Dutasteride or Finasteride After Transplant?
Dutasteride is stronger, but that does not make it the better choice after a hair transplant. I usually discuss finasteride first because it has a longer, clearer place in male pattern hair loss. I consider dutasteride when the native hair risk is stronger, such as aggressive crown loss, diffuse miniaturization, strong family pattern, or weak response to finasteride. The transplant itself should not be made dependent on either medicine.
Finasteride and dutasteride mainly protect vulnerable native hair, not transplanted grafts. A properly handled graft from the safe donor area should not need these medicines to survive. The hair I watch most closely is the hair that was already miniaturizing before surgery. If that hair keeps thinning, the grafts can grow well but the overall result may still look weaker over time.
I start with the reason for the medication. Are we trying to slow crown loss, protect hair behind the hairline, reduce future graft demand, or manage a plan after finasteride was stopped? Those are different problems, so they do not always lead to the same medicine. I explain the broader timing question separately in my article about finasteride before or after a hair transplant.
Start With Stability, Not Strength
If finasteride is tolerated and the hair loss pattern is not unusually aggressive, I do not rush to replace it. Stability has value during the first year after surgery. If fatherhood timing, semen analysis, or partner pregnancy is part of the history, I review finasteride, dutasteride, fertility, and hair transplant planning before treating dutasteride as a simple upgrade. Blood donation center deferral rules create a different timing issue, so I separate that in finasteride, dutasteride, and blood donation before FUE.
If loss is aggressive, the crown is still thinning, the family pattern is strong, or finasteride has not stabilized the situation, dutasteride can enter the medical discussion. It blocks both type I and type II 5 alpha reductase, while finasteride mainly blocks type II. That broader action can lower DHT more deeply, which is why some doctors consider it in selected cases.
Finasteride has clearer formal use for male pattern hair loss in many places. Dutasteride is often a hair loss decision outside its prostate label. That does not make dutasteride wrong, but it means consent, monitoring, side effect planning, and fertility timing should be handled more deliberately.
Changing medication immediately after surgery needs a clear reason. The early transplant months already include shedding, redness, anxiety, and changing hair texture. If several treatments start or change at the same time, it becomes harder to know what caused a shed, irritation, sexual side effect, mood change, or improvement.
My answer is practical. Finasteride is often the first step. Dutasteride may be worth discussing for selected men. The surgical plan should still be safe if the medication plan changes later.
Grafts Versus Native Hair
The transplanted hairs are usually taken from the donor area, where follicles are more resistant to DHT. That donor resistance is the reason transplanted hair can keep growing in the recipient area. Finasteride and dutasteride do not turn a poor extraction, poor graft handling, or poor recipient area plan into a good operation.
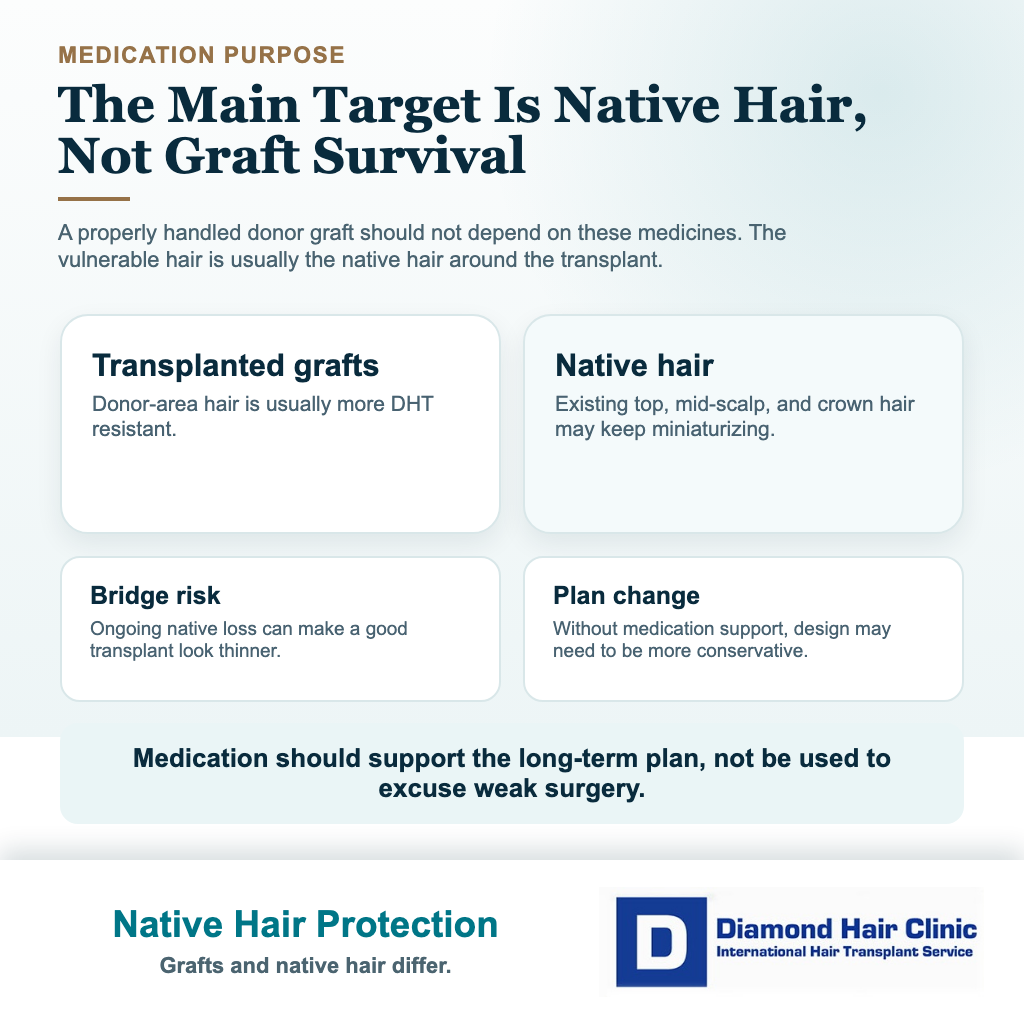
The native hair is different. Hair that remains on the top, mid scalp, crown, or behind a new hairline may still be sensitive to DHT. If that hair continues to miniaturize, the natural bridge between transplanted and existing hair can weaken. That is when a result may start to look separated or thinner even though the implanted grafts grew.
When I plan a hair transplant without finasteride, the surgical design must respect the lack of medication support. I may need a more mature hairline, a different crown plan, or a smaller first session. Medication should never be used to justify reckless graft use.
Donor management matters here. Medicines may help preserve native hair, but they do not create more donor capacity. Once grafts are removed, that donor budget has been spent.
The Way These Medicines Reduce DHT
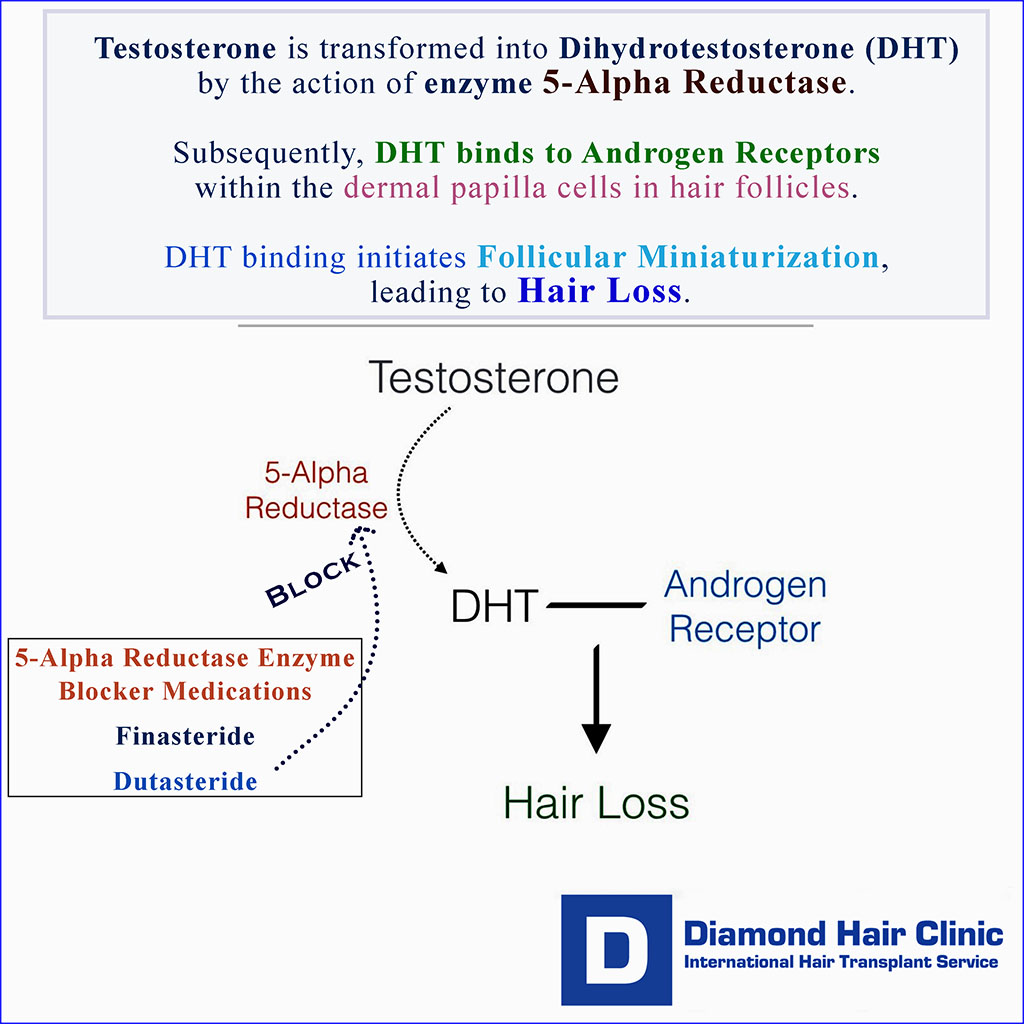
Both medicines reduce dihydrotestosterone, usually shortened to DHT. DHT is made when the body converts testosterone through the 5 alpha reductase enzyme. In men who are genetically sensitive, DHT can gradually shrink hair follicles on the scalp. The hair becomes thinner, shorter, and less useful for coverage.
Finasteride mainly blocks the type II form of the enzyme. Dutasteride blocks type I and type II, so the DHT reduction is usually deeper. That does not mean dutasteride fits every patient. It means the medicine has a stronger biological effect, and stronger biological effects deserve more careful medical supervision.
Dose numbers can be misleading. Seeing finasteride 1 mg and dutasteride 0.5 mg online does not turn those numbers into a personal prescription. Dose, frequency, and follow up must come from the doctor who knows the medical history.

The location of hair loss matters. A patient with a stable frontal recession may need a different plan from a young patient with diffuse thinning across the top. A patient with crown loss also needs special caution because crown demand can grow for many years. Medication may help slow that demand, but surgery still has to be planned with the future in mind.
If the main concern is the hairline, the design must still look age appropriate and natural. A medicine cannot fix an aggressive low hairline that ignores future loss. For hairline design in hair transplant surgery, the shape and height of the hairline must be decided surgically, not emotionally.
Finasteride Often Fits Better in Stable Cases
Finasteride often makes more sense when the patient has never used a DHT reducing medicine, has moderate male pattern hair loss, and wants a more established first step. It may also be reasonable when a patient has already tolerated it well before surgery and the transplant plan depends mainly on preserving native hair behind the new hairline.

I also prefer a stable medication history when possible. If a patient has been taking finasteride without side effects and the hair loss is controlled, changing to dutasteride right after surgery may add uncertainty without enough benefit. Stability is valuable during the first year after a transplant.
Finasteride is not mandatory for every patient. Some patients cannot tolerate it. Some do not want it. Some have limited recession with strong donor hair and little active miniaturization. In those cases, I plan the transplant more carefully and explain the tradeoff. My article on stopping finasteride after a hair transplant helps show what can happen when native hair loses medication support.
Dutasteride Enters the Discussion in Selected Cases
Dutasteride may be discussed when the hair loss is active despite finasteride, when the crown is worsening, when the patient has strong family history, or when the scalp shows diffuse miniaturization that makes future surgery risky. I see it as a stronger medical tool, not as a routine upgrade for everyone.

The timing matters. If the patient is only days or weeks after surgery, I avoid unnecessary medication switches unless the prescribing doctor has a clear reason. Shock loss, early shedding, and the normal waiting period after surgery can already make the patient anxious. Changing treatment too quickly can make the interpretation of recovery more confusing. Early thinning does not always mean failure. Keep that in mind with shock loss after a hair transplant.
Dutasteride may also remain in the body for a long time. That matters when side effects occur, when a patient is planning fertility discussions, or when blood donation rules apply. A patient using dutasteride may be told not to donate blood until six months after the last dose. These details are not cosmetic details. They are medical details.
Copying another person’s dutasteride plan from the internet is unsafe. The same medicine can be reasonable in one man and inappropriate in another.
Stronger DHT Blocking Is Not Always Better
A stronger DHT blocker can protect more hair in the right man, but strength is not the whole decision. A useful switch has a clear reason, such as ongoing miniaturization despite steady finasteride use, crown progression, diffuse loss, or a strong family pattern. A weak reason is panic during shedding, package pressure, or the idea that stronger must always mean safer.
Forum routines can make the decision look like a race toward the strongest stack. I do not use it that way. A higher exposure plan is not safer just because another patient tolerated it, and oral minoxidil adds a separate blood pressure, pulse, swelling, and monitoring discussion. Before changing a DHT blocker or adding oral minoxidil around hair transplant planning, I want the reason for the change, side effect history, fertility timing, prostate screening context, other medicines, and surgical design reviewed together.

Suppressing DHT as much as possible is not the goal. The goal is to protect hair safely enough for that person’s long-term plan. A 24 year old with diffuse loss, a weak donor area, and an aggressive family pattern is not the same as a 45 year old with stable frontal recession.
Hair transplant planning also changes the calculation. If medicine keeps native hair stable, the surgeon may be able to use fewer grafts and preserve donor capacity. If side effects force the medicine to stop, the surgical design must still age reasonably. I never want the result to depend on a medication the person cannot continue.

Side Effects That Need Medical Attention
Both finasteride and dutasteride can cause side effects. The list men usually worry about includes lower libido, erectile difficulty, ejaculation changes, testicular discomfort, breast tenderness or swelling, mood changes, and fertility concerns. These effects do not happen to everyone, but they should not be dismissed when they appear.
If breast swelling, breast pain, nipple discharge, a new breast lump, severe mood change, or suicidal thoughts appear, the medication conversation must become medical immediately. That is not a normal hair transplant recovery issue. Contact the prescribing doctor promptly, or seek urgent help if the symptom is severe.
Mood history deserves direct discussion before starting or changing these medicines. That is not because every man will have a serious mood problem. It is because depression, severe anxiety, thoughts of self harm, and sexual side effects are too important to hide during a hair transplant plan.
These medicines can also change PSA interpretation in prostate screening. Men who are being monitored for prostate health need to tell their doctor that they use a 5 alpha reductase inhibitor. Hair treatment must not hide information from another part of medical care.
Pregnant women, or women who may become pregnant, should not handle crushed or broken finasteride tablets or leaking dutasteride capsules. This matters for household safety because exposure can create risk for a male fetus. It is a small practical detail, but it should be understood before these medicines are treated casually.
Previous Hormone Sensitivity or Gynecomastia
If a man previously had gynecomastia, breast tenderness, hormone sensitivity, sexual side effects, or a complicated reaction, restarting or switching medication alone is not wise. The hair transplant plan has to be built around his medical history, not around a generic medication rule.
Some patients can still have surgery without finasteride or dutasteride. Some may need a topical option, a lower exposure plan, observation, or a different timing. Some should speak with a dermatologist, urologist, endocrinologist, or the doctor who handled the earlier hormone issue before making a new decision.
My detailed finasteride after gynecomastia or hormone sensitivity covers this situation separately. Dutasteride is not a clever way to avoid a serious finasteride history. It is still a DHT reducing medicine, and the medical history still matters.
Topical Options, Minoxidil, and PRP
Topical finasteride can be useful for some patients, but topical does not mean risk free. Some absorption into the body can still occur, and formulas differ. I do not apply it onto fresh grafts in the first days after surgery. The scalp must heal first. I discuss this timing in the article about topical finasteride before or after a hair transplant.
Minoxidil works differently. It does not block DHT. It may help some hairs stay in a better growth phase, and it can be useful when native hair needs support, but it is not a substitute for DHT control in every androgenetic pattern. When native hair support is the question, minoxidil after a hair transplant has to be timed around scalp healing and tolerance.
PRP may help selected patients with scalp quality or hair thickness, but it does not replace the biological role of finasteride or dutasteride in DHT sensitive hair. It should be presented as supportive treatment, not as a guarantee that future hair loss will stop.
Oral minoxidil is another medical discussion, especially when topical use is difficult. It has its own blood pressure, heart rate, swelling, and monitoring issues, so it should not be added casually. My oral minoxidil and hair transplant planning covers that decision more directly.
Starting or Changing Medication Around Surgery
If someone is already stable on finasteride before surgery, many surgeons prefer not to disturb a working routine. If he has never used medication, the discussion belongs before the operation rather than after grafts have been placed.
Starting medication before surgery can sometimes help reveal whether native hair is stabilizing. It can also change the surgical plan. If the crown improves or the mid scalp thickens, fewer grafts may be needed. If nothing improves, the consultation becomes more realistic. I cover this wider decision in the article about whether it is better to try medication before a hair transplant.
After surgery, medication timing must respect healing. Tablets do not touch the grafts, but topical products, sprays, foams, and irritating solutions can affect the recipient area if used too early. Follow the post operation instructions from the surgical team rather than mixing online routines.
The full product list matters before surgery. If a patient is using online topical blends, compounded sprays, or research chemical style products, I review online topicals before FUE planning before connecting the medication routine to the surgical plan.
If shedding has already started, changing several treatments at once is usually unhelpful. It may be better to document photos, wait for the proper timeline, and adjust one variable at a time. Hair transplant recovery is slow enough without adding avoidable confusion.
These 8 DHT blocker decision slides separate transplanted grafts, native hair risk, finasteride history, dutasteride discussion, side effect signals, hormone sensitivity, timing around surgery, and review with the prescribing doctor. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.