Can Transplanted Hair Grow in Scar Tissue?
Yes, hair can sometimes be transplanted into scar tissue after an injury, burn, hairline lowering surgery, old strip surgery, or another scalp operation. It is less predictable than transplanting into healthy scalp, so I do not judge it from the empty patch alone.
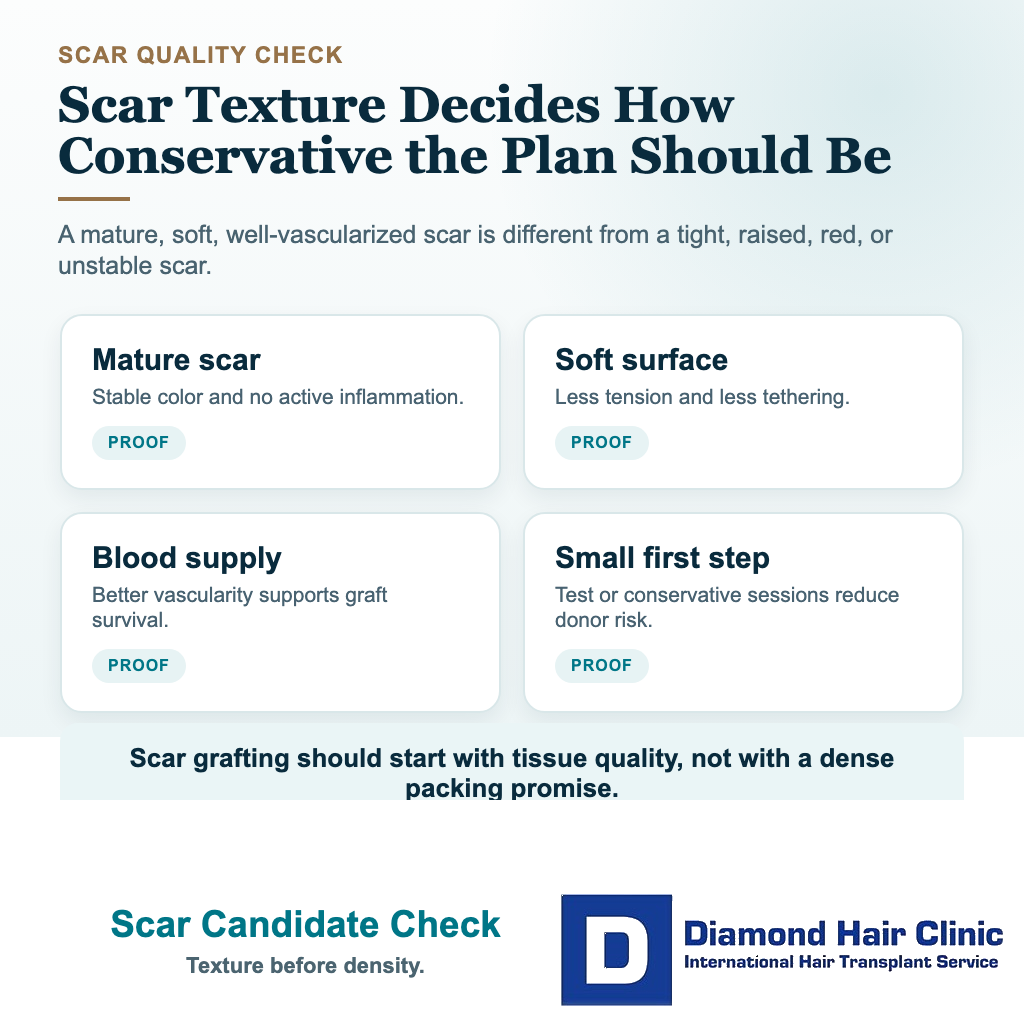
The key question is whether the scar has enough blood supply, softness, maturity, and surrounding hair to make grafting worth the donor cost. A scar that looks small in a photo can still be tight, thick, or poorly mobile when examined.
A flat, mature, soft scar may respond well to careful grafting at lower density. A raised, tight, painful, red, unstable, or very wide scar may need waiting, dermatology treatment, scar revision, scalp micropigmentation, or no surgery at all. A scar after tinea carries the same logic. Hair transplant after tinea capitis depends on scalp calmness and scar quality, not just an empty patch.
I also separate a stable physical scar from an active scarring condition. An old injury scar may be a camouflage question. Lichen planopilaris, discoid lupus, dissecting cellulitis, CCCA before hair transplant, or another active inflammatory process is diagnosis planning first, not simple scar camouflage. The same caution applies to beard transplant planning for facial scar areas, because visibility with a close shave and hair direction make small mistakes harder to hide.
Scar tissue can accept grafts only in selected cases
Scar tissue can grow transplanted hair in selected cases. The graft is not trying to wake up an old follicle inside the scar. It is a living follicular unit moved from the donor area into a new place, and it needs the recipient area to heal around it.
The difficulty is that scar tissue is not normal skin. It may be firmer, thinner, less flexible, and less vascular than the surrounding scalp. That means the grafts may not receive the same support they would receive in an untouched recipient area.
I describe scar cases as camouflage, not erasure. A good result can soften the contrast between the scar and surrounding hair. It should not be sold as making the skin exactly like it was before the injury. The same distinction matters when SMP is considered after a thin transplant result. Pigment can soften contrast, but it cannot make scar tissue normal skin.

What makes scar tissue different from normal scalp?
Healthy scalp has a natural blood supply, flexible tissue, and a predictable skin layer for creating recipient incisions. Scar tissue can have less circulation and more fibrous texture. Some scars feel flat and soft. Others feel tight, shiny, thick, or tethered to the deeper tissue.
When I plan a standard FUE hair transplant, I can usually predict the recipient area more confidently. In a scar, the plan has to be more conservative because the tissue may not nourish every graft equally. The edge of a scar near healthy scalp can behave differently from the tight center of a wide scar.
High density is not the first aim in this tissue. Survival, natural direction, and a softer visual break come first. If the scar accepts the first session well, a second small session can sometimes improve coverage later.
When should a scar be left to mature before surgery?
A new scar should usually be left alone until it has matured. For some patients, that means waiting at least 6 to 12 months before making the decision whether grafting is sensible. Some scars need longer, especially after burns, wider surgery, infection, or repeated revision.
Early redness, firmness, itching, and color change can improve with time. If surgery is done while the tissue is still changing, the surgeon may be judging the wrong scar. You may spend donor grafts on an area that would have become less visible with proper healing.
Symptoms matter because they can show that the scar is not quiet yet. Pain, spreading redness, repeated crusting, tenderness, thickening, or a scar that is still rising should delay the decision. A settled scar gives the grafts a fairer environment.
Photographs help, but they do not replace touch and close examination. A scar can look acceptable in a picture and still feel tight, thick, or poorly mobile under the fingers. That physical quality changes graft angle, density, spacing, and whether surgery is reasonable at all.

Which scars are usually better candidates?
The best candidates are usually flat, pale, mature, soft scars with stable surrounding hair. A small childhood injury scar, a narrow surgical scar, or a stable hairline lowering scar may be more suitable than a thick raised scar or a large burn scar with tight skin.
I check the hair around the scar. If the surrounding hair is strong and the scar is small, a modest number of grafts can sometimes create a good blending effect. If the surrounding hair is weak, diffuse, or miniaturizing, the scar may still show because the whole region lacks coverage.
Scar location matters as well. A hairline scar needs very fine direction control because the front edge is visible in normal conversation. A crown or mid scalp scar may be more forgiving from the front, but it can still show if the surrounding hair is thin or if the patient keeps the hair very short.
This overlaps with general candidacy. A person may be a good candidate for camouflaging one small scar but not a good candidate for a large density operation. Scar cases need the same careful lens used when deciding whether someone is really a good candidate for a hair transplant.
When is grafting into a scar a poor idea?
Grafting into a scar is a poor idea when the scar is active, raised, unstable, infected, very tight, or medically unexplained. It is also a poor idea when the patient expects normal density in one session. Scar tissue can improve, but it does not behave like untouched scalp.
A history of thick scars or keloids changes the decision. In that case, I would not treat the scar as only a cosmetic gap. I would first think about skin behavior, because new surgical trauma may create new scar problems. Patients with this history should read more about hair transplant and keloid scar risk before assuming FUE is safe for their skin.
Active inflammatory scarring diseases are a different situation again. A physical scar from an old injury is not the same as lichen planopilaris, discoid lupus, or another process that is still destroying follicles. If the diagnosis is uncertain, the safer route is to clarify it before planning surgery, especially in cases that resemble scarring alopecia or lichen planopilaris.
If there is ongoing itching, scaling, burning, redness, pustules, spreading hair loss, or a patch that looks like a scar that has not been diagnosed, I would not treat it as a simple camouflage case. Dermatology review, and sometimes biopsy, may be more important than choosing a graft number.
Use the 8 scar tissue transplant slides below to separate scar maturity, blood supply, diagnosis, density limits, conservative test sessions, SMP or scar revision options, donor cost, and promises that should make you pause. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.