



Choosing Hair Transplantation for Hair Loss
Hair transplantation can be the right choice when your hair loss pattern, donor area, age, expectations, and long term plan all support surgery. It is not the right choice just because a clinic says you can have many grafts, or because you feel tired of hiding thinning hair. The answer is case dependent, and the factor that changes the answer most is not the bald area alone, but the quality and future of the donor area.
I explain it from the patient’s real decision. A hair transplant moves hair from a stronger area to a weaker area, but it does not create unlimited new hair. My priority is always quality over quantity. If surgery is planned well, it can make the face look more balanced, the hairline more natural, and the thinning area easier to manage. If it is planned poorly, it can waste grafts that the patient may need later.

Changes created by hair transplantation
Hair transplantation changes the distribution of your existing permanent hair. In most patients, the stronger hair is taken from the back and sides of the scalp and moved to thinning or bald areas. This transplanted hair is placed as small follicular units, which are natural groupings of 1 to 4 hairs.
This is the useful part of the traditional explanation, but it is not enough for real decision making. The patient usually asks what is being moved, while the surgeon must also ask what is being protected. Every graft removed from the donor area leaves that donor area with one less available follicular unit. This is not dangerous when extraction is controlled, but it becomes a problem when a plan treats the donor area like an unlimited supply.
Hair transplantation can also be used in other areas, such as eyebrows, beard, or scars after injury or previous surgery. The principle is similar, but the planning is not identical. Beard hair, eyebrow direction, scar tissue, and scalp hair all behave differently. A medically sound plan must respect the biology of the area being treated.
For scalp hair loss, the central idea is donor dominance. Hair from the safer donor zone usually keeps more of its original resistance after it is moved. But that does not mean every hair on the back of the head is equally safe forever. The surgeon still has to decide where extraction should happen, how widely it should be spread, and whether the patient’s donor area is stable enough.
A good transplant does not simply fill empty space. It creates the appearance of coverage by choosing the correct grafts, angles, density, and placement. I am not trying to copy the density you had as a teenager. The purpose is to create a natural result that still makes sense when you are older and when your native hair continues to change.
Another optical part that patients sometimes underestimate. A surgeon is not only counting hairs. He is deciding where each type of graft will create the greatest visual value. Fine single grafts belong in the soft front edge, stronger grafts can support the area behind it, and the direction must respect how hair naturally exits the scalp.
If this planning is poor, even a large number of grafts can look artificial or thin. If the planning is careful, a moderate number of grafts can create a better visual result because the hair is placed where it matters most. The operation must be designed before it is counted.
Hair transplantation also has limits. It does not stop future hair loss. It does not make weak native hair stronger by itself. It does not guarantee full density across every thinning area. It can improve coverage and facial balance, but it must work together with diagnosis, long term planning, and sometimes medical treatment.
I avoid planning surgery only from one photograph of the hairline. Hair transplantation is a surgical redistribution of a limited resource. When a patient understands that, the whole conversation becomes more serious, more reliable, and more useful.
Suitable candidates for hair transplantation
A good candidate is not simply a person with visible hair loss. A good candidate has a pattern of loss that can be planned safely, a donor area that can support the goal, and expectations that match what surgery can realistically achieve. Age matters, but age alone does not decide everything.
In consultation, I look at the donor area, the degree of miniaturization, the family pattern, the crown, the front, hair caliber, scalp contrast, medication history, previous surgery, and how quickly the hair loss is changing. A patient with stable loss and a strong donor area may be a good candidate. A younger patient with diffuse thinning, weak donor density, and fast progression may need medical treatment and observation before surgery.
I often tell patients that being told to wait is not rejection. Sometimes it is protection. If you are unsure whether your case is ready, the more detailed discussion on being a surgery is a good fit is worth reading before you commit to a date.
The emotional part also matters. Some patients are steady and want a realistic improvement. Others are desperate for a dramatic change and become vulnerable to clinics that promise too much. I take that seriously, because anxiety can push a patient toward a decision that feels relieving today but becomes difficult later.
I watch whether the patient understands the limits of surgery. A patient who wants improvement and accepts staged planning is usually easier to help than a patient who wants every thin area filled immediately. The second patient may still be operable, but the consultation must slow down, because the weaker point is not only technical. The weaker point is that the patient may agree to a plan that cannot age well.
A proper candidacy assessment should also separate different types of thinning. A receding frontal hairline, diffuse thinning through the top, crown loss, and donor miniaturization are not the same problem. If these patterns are mixed together, the patient may receive a plan that looks simple but does not fit the diagnosis.
I also consider lifestyle and hairstyle. A patient who wants to keep the hair very short after surgery needs a donor plan that is even more careful. A patient who uses hair fibers, styles the hair forward, or has a high contrast between scalp and hair color may need a different density strategy. These details are not small. They change how natural the result will look in daily life.
Cases that should not rush into hair transplantation
Patients need to not rush into surgery when hair loss is still changing quickly, the donor area is weak, the diagnosis is unclear, or the expectation is to restore teenage density. Surgery may still be possible later, but the first decision should protect the patient.
Very young patients, diffuse thinning, unstable crown loss, and anxiety driven decisions all need a slower consultation. In these cases, a period of observation or medical treatment can be more responsible than booking surgery immediately.
Diffuse thinning and hair transplant planning shows why a transplant can be risky when weak native hair and donor uncertainty are not separated carefully.
Safe graft number decisions
The safest graft number is not the biggest number a clinic can extract. It is the number that improves the recipient area while still protecting the donor area for the future. This is a common misunderstandings in hair transplantation.
Patients often compare offers from different clinics and feel confused when one clinic says 2,500 grafts and another says 5,000. A higher number can sound more generous, but it can also be a sign that the clinic is chasing coverage without enough respect for donor management. It is better to plan fewer grafts well than create a larger surgery that looks impressive on paper but weakens the patient’s future options.
Graft planning should start with diagnosis and design. The surgeon should ask which areas matter most visually, how much native hair may continue to thin, whether the crown should wait, and how much density is safe for the scalp. A proper graft number is a clinical decision, not a sales number.
There are cases where a large session is appropriate, but it should never be presented as automatically better. If the donor area is weak, if miniaturization is present, if the crown is large, or if the patient is young and still losing hair actively, a restrained plan may be wiser. The decision is not simply how many grafts can be taken today. The question is how the patient will look after this surgery, and after the next years of hair loss.
When I reduce a graft number, it is not to create a smaller result. It is to help the result survive real life. A hair transplant should still look natural when the hair is shorter, when the patient is under harsh light, and when future thinning reveals more of the scalp. That requires leaving the donor area with enough reserve.
I check hair caliber. Thick, wavy hair can create stronger coverage with fewer grafts. Fine, straight, high contrast hair often needs more careful expectations because the scalp shows through more easily. Two patients with the same number of grafts can have very different visual outcomes.
The size of the recipient area matters too. A small hairline correction and a wide Norwood 6 pattern are not comparable operations. A large graft number is not a plan unless it explains the surface area, expected density, and donor consequence. Without that context, the patient has received a number, not real planning.
My preference is to use grafts where they make the strongest visual difference. For many men, that means the frontal frame first. Once the face is framed naturally, the whole appearance can improve even if every thinning area is not filled heavily. This is often more responsible than spreading grafts too thinly across a very large area.
During the hair transplant procedure
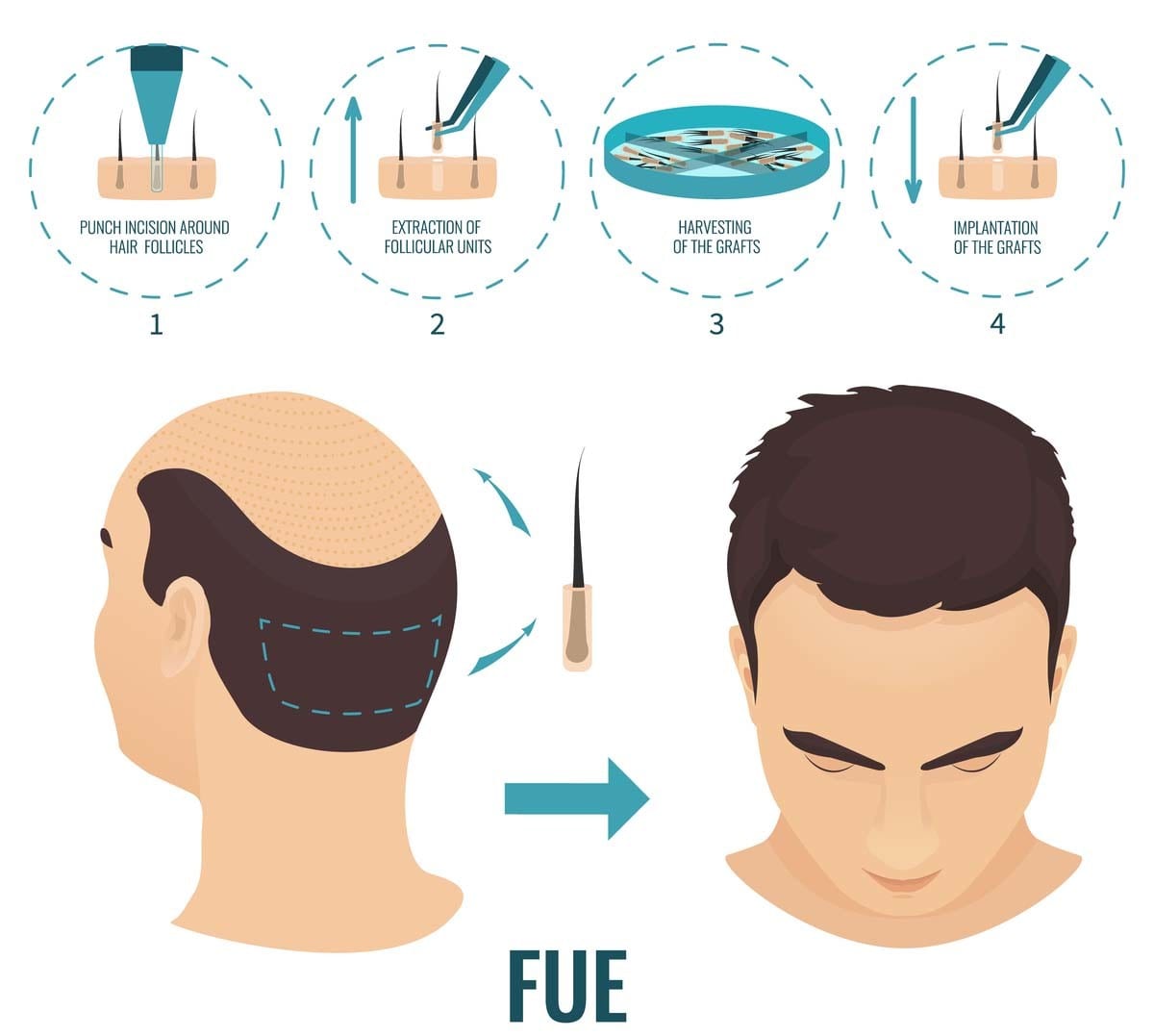
The procedure has several main stages. First, the patient is evaluated and the surgical plan is confirmed. The hairline and recipient area are designed, the donor area is prepared, local anesthesia is applied, grafts are extracted, recipient area incisions are created, and the grafts are placed carefully.
Patients sometimes think the extraction method is the whole procedure, but it is only one part. The artistic and medical quality of the result depends heavily on recipient area planning. The angle, direction, density, and distribution of the incisions decide whether the hair will grow in a natural direction and whether the result will frame the face properly.
I use Sapphire FUE for recipient area incisions because I believe this step deserves direct surgical control and precision. A tool does not replace surgical judgment, but the right tool in experienced hands can support careful planning.
The grafts themselves must also be handled gently. They are living tissue, not simple cosmetic fibers. Time outside the body, dehydration, trauma, poor sorting, and rushed placement can all affect the final result. I do not view hair transplantation as a fast cosmetic service. It is a long surgical day that rewards patience, discipline, and a team that understands the value of every graft.
One detail I discuss with patients is responsibility during the operation. Many advertisements make the procedure sound like a machine based service. In reality, judgment is needed at every stage. If the hairline is changed during surgery, if the donor area shows unexpected weakness, or if the graft count must be adjusted, the surgeon should be present enough to make that decision safely.
The first surgical day is not only about what happens in the operating room. It begins with confirming the plan again when the patient is physically present. Photos can help, but they do not replace direct assessment of scalp laxity, donor density, hair caliber, miniaturization, and the real shape of the head.
Local anesthesia is used so the patient can undergo the procedure without feeling the surgical work. Some patients fear this part more than the transplant itself. I understand that, because the idea of scalp injections can sound uncomfortable. In a proper clinic, comfort is managed seriously, but patient safety remains the priority.
After extraction, grafts should be sorted in a way that supports the design. Single hair grafts have a different role from 2, 3, or 4 hair grafts. If this sorting is careless, the hairline may look harsh or the density may be wasted in the wrong place. Here, surgical planning and team discipline meet.
Decisions before the surgery day
Before surgery day, the patient needs to understand the diagnosis, donor capacity, hairline plan, estimated graft number, priority areas, and what will intentionally be left lighter. A serious plan should not be invented under pressure on the morning of surgery.
The surgery day may still require small adjustments after direct examination, but the patient needs to not arrive with only a package name and a graft promise. He should know why the plan fits his case and what would make the surgeon reduce or change it.
Instructions before hair transplant surgery matter because preparation is not only about logistics. It is also about making sure the medical plan is understood before travel.
FUE, FUT, and case fit
FUE and FUT are different ways of harvesting grafts from the donor area. FUE removes follicular units one by one with small punches. FUT removes a strip from the donor area and then separates the grafts under magnification. Both methods can produce natural results when performed properly, and both can produce poor results when planning is weak.
FUE is popular because it avoids a linear scar and usually allows shorter hairstyles than FUT. It is also the method I usually prefer in my own practice. But FUE is not magic, and it is not scarless. If too many grafts are extracted, or if the extraction is spread poorly, the donor area can look thin or patchy.
FUT may still have a role in selected cases, especially when a patient wears the hair longer or needs a strategy that preserves certain donor options. I do not present FUT as outdated for every person, but I also do not use it as my usual method. Strip surgery may still be considered. That timing belongs in FUT hair transplant.
The bigger point is simple. The method is not the full plan. Patients need to not choose a clinic only because it advertises FUE, DHI, Sapphire FUE, or any other label. The deciding detail is whether the donor area was evaluated, whether the hairline suits the patient’s face and age, whether the recipient area is created with surgical judgment, and whether the plan protects the future.
I often see patients become focused on method names because those names feel easier to compare. But the same method can produce very different outcomes in different hands. FUE with poor extraction can damage the donor area. FUT with poor closure can leave a visible scar. Sapphire blades used without aesthetic planning do not simply create a natural result. The method matters, but the person planning and performing the critical steps matters more.
DHI is another term patients often ask about. It usually refers to implantation with implanter pens, not to a completely different biological principle. This should not be reduced to whether a clinic uses a fashionable name. The decision depends on whether the grafts are protected, whether the direction is controlled, and whether the surgical plan is appropriate for that patient.
Robotic systems and motorized punches can also sound advanced, but technology still needs judgment. A device can assist with extraction, yet it cannot decide the correct long term hairline, the emotional maturity of the patient, or how much donor reserve should be saved. Those decisions remain medical decisions.
Hairline design matters
The hairline is usually the first thing people notice after a hair transplant. It frames the face, changes the perceived age, and determines whether the result looks natural in real life. A dense but unnatural hairline is not a success in my eyes.
Natural hairline design requires moderation. The line should match the patient’s age, facial structure, hair caliber, donor capacity, and future hair loss. A very low hairline can look attractive in a drawing, but it may consume too many grafts and create an artificial appearance later.
The small details matter. Single hair grafts should be used at the front, angles should follow natural direction, irregularity should be controlled, and density should match the available safe donor supply. I see natural hairline design as a surgical and artistic decision, not just a shape drawn before the operation.
I also tell patients not to judge a hairline only from a dramatic before and after photo. Lighting, styling, hair fibers, wetness, hair length, and camera angle can change perception. A strong hairline should look appropriate when the hair is dry, short, moving, and seen from normal distance.
A natural hairline is also not a perfectly straight line. Real hairlines have softness, small irregularities, and a transition from finer front hairs to stronger hairs behind. If the front is built with thick grafts or placed too low, the patient may gain density but lose naturalness. That is not a good exchange.
Temple points deserve special caution. They can improve facial framing in specific cases, but they also expose poor planning quickly because the angles are demanding and the hair must lie naturally. If the patient does not have enough donor reserve, or if future loss is likely to progress, aggressive temple work can make the whole design harder to maintain.
I also consider the patient’s ethnic hair characteristics. Curly, wavy, straight, coarse, and fine hair do not behave the same way. The angle of exit, curl pattern, and density impression must be adapted to the person. A copied hairline design from another patient is rarely the best plan.
Crown coverage in one session
Sometimes the crown can be improved in the same session, but it should not simply be treated the same way as the hairline. The crown often consumes many grafts because of the spiral pattern and the way light hits the scalp. It can look thin even after a technically good transplant if expectations are too high.
When a patient has both frontal loss and crown thinning, I usually think first about what will give the greatest visual improvement and the safest long term plan. For many patients, restoring the front and framing the face creates more visible benefit than trying to fill the entire crown heavily in one operation.
A crown hair transplant needs planning with particular caution in young patients, patients with active thinning, and patients with limited donor capacity. The crown can expand over time. If all grafts are used too early, the patient may later have a dense island surrounded by thinning native hair.
This belongs among the areas where surgical judgment matters more than patient enthusiasm. I understand why crown thinning bothers patients, especially under bright light. But the plan must protect the donor area and avoid creating a result that looks good for a short period and difficult later.
Sometimes the best crown plan is not no crown work. It may be limited crown work. It may be waiting until medication response is clearer. It may be accepting lighter coverage so the front can be stronger and the donor area remains usable. This is not a lack of ambition. It is long term planning.
The crown also matures slowly in many patients. Even when the surgery is done well, the visual change may take patience because the area is wide and the hair angle changes around the whorl. A patient who expects instant full coverage may feel disappointed even after a medically reasonable plan.
In advanced hair loss, I sometimes prefer to create a natural transition rather than chase full coverage. This can mean a stronger front, a reasonable mid scalp, and a crown that is improved but not made unrealistically dense. This type of planning may sound less dramatic, but it often ages better.
Recovery expectations after surgery
After surgery, the first days are about protection and healing. The recipient area has small scabs, the donor area may feel sore or tight, and the patient must follow washing and sleeping instructions carefully. At Diamond Hair Clinic, I follow patients closely in the early period, including the second day check and the 10 day washing process.
The transplanted hairs often shed after the early healing phase. This can make patients anxious, but shedding of the hair shaft is part of the normal cycle often. The graft root can remain under the skin while the visible hair falls. Growth then develops gradually over months, and I evaluate final maturation over a much longer period, often up to 18 months.
Patients should not judge the final result from day 10, month 2, or even month 5. Early redness, uneven shedding, temporary thinning, and slow changes can create unnecessary panic. If you need help understanding the emotional side of monitoring progress, Constant comparison can be misleading. Keep that in mind with tracking hair transplant growth.
There are still warning signs that deserve attention. Increasing pain, spreading redness, pus, fever, trauma to the grafts, or a sudden change that does not match the clinic’s instructions should be reviewed with the surgeon. Calm observation is useful, but silence in the face of a real concern is not.
The recovery period is also when many patients start comparing themselves with other people. This can be misleading because scabbing, redness, shedding, and early growth vary. My preference is patients to follow their own healing pattern with consistent photos and direct communication, rather than judge the surgery from random daily comparisons.
Shock loss can also occur. This means some native hair may shed temporarily after surgery, especially when the area already contains miniaturized hair. It can be emotionally difficult because the patient may feel the transplant made things worse at first. Often this improves with time, but it should be assessed properly if the thinning is severe or prolonged.
The donor area also changes during healing. Early redness, patchiness from shaving, scabs, and uneven regrowth can make patients worry. The deciding detail is whether the extraction pattern was safe and whether the donor area settles naturally as hair grows back. A healthy recovery needs judgment over time, not from one anxious early photo.
Aftercare instructions matter because early trauma can damage grafts. Washing, sleeping, sun exposure, exercise, alcohol, smoking, and touching the grafts should follow the clinic’s instructions. I am cautious when aftercare is vague. The patient needs to know what to do, when to do it, and when to contact the clinic.
The next 5 slides turn the recovery points into quick visual reminders. You can swipe sideways, use the arrows, or choose a number below the image.

Aftercare details before committing
Before committing, the patient needs to know how washing is taught, when photos are reviewed, who answers urgent questions, how swelling is handled, and what symptoms need medical review. Aftercare should not begin only after the patient has already flown home.
A strong clinic makes recovery feel structured. The patient needs to understand the first wash, sleeping position, exercise limits, sun protection, medication instructions, and the normal shedding timeline.
The full hair transplant aftercare guide gives more detail on why recovery instructions should be part of the clinic decision, not an afterthought.
Judging a clinic promise before booking
When deciding whether hair transplantation is the right choice, the patient needs to not judge the clinic only by excitement, price, or a graft number. He needs to understand how the donor area was evaluated, why the graft number was chosen, and whether the hairline suits his face, age, and future hair loss pattern.
The plan should also explain medication where relevant, crown progression, possible future sessions, and the limits of surgery. This is not meant to make the patient afraid. It is meant to make the decision clearer and more reliable.
A fast yes is incomplete when the consultation does not explain what surgery cannot do. The patient needs to feel informed, not pushed.
Waiting can be better than surgery
Waiting is better when the diagnosis is unclear, the hair loss is changing quickly, the donor area looks weak, the expectations are unrealistic, or medication has not been considered in a patient who may benefit from it. Waiting can feel frustrating, but sometimes it protects the patient from a surgery that would be technically possible but strategically unwise.
This is common in younger patients with diffuse thinning. If the native hair is miniaturizing across the top and the donor area is not strong, surgery may not improve the situation enough. It may even make future planning harder. In these cases, medical treatment, observation, and repeated assessment can be more responsible than rushing to operate.
Medication is not a substitute for surgery when the hairline is already gone, but it can change the plan in patients with active miniaturization. A proper discussion about medication before surgery can help reveal whether the native hair can stabilize, whether the crown may improve, and whether the transplant should be smaller or delayed.
Waiting can also be wiser after a previous poor transplant. A repair plan should not be rushed while the scalp is still healing, while redness is active, or while the final growth is unclear. Repair surgery has fewer options than first surgery because some donor grafts have already been used and some recipient areas may contain scarring or unnatural grafts.
A correct decision can be more precise than approval or rejection. Surgery may be reasonable as a smaller plan, focused only on the front, delayed until after medication, postponed for the crown, or considered only if the donor area proves strong enough in person. These distinctions are where a careful consultation becomes more valuable than a quick quote.
Make the decision carefully. Choose hair transplantation when the plan is realistic, medically safe, and designed for your future, not only for your next photo. A natural result comes from careful design, protected donor capacity, realistic density, and surgeon-led planning. If a plan respects those limits, hair transplantation can be life changing in a quiet and natural way. If it ignores them, the patient may pay for that decision for many years.