


Dissecting Cellulitis Needs Stable Scalp Control Before Grafts
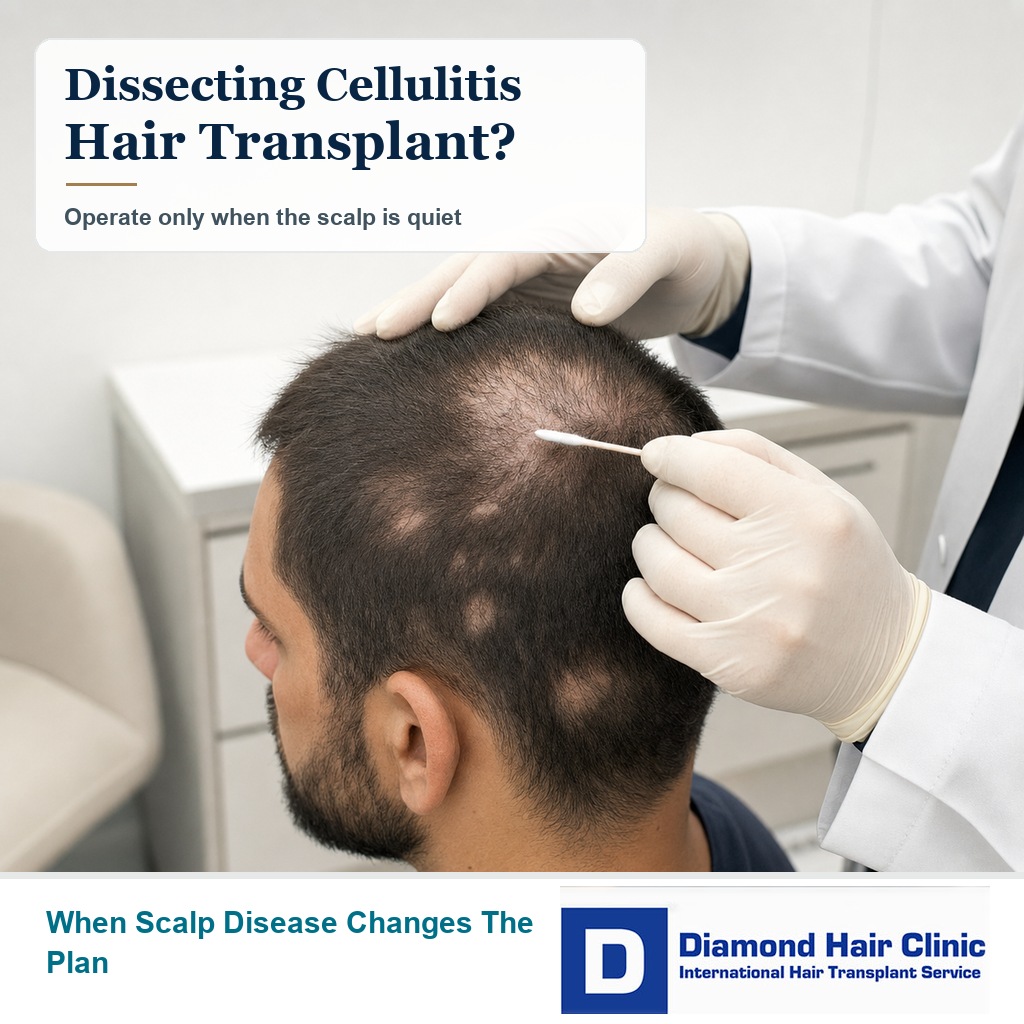
A hair transplant after dissecting cellulitis of the scalp may be possible, but only after the disease has been quiet long enough to trust the skin. If you still have painful lumps, drainage, pus, wet crusting, swelling, or new areas of hair loss, surgery should wait.
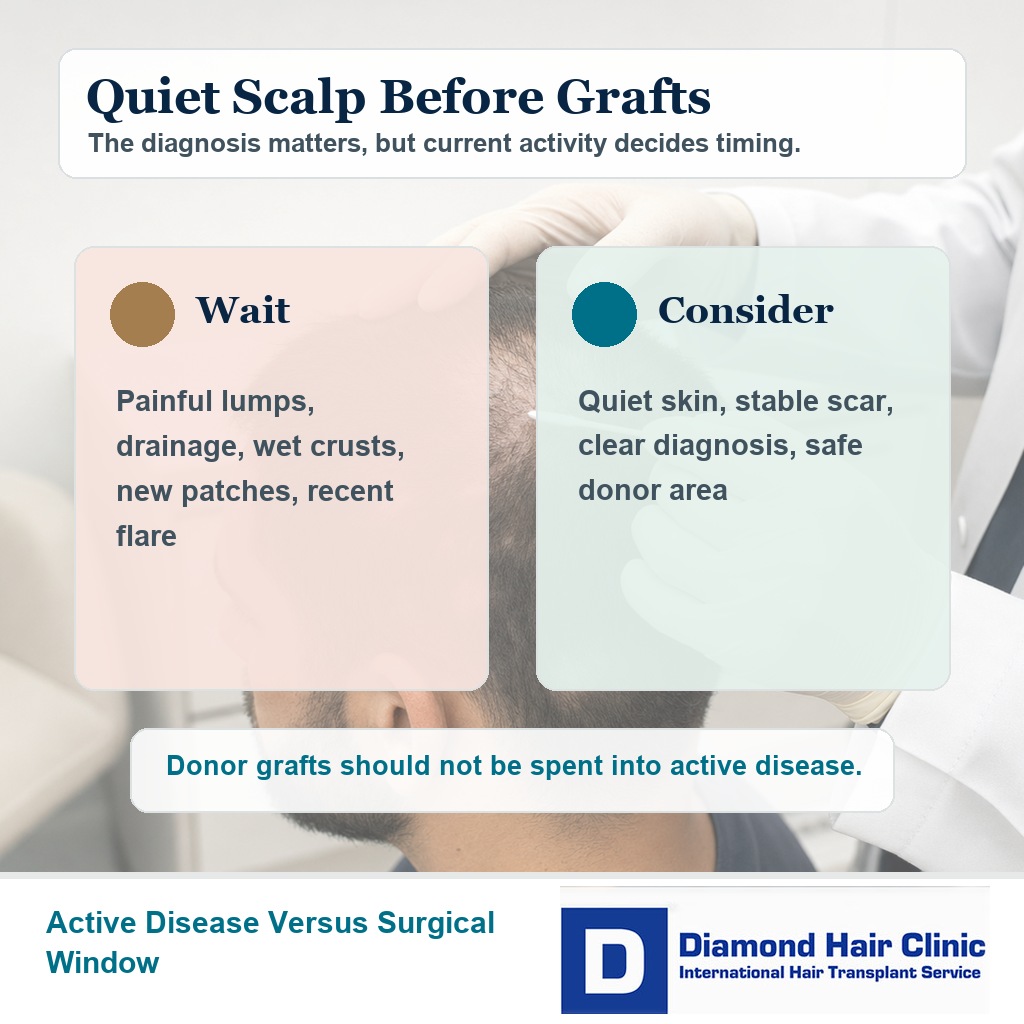
The graft number comes after medical stability. The scalp has to be stable enough for surgery. A transplant can move healthy follicles into a stable scarred area, but it cannot control active dissecting cellulitis. If that distinction is not clear before surgery, donor hair can be spent into a scalp that is still changing.
Dissecting cellulitis changes transplant planning
Dissecting cellulitis changes the plan because the scalp may not behave like normal recipient area skin. This condition can create deep inflammation around follicles, abscess like swelling, draining tunnels, scarring, and permanent patches of alopecia.
In ordinary pattern hair loss, I mainly judge donor capacity, hairline design, hair caliber, recipient area size, and future hair loss. With dissecting cellulitis, I also need to know whether inflammation is still active under the skin.
That difference matters. If the disease is active, new grafts are being placed into an unstable field. The operation may be technically possible, but it can still be a poor use of donor hair.
This overlaps with the broader discussion of hair transplant surgery with scarring alopecia, but dissecting cellulitis deserves separate caution because the inflammation can be deeper, recurrent, and more destructive than an ordinary scar.
Some bald patches may recover without grafts
Before planning grafts, I need to decide whether the follicles are truly destroyed. Some thinning around inflammation is temporary. Some hairs are broken or weakened while the skin is inflamed. Other areas become smooth scar tissue where the follicles have been permanently lost.
One close photo is not enough. I look at follicular openings, skin texture, tenderness, scale, drainage history, older photos, treatment response, and whether the area has changed over time.
A bald patch that has been quiet and unchanged for a long period is a different surgical question from a patch that was swollen or draining last month. If the scalp is still changing, surgery is premature.
This is also why I separate dissecting cellulitis from folliculitis before a hair transplant. Small surface pustules and deep tract forming inflammation are not the same problem. A separate pattern such as folliculitis decalvans before hair transplant also needs its own timing judgment because it can scar the scalp while looking like pustules and crusting from the outside.
A medical recovery window should not be skipped. If short hairs are returning, if follicular openings remain, or if the area improved after treatment, surgery may be the wrong next step.
Surgery should wait during active inflammation
Surgery should wait when there are active painful nodules, pus, draining tunnels, wet crusts, heat, spreading redness, swelling, or new hair loss patches. I also delay if antibiotics, isotretinoin, steroid injections, or another treatment were recently started, stopped, or changed and the scalp has not yet shown stable behavior.
I understand why a visible scarred patch creates pressure. It can affect haircuts, photographs, and confidence. But the donor area is limited, and grafts should not be placed into skin that is still inflamed.
Waiting is not passive. It protects the final result. If the disease flares again after surgery, the new hair may be blamed when the real problem is ongoing scalp disease.
If the issue is pus, odor, fever, increasing pain, or worsening redness after a recent operation, the more urgent page is infection after a hair transplant. The surgical question is whether transplant surgery is responsible after dissecting cellulitis, not home diagnosis of an active infection.
Transplant consideration starts after disease control
A transplant can be considered when the diagnosis is clear, the disease has stayed quiet, the skin is not tender or draining, and the bald area behaves like a stable scar. The donor area must also be strong enough and separate from the disease process.
Scarred skin may not accept density in the same way as healthy scalp. Blood supply, skin thickness, old tunnels, and previous inflammation can all reduce the margin for error.
In some cases, surgery is only a limited cosmetic improvement, not full restoration. A small stable scarred patch may be reasonable to soften. Widespread unstable disease across the crown or donor region is a very different situation.
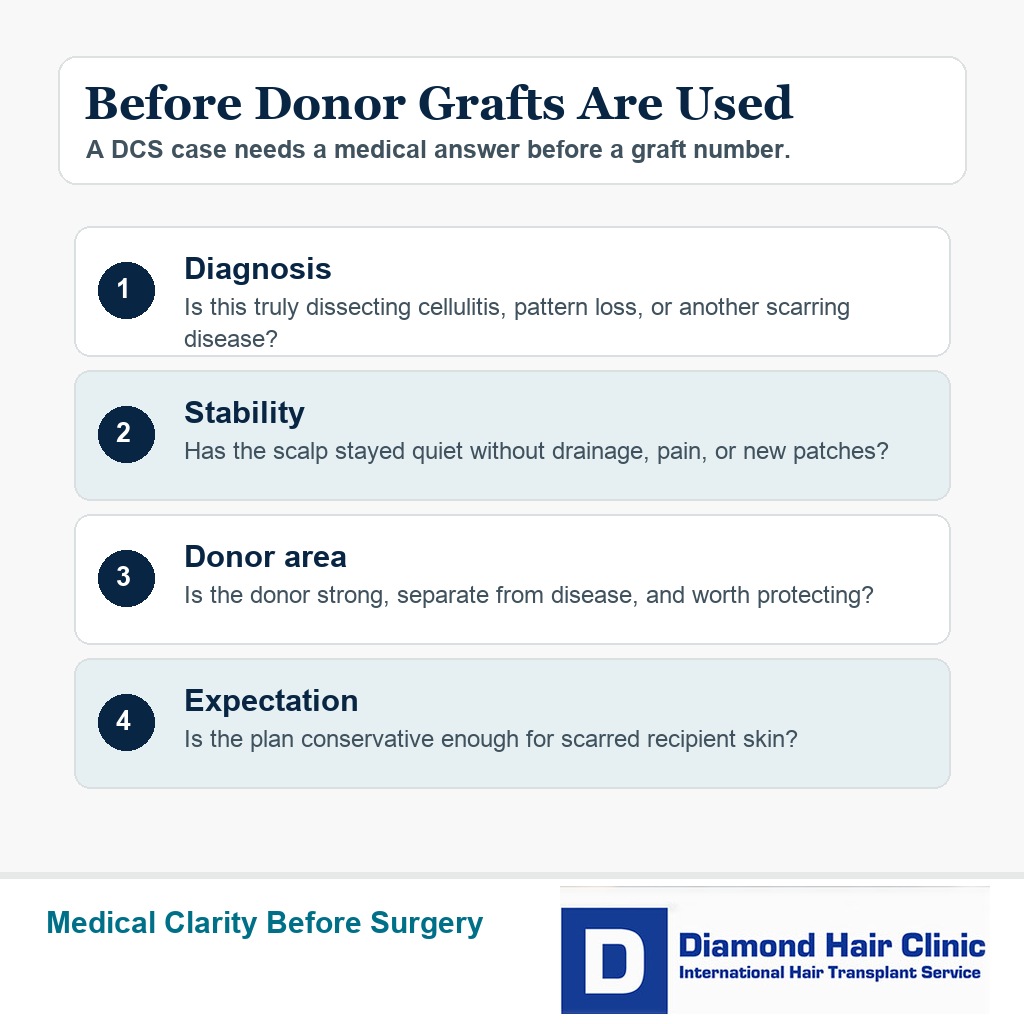
Here, being a good candidate for a hair transplant means more than having enough empty scalp. Disease control, donor strength, recipient skin quality, and expectation all need to fit together.
A quiet scalp period is needed before surgery
People often want an exact waiting period. I cannot give the same number to every case, but I do not consider the scalp ready just because antibiotics dried the area for a few weeks.
For dissecting cellulitis, I generally want at least 12 months of quiet behavior before cosmetic grafting is discussed. In more destructive, recurrent, or heavily scarred cases, 1 to 2 years of stability may be more responsible.
Quiet means more than a dry looking photo. I mean no painful nodules, no drainage, no sinus tracts, no pus, no wet crusting, no expanding patches, no recent rescue treatment, and no uncertainty from the dermatologist that the disease is still active.
If the disease returns every time medicine stops, the transplant discussion is too early. The surgeon should be able to explain why the chosen area is a stable scar rather than active dissecting cellulitis. That is the difference between careful reconstruction and spending donor hair into a moving disease.
Preoperative checks come before using donor grafts
Before donor grafts are used, the medical picture has to be clear. A dermatologist’s diagnosis matters, and in unclear cases trichoscopy or a scalp biopsy before a hair transplant may be needed before surgery is even discussed.
Treatment history also matters. Antibiotics, isotretinoin, steroid injections, biologic medication, medicated shampoo, previous drainage, and flare timing can all change the safe timing of surgery.
The donor area needs careful examination. If the donor area has scarring, repeated inflammation, low density, or miniaturization, the operation may become much more limited. A large graft quote with those findings is a warning sign.
If the donor region itself has painful nodules, drainage, or unstable patches, I do not treat that as a simple density problem. The source of grafts may not be safe enough yet, even if the bald scar in the recipient area looks ready.
Medical screening may also be needed because some people with dissecting cellulitis have other inflammatory or follicular occlusion conditions. Blood tests before a hair transplant can clarify general readiness before the cosmetic plan becomes the focus.
For dissecting cellulitis, these 4 slides keep the decision tied to diagnosis, flare control, donor safety, and when grafting should wait. Swipe sideways, use the arrows, or choose a number below the image.

FUE can be limited in scarred scalp
FUE can sometimes place grafts into scarred scalp, but scarred scalp is less forgiving than normal skin. The grafts still need blood supply, correct depth, careful spacing, and a recipient area that is not inflamed.
A scar from old trauma, a surgical scar, and a scar created by dissecting cellulitis do not behave exactly the same. A dissecting cellulitis scar may sit in skin that previously had deep inflammation, abscesses, tunnels, and repeated tissue damage.
The general principles of hair transplant into scar tissue still apply. The added issue is disease control. Treating a mature scar is one thing. Transplanting into a scalp that may flare again is another.
If FUE is used, I plan the work in a measured way instead of packing grafts aggressively into questionable tissue. A staged approach may be safer when skin quality is uncertain.
Full density is not always realistic
The graft number depends on the size of the stable scarred area, the strength of the donor area, the blood supply of the recipient skin, and the amount of coverage you expect. A serious plan should not come from a few phone photos.
Scarred skin often needs more careful density planning. Trying to force normal density coverage into scarred or previously inflamed tissue can weaken graft survival and create a harsher repair later.
Donor hair is a lifetime reserve. If you have already lost hair from inflammation, those grafts may also be needed for future repair, crown thinning, or pattern hair loss later.
If the bald patch is large, partial improvement may be more realistic than dense full coverage. In scarred or medically complex skin, a modest plan that heals well is better than an ambitious plan that fails.
Medication can change surgical timing
Medication changes can tell us whether the disease is truly controlled. If the scalp flares again after antibiotics stop, that is not a stable surgical window. If isotretinoin or another treatment has just started, I need to see how the scalp behaves before planning grafts.
Do not stop dermatology medication by yourself to look eligible for a transplant. The priority is disease control. Cosmetic surgery should fit around medical stability, not compete with it.
Medication planning also matters around the operation itself. Antibiotic use, stomach tolerance, allergy history, retinoid timing, inflammation treatment, and other prescriptions need review before surgery. For antibiotics after a hair transplant, medication decisions should be individualized rather than copied from another case.
If another doctor is managing the skin disease, the hair transplant plan should respect that treatment plan. Poor communication between doctors can create unnecessary risk.
Risky clinic promises deserve caution
A clinic promise should make you pause when the disease history is ignored. If nobody asks about drainage, abscesses, active bumps, biopsy, dermatology treatment, medication, remission length, donor quality, or scar stability, the quote is incomplete.
Be especially careful when the answer is only a high graft number. In dissecting cellulitis, the graft quote should come after the scalp has been judged, not before. A number offered before diagnosis and stability are reviewed is not a medical plan.
I become concerned when a clinic treats the scar as ordinary empty skin. One photo may look quiet, but old tunnels, fragile skin, and recurrence risk can change the plan.
If you already had a poor operation or a rushed plan elsewhere, bad hair transplant repair becomes a harder discussion. Repair after a rushed decision is usually harder than making the first surgical decision slowly.
Future flares need planning before surgery
A future flare must be part of the consent discussion. Even if the scalp is quiet before surgery, dissecting cellulitis can recur in some people.

You need to know what to do if painful bumps, drainage, heat, swelling, or new tenderness appears after surgery. Early dermatology review is safer than squeezing lesions, applying random products, or waiting until more scarring appears.
Aftercare also needs more attention with this history. Clean washing, avoiding scratching, avoiding dirty hats or pressure, and direct follow up matter. The broader hair transplant aftercare guide is useful, but previous dissecting cellulitis can require more individualized follow up than a routine case.
I also document the scalp before surgery with clear photos. Later, if a symptom appears, comparison is easier. That comparison helps separate ordinary healing, folliculitis, and recurrence of the original disease.
Vague reassurance is not enough when the history includes deep inflammation and scarring. The follow up plan should include a contact route, useful photo instructions, and clear timing for local medical review if symptoms become painful, draining, or progressive.
The safer next step is medical review before graft use
If you have active dissecting cellulitis, the next step is medical control, not a transplant date. See a dermatologist, treat the inflammation, document the diagnosis, and wait until the scalp proves that it is quiet.
If the disease has been quiet and you are left with stable bald scarred patches, then a hair transplant consultation can be reasonable. The consultation should include donor assessment, recipient skin assessment, density limits, flare history, and a realistic explanation of what surgery can and cannot improve.
Do not let embarrassment or frustration push you into a fast package. Dissecting cellulitis can leave visible scars, but donor grafts are valuable. They should be used only when the scalp gives them a fair chance.
My approach is careful and staged when needed. First control the disease. Then confirm stability. Then decide whether the scarred area, donor area, and expectation make surgery responsible.
When the answer is yes, the plan should be measured enough to heal and natural enough to look like hair, not a repair attempt that creates a new problem.