Keloid Scars and Hair Transplant Risk
If you have a real history of keloid scars, a hair transplant is not necessarily impossible, but it cannot be answered with a quick yes. Surgery should only be considered after your scar history, skin behavior, donor area, diagnosis, and medical risk are reviewed carefully. In some patients I may operate with a smaller and more conservative plan. In others, I advise waiting, getting dermatology input, or avoiding surgery completely. A scalp mole before hair transplant planning can also change scar and timing decisions if it was recently removed or raised.
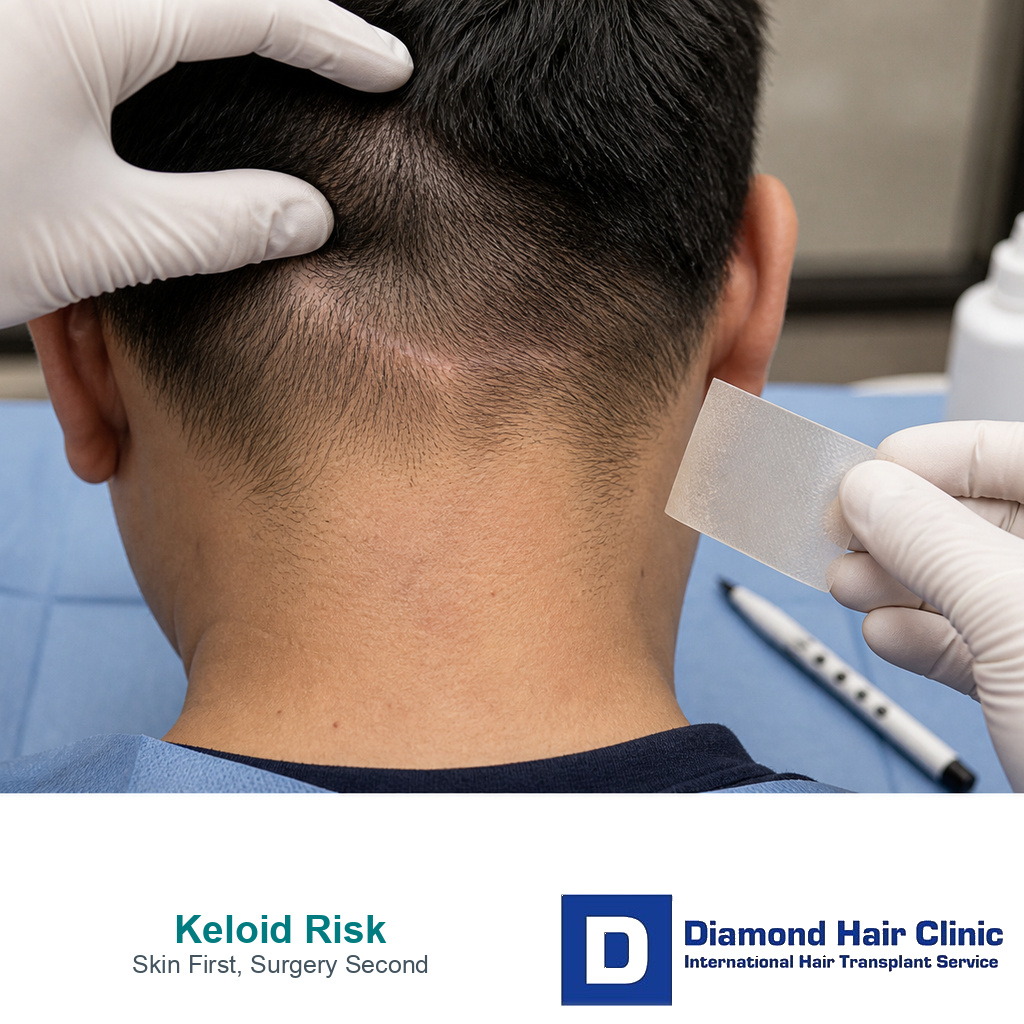
The mistake comes from treating keloid history like a small detail. It is not. A hair transplant creates thousands of tiny injuries in the donor and recipient area. Most patients heal from those tiny injuries quietly, but a patient prone to keloids may react differently. I look beyond whether hair can be moved. The skin also has to heal safely after we move it. This is different from vitiligo hair transplant planning, where pigment changes after injury matter more than raised scar growth. If the concern is a flat color change in the recipient area, I handle dark scalp color after FUE as a separate recovery question.
With keloid scars, I slow the decision down before graft numbers. I assess where the scars formed, why they formed, how they behaved, how long they stayed active, and whether there is a family tendency. A clinic that jumps straight to graft numbers before asking these questions is not giving the problem the respect it deserves.
It helps to know the emotional side of this decision. Having a keloid history does not mean you are being rejected as a patient. It means your case needs a different level of judgment. My role is not to make the surgery sound easy. My role is to decide whether surgery can be done without creating a problem that may bother you more than the hair loss itself.
Keloid history changes the surgical decision
A keloid is not just a thicker scar. It is a healing response where scar tissue can grow beyond the original injury. That matters in hair transplantation because the procedure depends on predictable skin healing. If healing is unpredictable, even a technically clean operation can become a poor decision.
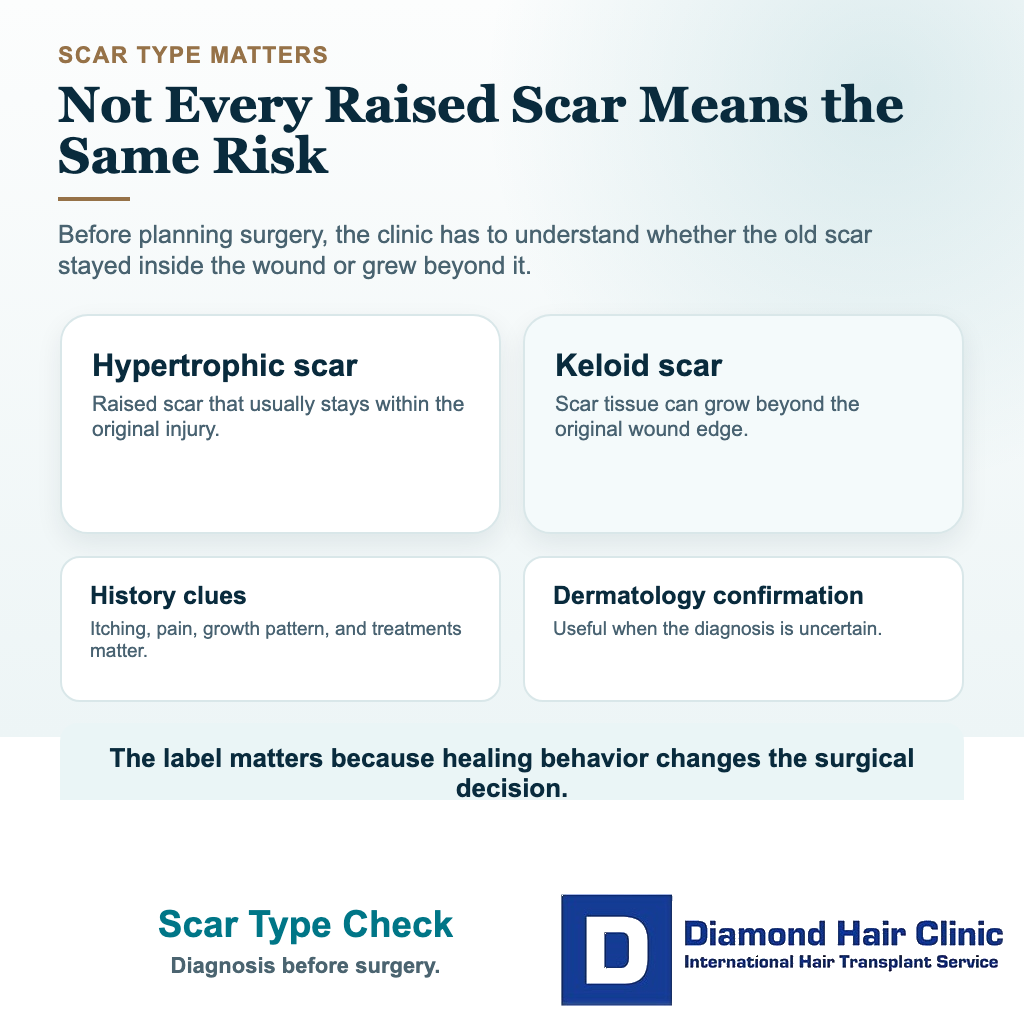
I first try to understand whether the patient truly has keloids or whether the past scars were hypertrophic scars. A hypertrophic scar is raised but usually stays within the original wound. A keloid can grow beyond it. Patients often use the same word for both, but the surgical meaning is different. If the diagnosis is unclear, dermatology confirmation is safer before we plan surgery.
A photograph can show the size and shape of an old scar, but it cannot show the full behavior of the skin. I still need to know when the scar appeared, whether it kept growing, whether it became itchy or painful, and what treatment was needed.
The location of the previous scar also matters. A small earlobe keloid after piercing does not carry the same meaning as multiple thick scars on the chest, shoulders, back, or jawline. A patient with one old piercing scar and normal healing after other injuries may be a different candidate from a patient who forms raised scars after acne, small cuts, or previous surgery. This is especially relevant for facial hair requests, where beard transplant regret can involve raised texture, visible borders, and difficult removal.
When I plan surgery, I am asking one practical question. Is this patient likely to heal the donor and recipient area in a controlled way? When this remains uncertain, the plan must become smaller, slower, or sometimes postponed. A large session at that point creates more skin injury and leaves less room to correct a problem later.
I also separate cosmetic desire from medical behavior. A patient may be a strong cosmetic candidate because the hairline needs improvement and the donor hair looks good, but still be a weak surgical candidate because the skin has shown abnormal scarring. Hair transplantation is not only hair design. It is controlled injury and controlled healing.
A keloid on the chest or shoulder does not tell me exactly how the scalp will heal
Not always, but it must be taken seriously. Keloids are more common on some body areas, such as the chest, shoulders, ears, jawline, and upper back. The scalp may not behave exactly the same way, but that is not a reason to ignore the history.
A patient with one old earlobe keloid and normal healing after other injuries is different from a patient who forms thick scars after acne, injections, small cuts, or previous surgery. I need a clear picture of the pattern, not only the label. Where the keloids formed, how easily they appeared, whether they kept growing, and whether they needed treatment all change the decision.
Skin tone, curl pattern, and family history can also influence the discussion, especially when I am planning Afro textured or very curly hair transplantation, but they do not decide the case alone. Background alone should not reject a patient, and one quiet scalp photograph should not approve surgery. I judge the individual scar history and the planned surgical stress together.
FUE may reduce one scar concern, but it does not remove risk
In many patients prone to keloids, I am much more cautious with any procedure that creates a long incision. The discussion often turns toward FUE hair transplant because FUE avoids the long linear incision used in FUT hair transplant, so it may reduce one type of scar concern.
But FUE is not magic. It still creates many tiny extraction wounds in the donor area and many small openings in the recipient area. A patient who forms keloids from very small injuries cannot be told that FUE removes the risk. It may make the risk more acceptable in carefully chosen patients, but it does not remove the risk. In patients whose raised scars involve the nape, acne keloidalis nuchae can also change FUE donor planning.
Changing the label to DHI hair transplant does not remove this biology. The grafts still have to be extracted, the recipient area still has to be opened, and the skin still has to heal.
Weak clinic advice can become dangerous here. Some clinics say FUE leaves no scar. I am deliberate about that phrase. FUE usually leaves tiny dot scars that are hidden well when the donor area heals properly and hair length is appropriate. In a patient prone to keloids, I look at whether those tiny wounds may heal in an exaggerated way.
Keloid scarring after FUE is rare, but rare is not the same as impossible. That difference matters because a rare complication can still be serious for the patient who already knows their skin may overreact to injury.
If a patient has a strong keloid history, I think carefully about graft count. A very large FUE session means more extractions and more recipient area openings. The patient may be attracted by a high number, but my responsibility is to ask whether the skin and donor area can tolerate that plan. Sometimes the better plan is smaller, staged, or no surgery at all.
FUT can still have a place in hair restoration generally, especially in some repair or donor preservation discussions, but a patient with keloid risk changes that calculation. A long donor incision may be a poor match for someone who forms raised scars after surgical wounds. If the issue is an old line rather than active keloid behavior, I assess FUT scar repair with FUE grafts separately. Even when FUE is chosen, I do not describe it as free of scarring. I describe it as a different scar pattern with a different risk profile.
Waiting can be safer than operating
I advise waiting if the patient has active, growing, painful, itchy, or recently treated keloids. Active scar behavior tells me that the skin is still reactive. Operating while that pattern is active can turn a cosmetic procedure into a healing problem.
I also wait if the patient cannot clearly describe the scar history. If someone only says they think they get keloids, but the diagnosis was never confirmed, I do not rush. I need photographs, medical history, dermatology notes if available, and a careful look at the scalp. Good surgical planning begins before the operating day.
Another reason to wait is an uncertain hair loss diagnosis. If the patient has scarring alopecia, active inflammation, alopecia areata, or diffuse thinning that is still changing, the scar concern is only one part of the risk. The first decision is whether the hair loss itself is stable enough for surgery. I always connect keloid risk with the question of whether someone is a good candidate for hair transplant.
I also delay if the patient wants surgery mainly because of pressure, embarrassment, or a discount that expires soon. Keloid risk is exactly the kind of issue that becomes dangerous when decisions are rushed. The patient needs time to collect medical details, think clearly, and hear a plan that is not built around urgency.
Waiting is not a failure. It can be the most surgical decision I make. It protects the patient from a rushed operation, and it protects the donor area from being used before we know whether the skin will heal safely. Delay can feel frustrating, but disappointment in consultation is better than a scar problem that cannot be fully reversed.
A small test session can make the decision safer
In carefully chosen patients, a small test session can be discussed. Instead of moving thousands of grafts immediately, the surgeon performs a very limited number of extractions and implantations, then watches how the skin heals over time. This can give more information than theory alone.
But a test session is not a guarantee. If the test area heals well, it is reassuring, but it does not prove that a larger operation will behave the same way. A full session creates more total skin injury, longer operating time, more aftercare demand, and more inflammation. The test can reduce uncertainty, but it cannot remove it.
I consider a test only when the patient understands its limits. The patient must be willing to wait for proper healing before making the decision on a larger procedure. Judging the test after a few days is not enough. Keloid behavior and abnormal scar thickening can take longer to declare themselves, so impatience defeats the purpose of the test.
The test also needs intelligent planning. The donor area should be chosen carefully, the recipient area should not be cosmetically risky, and a reassuring test must not be sold as proof that a large session is safe. A test is a clinical tool, not a marketing shortcut.
A test session should not be used to satisfy curiosity if the concern is already clearly too high. If a patient has repeated aggressive keloids after small injuries, the answer may already be clear enough. A test should be used when the situation is borderline and the result of the test may genuinely change the decision.
A test area needs months of observation
A test area should not be judged after a few days or a few weeks. Early redness, scabs, itching, and small bumps can be part of ordinary healing. Keloid behavior can take longer to show itself, and scars can continue changing for months.

If the concern is mild, I still want enough time to see settled healing before approving a larger operation. If the concern is serious, I may prefer to watch the test area for 6 to 12 months before making a bigger decision. That may feel frustrating, but it is better than discovering the problem after thousands of wounds have already been created.
The test should also include both sides of the decision. The donor extraction points and the small recipient area both need to heal quietly. A quiet donor response alone does not necessarily prove that a full hairline or crown plan will be safe.
Checks needed before surgery is planned
Before surgery, the medical and scar history needs to be detailed. I ask about past surgery, piercings, acne scars, burns, vaccinations, tattoos, family history, and any scar treatments such as steroid injections, silicone sheets, laser sessions, or surgical scar revision. These details help me understand whether the skin reacts only in certain areas or reacts strongly to many types of injury.
I also review general medical readiness. If the patient has diabetes, uncontrolled blood pressure, smoking, immune problems, or medications that affect healing, the risk discussion changes. This helps explain why blood tests before hair transplant surgery are not just a routine formality. They help us catch medical issues that may make healing less predictable.
Medication history matters too. Some patients are using drugs that affect bleeding, inflammation, immunity, or wound healing. Others are taking acne medication or treatments for skin disease. I avoid patients stopping anything on their own, but I do want the medication list reviewed before surgery. A separate discussion about medication before a hair transplant can prevent unsafe assumptions.
The scalp itself must be examined for active dermatitis, folliculitis, psoriasis, scarring, irritation, infection, and poor donor quality. If the scalp is inflamed, controlling that comes first. A quiet scalp is easier to operate on and easier to heal, especially in a patient whose scar response may already be sensitive.
I also have to see whether the patient picks, scratches, or irritates healing skin. This may sound small, but behavior after surgery can influence healing. One accidental touch is different from repeated checking, rubbing, picking, or testing the skin every hour. In a patient prone to keloids, that extra irritation can create confusion and make healing harder to judge. Part of the plan is making sure the patient can follow specific aftercare without panic.

Protecting the donor area in patients prone to keloids
The donor area is not only where grafts come from. It is a lifetime resource. In a patient prone to keloids, I protect it even more carefully because donor damage is difficult to hide and difficult to repair. If the donor heals badly, the patient may lose grafts and gain a visible scar problem.
I plan extraction density more conservatively. I avoid chasing a dramatic graft count if it requires aggressive harvesting. The patient may ask for maximum coverage, but the donor area has a biological limit. I often explain the donor area as a budget that must last for the future, not as a bank that can be emptied in one day.
Overharvesting is already a serious mistake in ordinary patients. In a patient prone to keloids, it can become even more unforgiving. Too many extractions close together can create visible thinning, textural change, and a donor area that looks surgically damaged. Patients who want to understand this risk should study overharvesting in the donor area before agreeing to a large number.
Good donor management also means knowing when to say no to crown ambitions or very low hairline requests. For a patient prone to keloids, it is not wise to spend grafts on a plan that is already cosmetically excessive. I do not aim to use every possible graft. The aim is to create a natural improvement while keeping the scalp and donor reserve as safe as possible.
In these cases I keep in mind hairstyle after surgery. If the patient likes to shave very short, donor texture becomes more visible. Even tiny FUE marks can matter more when the hair is kept extremely short. If abnormal scar thickening occurs, a very short haircut may make it harder to hide. That detail needs review before surgery, not after the patient is disappointed.
Use these 8 slides to check scar history, donor safety, and whether surgery should wait. Swipe sideways, use an arrow, or choose a number below the image.