



FUT Hair Transplant and Linear Scar Planning
FUT hair transplant, also called follicular unit transplantation or strip surgery, removes a narrow strip of scalp from the donor area and then divides that strip under magnification into follicular unit grafts. The grafts can be implanted into the recipient area in a similar way to other hair transplant methods, but what it costs the donor area is different.
FUT is not the default choice for most people asking for hair restoration today. I work mainly with FUE and Sapphire FUE because they usually fit better with donor protection, future flexibility, and shorter hairstyle expectations.
Still, FUT should not be dismissed as useless. It has a long history in hair transplantation, and in selected patients it can still be a reasonable surgical option.
FUT versus FUE should not be treated as a slogan. I look at the strip scar, scalp laxity, healing history, hairstyle plan, donor reserve, and future hair loss pattern. If those details do not support a permanent linear scar, short-term convenience is not enough reason to choose FUT.
FUT removes a donor strip and dissects grafts under magnification
In FUT, the surgeon removes a strip of skin from the back or sides of the scalp, usually from the more stable donor zone. The wound is then closed with sutures or staples, and the removed strip is dissected under magnification into naturally occurring follicular units, usually containing one to four hairs.
After that point, the surgery starts to resemble other hair transplant methods more closely. The grafts still need careful hydration, selection, placement, angle control, and recipient area planning. The main difference is not where the grafts finally go. It is how they are harvested and what that harvesting leaves behind.
This distinction matters more than many patients initially realize. The donor area is limited. It is not an unlimited source, and every harvesting method leaves evidence. The donor strategy is not a side issue. It is central to the entire surgery.
The same donor logic applies when I discuss whether the donor area can look normal after FUE, because every harvesting choice changes what remains possible later.
FUT and FUE differ mainly in the donor footprint
In an FUE hair transplant, follicular units are removed one by one with small punches. In FUT, a strip of scalp is removed first, and the follicular units are separated from that strip outside the body. Both methods can produce grafts for implantation, but the donor footprint is very different.
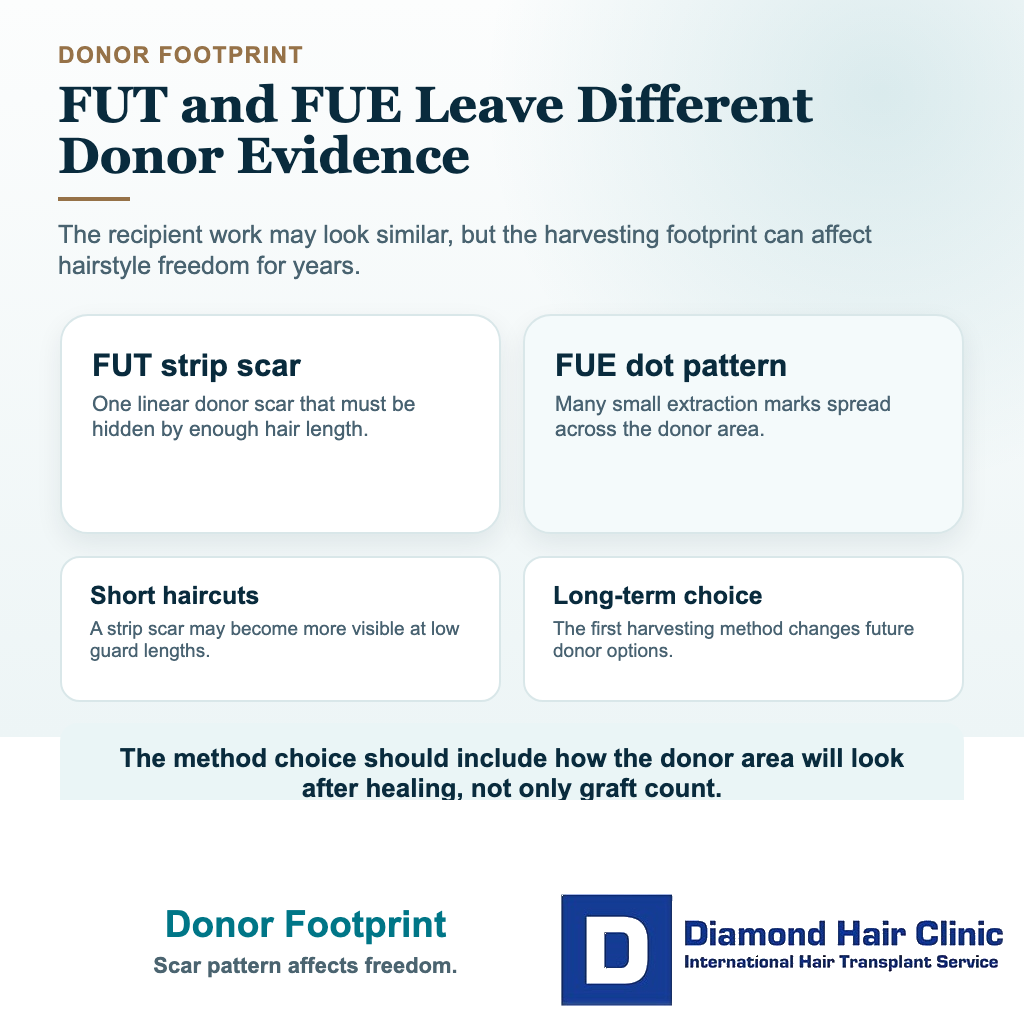
FUE usually leaves many small dot scars spread across the donor area. FUT usually leaves one linear scar.
This does not mean FUE leaves no marks. If FUE is overdone, poorly distributed, or shaved very short later, dot scarring or patchy donor depletion can still become visible. The difference is that FUT creates one line that has to be planned around for the rest of that person’s life.
A man who wants a very short haircut may tolerate tiny scattered FUE marks more easily than a strip scar. Another patient with longer hair, good scalp laxity, stable donor density, and no short hair goal may view the tradeoff differently.
Once a linear scar exists, it becomes part of the donor area permanently. Even if it heals thin and remains hidden under longer hair, it is still a surgical mark. That needs to be understood before surgery, not after.
Why did FUE become the modern default for many patients?
FUT lost popularity because patient expectations changed and FUE improved.
Patients increasingly wanted less visible donor evidence, more freedom with hairstyle choices, and a procedure that felt less invasive from their own point of view. At the same time, FUE instruments, magnification, punch control, graft handling, and extraction planning improved.
FUE is not superior in every possible scenario, and I avoid talking about hair transplantation in absolute terms. But for many patients, FUE fits better with a donor area without a linear scar, more flexibility for future haircuts, and a surgical approach that is easier to accept psychologically.
The caution is still important. A modern technique label does not protect the donor area by itself. FUE only becomes safer when the extraction pattern, total number, spacing, donor strength, and future hair loss plan are controlled well.
When can FUT still make sense?
FUT can still be considered in selected donor plans.
A more reasonable FUT candidate usually has strong donor density, good scalp laxity, realistic expectations, no history that strongly suggests raised or widened scarring, and no desire to wear the donor area very short. That person also needs to accept that even a strip scar that heals well is still permanent.

In some high graft demand cases, or in certain complex restoration strategies, FUT may be part of the discussion. It can also be considered when the plan aims to preserve parts of the donor area from widespread punch extraction. Even then, the reason has to be specific to the patient, not a routine clinic habit.
The opposite profile matters just as much. FUT becomes harder to justify when the scalp is tight, the donor is weak or unstable, the patient prefers very short hair, previous surgery has changed scalp movement, diffuse thinning may involve the donor area, or the patient is being sold a large strip session mainly because it sounds like many grafts.
A larger first surgery is not better if it narrows future options. A good strip plan usually means careful strip width, careful level, tension control, closure planning before tissue is removed, and a clear explanation of what happens if the scar widens.
Short haircuts, tight scalps, and scar history need extra caution
I become more cautious about FUT when a patient likes short haircuts, has a tight scalp, has a history of thick or raised scars, already feels anxious about visible evidence of surgery, or may need several future procedures. These details can change the whole donor strategy.
A very short hairstyle changes the conversation. The question is not only whether the scar can be hidden under longer hair. The question is how it may look at a number two or number three guard, under bright light, after future hair loss, or after another surgery.
I am also careful when avoiding shaving is presented as the main reason for FUT. That can matter for privacy, especially for some women or people who work in front of others, but it should not hide a weak donor plan. In women with diffuse thinning or unstable donor density, privacy is not the main issue. Donor stability is.
Before accepting FUT, the scar plan, hairstyle limits, closure approach, possibility of scar widening, and later repair options should all be clear. Ask whether trichophytic closure or scar revision is being discussed realistically, not as a promise that the scar will disappear. That is not fear. It is informed consent.
The main FUT tradeoffs are scar, recovery, and flexibility
The main disadvantage is the linear scar.

Even when a scar heals well, it remains a permanent line in the donor area.
In some patients it stays very fine. In others, it can widen over time. Scar width is influenced by surgical technique, closure quality, scalp tension, the patient’s scar biology, and how the scalp behaves during healing.
I avoid reassuring patients too easily with sentences like the scar will be invisible. A scar may become subtle. It may be hidden well. But no ethical surgeon should speak as though a strip scar does not matter.
Recovery can also feel different from FUE. Sutures or staples need care, and some patients feel tightness, numbness, pulling, or sensitivity in the donor area during the early period. Many recover smoothly, but the donor area can remain more noticeable for some patients while the wound settles.
Flexibility is the third tradeoff. A patient who later wants to wear a very short haircut may realize that the donor scar limits that freedom. This is a long-term lifestyle question, not a small technical detail.
A strip scar can become a real donor area problem
Sometimes the scar remains thin and acceptable. Sometimes it does not.
A widened scar can frustrate someone years later, especially if hairstyle preferences change, surrounding hair thins, or the donor area no longer feels as normal as expected. A scar can also bother a person psychologically even when it looks acceptable to someone else.
This part matters more than many clinics admit. Hair restoration is not only about whether something looks reasonable under clinic lighting or in standardized photographs. It is also about whether the patient feels comfortable with what was done to his scalp.
Repair options exist, but they need realistic language. Trichophytic closure, scar revision, scalp micropigmentation, or FUT scar camouflage with FUE may help selected scars. None of them erases the original decision or restores an untouched donor area.
I discuss the scar before surgery in the same practical way I discuss the recipient result. The donor area is part of the cosmetic outcome.
Avoiding shaving should not drive the FUT decision
Patients hear this argument often, and it can sound attractive.
Avoiding shaving can be useful in certain situations. Some patients value privacy strongly, some women may prefer to avoid large visible shaved areas, and some men do not want people around them to notice surgery immediately.
I understand that, but social convenience in the first weeks should not dominate the donor decision. A procedure that is easier to hide in the short term is not necessarily the better operation over the long term.
A hidden scar is still a scar. If FUT is being chosen mainly to avoid shaving, I slow the conversation down and look again at scalp laxity, donor density, future hair loss, scar risk, and hairstyle goals.
I recommend choosing the harvesting method that fits the medical and aesthetic plan, not the method that creates the easiest social story for the first month.




Graft quality depends on judgment, not the harvesting acronym
Some patients are told that FUT automatically gives better grafts because the strip is dissected under magnification. That is too simple.
Microscope dissection can be useful. So can careful FUE extraction. What matters is how the tissue is removed, how the grafts are dissected, how long they spend outside the body, how they are hydrated, how they are sorted, and how carefully they are placed into the recipient area.
A poorly planned FUT can still damage tissue, create a poor scar, or waste donor capacity. A carefully planned FUE can still produce excellent grafts when extraction, handling, and placement are controlled well.
In hair transplantation, technique matters, but judgment matters even more. Patients are often encouraged to compare acronyms, but the safer comparison is the thinking behind the method.
That surgeon-led way of thinking is also part of how I have built Diamond Hair Clinic and how I approach my own cases.
FUT fits fewer modern expectations because the donor cost is permanent
In FUT planning, the donor scar often decides the discussion.
They want a natural recipient result, a donor area that remains cosmetically acceptable, and freedom to keep shorter hairstyles if they choose. FUT can still create natural recipient area work when the surgery is performed well, but the donor cost is different.
Many people today are less willing to accept a linear scar as part of that cost. That is understandable.
FUT should not be recommended in a routine or automatic way. The reason must be clear. If a clinic recommends strip surgery, the person needs to understand why this method is being chosen for this donor area, this hairstyle plan, and this future hair loss pattern.
Where I still place FUT in modern planning?
I consider FUT a legitimate hair transplant method with historical importance and real surgical value in selected cases. I am not against it as a technique.
But it is not my default choice for most patients. In my own practice, I generally plan around FUE because it fits better with donor management, visible donor evidence, future flexibility, and the way many patients want to wear their hair later.
I try to preserve as much future freedom as possible. Once a linear scar is formed, that freedom narrows. That is the main reason I lean away from FUT in routine modern practice.
Questions to ask before agreeing to FUT
Someone considering FUT needs direct answers before committing to the operation, because the most important details are usually not the marketing words but the surgical responsibilities behind them.
Before accepting FUT, make sure you understand who removes the strip, who closes the wound, how closure tension will be minimized, why the donor area is suitable for strip surgery, and what hairstyle limits may remain after healing.
Ask to see examples that match your intended haircut length, not only scars hidden under long donor hair. Ask what happens if the scar widens, whether trichophytic closure or later scar revision is realistic, and whether FUE into the scar would only camouflage rather than undo the problem.
Also ask why FUT is being recommended for this specific case. Is it truly the best long-term plan for your donor area, or is the clinic simply more comfortable with strip surgery operationally?
The method should serve the person having surgery. Do not accept pressure toward a method simply because it fits the clinic’s habits, staffing structure, or technical comfort zone.
FUT and FUE can be combined only with a lifetime donor plan
In some long-term restoration plans, both methods may appear across a patient’s lifetime.
FUT first and FUE later is one sequence, which I explain separately in the FUE after FUT discussion. With FUT first, the strip scar has to be respected when later FUE extractions are planned around it.
The reverse sequence needs a different donor review. If FUE was done first, the question becomes whether strip surgery after previous FUE can still be planned without crossing an already weakened or thinned donor zone. Previous harvesting narrows the safety margin.
For me, the lifetime donor plan should be considered before the first surgery, not only after problems appear.
Every harvested graft comes from a limited reserve. Every surgery changes what remains possible later. Someone may focus heavily on the first result, but the surgeon should be thinking much further ahead than that.
That is also one of the reasons I generally favor careful, flexible donor planning from the beginning.