical decision.
A small operation that does not solve the visible problem can leave you recovering twice while gaining too little from the first stage. If discretion matters, I discuss hair length, shaving pattern, timing, and work obligations directly. A hidden operation is not a successful operation if the result is poorly planned.
Staging can make density decisions clearer
Staging can help density decisions when the first session creates the frame and the later session refines selected areas after growth is visible. This is most useful when density is desired in the front but grafts still need to be protected for future mid scalp or crown change.
Density is not created by forcing as many grafts as possible into one area. It comes from design, hair angle, graft selection, hair caliber, skin contrast, and whether the tissue can support the plan. A staged approach lets me judge the first growth before deciding whether more density planning is worth the donor cost.
The second stage should have a precise reason. It may soften a hairline edge, add density to a clearly thin zone, extend coverage slightly, or treat a crown that was deliberately left for later. It should not become a habit of adding grafts every time harsh lighting reveals normal scalp visibility.
Visible growth comes before the next stage is planned
In most cases, the need for another stage should not be judged too early. Hair transplant growth changes month by month, and density or crown decisions often look different once the first result has matured. A common planning window is around 12 to 18 months, especially when the question is whether to add density, extend coverage, or treat the crown.
At 4, 5, or 6 months, many results are still immature. Some areas can look thin, uneven, or delayed. Spending more donor grafts at that stage can be an emotional decision rather than a surgical one.
Waiting is not doing nothing. It gives the result time to declare itself, gives the donor time to show how it healed, and gives the next plan better evidence. If the first result already solves the main concern, the second stage may become smaller or unnecessary. If the concern remains after proper maturation, the decision is clearer.
The 3 slides here show why smaller sessions can protect donor reserve, healing, and future planning. Swipe sideways, use the arrows, or choose a number below the image.