



Can active AKN delay FUE?
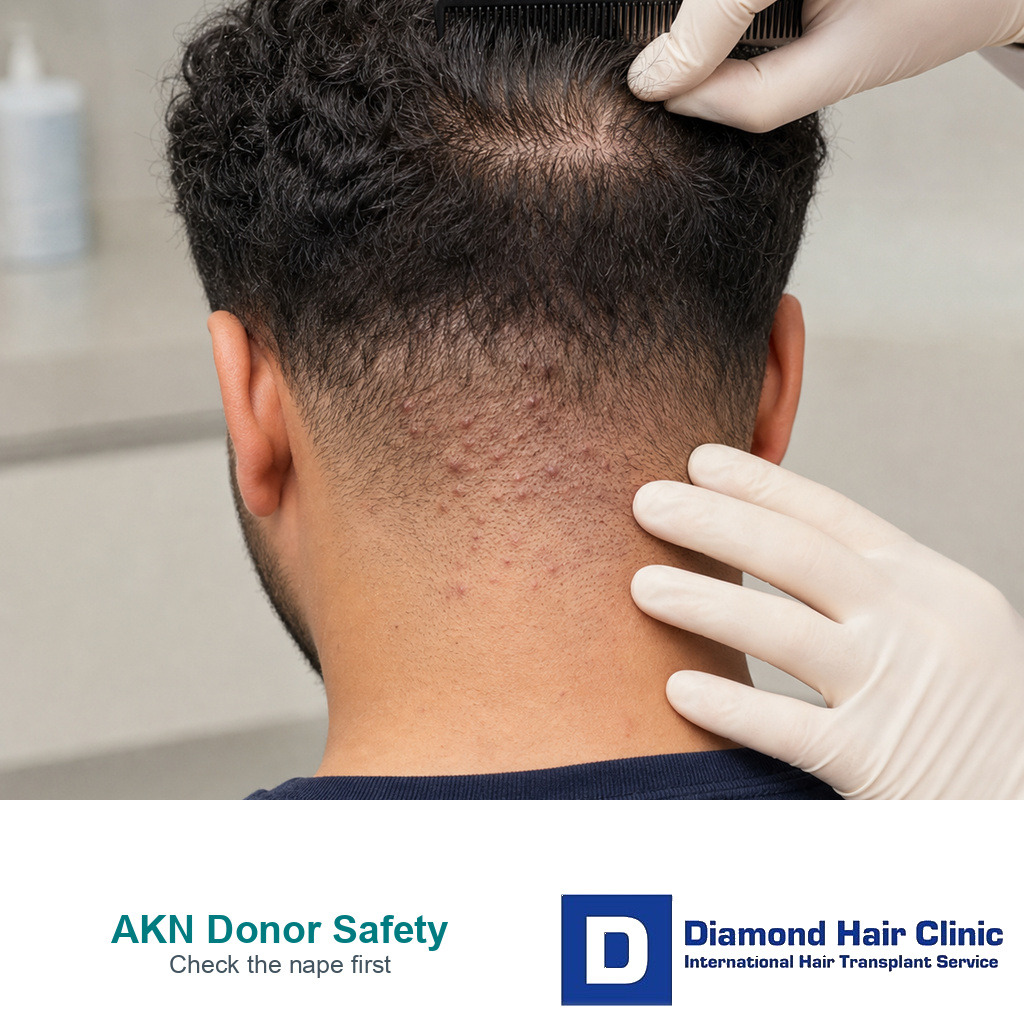
Active AKN tells me the skin is not settled. Tenderness, pustules, crusting, bleeding after scratching, repeated flares after shaving, and firm plaques all matter. These signs may still leave room for surgery later, but they change the timing.
Quiet old scarring and active disease are not the same surgical situation. Old stable marks may sometimes be mapped around. Painful bumps, drainage, spreading plaques, or repeated recent flares need control first because the skin is still declaring itself. The same distinction matters with folliculitis decalvans before FUE, where pustules, crusting, and scarring change the timing before donor planning starts.
FUE adds many small extraction points to the donor area. Even when done well, this is controlled trauma. Healthy donor skin often heals these points as tiny pale dots. Inflamed skin may react differently. It may stay red longer, itch more, become infected, or heal with thicker scar tissue. If the nape already forms raised bumps, that history has to be respected.
The next step is usually to settle the skin first. That can mean stopping close shaving, treating infection or inflammation, reducing friction from collars or helmets, and confirming the diagnosis when the pattern is unclear. This is not a pointless delay. It is how I find out whether the donor area can behave like safe donor skin.
Is the lower nape always safe donor hair?
The entire back of the head is not donor area. The lower nape may look like spare hair in a short fade, but it can sit outside the long-term safe zone. With AKN, that same area may also be the least predictable skin for healing. The safe donor zone is the part of the scalp most likely to keep hair long term. The lower nape can be unstable in two ways. It may contain hair that is not ideal for transplant survival, and in AKN it may contain skin that is already inflamed, thickened, or scarred.
That distinction matters because AKN often sits exactly where an aggressive plan might try to take extra grafts. If the extraction pattern dips too low, the operation can remove hair from a zone that should have been avoided. It can also create tiny wounds in skin that already reacts badly to repeated irritation.
I discuss this in detail when there is a weak donor area or signs of donor miniaturization. AKN does not remove the need for donor mapping. It makes donor mapping more important. The plan must show where the stable donor zone ends, where the nape disease begins, and whether there is enough usable hair between those limits.
How do haircut and friction history change the surgical plan?
The history often tells me more than one photograph. I ask what happens after a close haircut, whether the bumps flare after a razor fade, whether collars rub the nape, and whether the area is scratched at night. If every close shave causes painful bumps, that trigger pattern needs control before surgery. Even donor shaving for FUE should be planned with more caution.
Sometimes the disease is partly hidden by longer hair. Sometimes the consultation happens just after a haircut, when the bumps look angry. The pattern over time matters. Clear photos from different haircut stages help show whether the condition is stable or reactive.
This also affects recovery instructions. A single mild bump after a haircut is different from repeated painful flares after every skin fade. A loose collar is different from a tight helmet or shirt edge rubbing the same scarred nape every day. If the same trigger continues after surgery, a flare may be blamed on the transplant even when the irritation pattern was already present.
AKN planning starts with quiet skin, haircut trigger history, safe zone mapping, and realistic donor reserve.
How is AKN different from ordinary folliculitis?
Ordinary donor area folliculitis and AKN can both show bumps. The difference is how the skin behaves over time. Folliculitis is often temporary inflammation around hair follicles. AKN has a stronger tendency toward firm bumps, thickened scars, repeated irritation, and hair loss in the affected nape area. That difference changes the surgical risk.
If the problem looks like folliculitis before a hair transplant, I still want it treated before surgery. If the pattern suggests AKN, I become more conservative about the lower donor border and the timing of extraction. A few temporary pimples after FUE are not the same as chronic AKN plaques that have already scarred the nape.
When the diagnosis is uncertain, a dermatologist’s opinion or a scalp biopsy before a hair transplant can be more valuable than guessing. I also compare the nape findings with other scarring patterns. Some people with AKN have thick scars elsewhere. Some have another inflammatory scalp disease, such as scarring alopecia before hair transplant planning. The label matters less than whether the skin is stable enough to heal.
There is one more distinction patients sometimes miss. In selected dermatology cases, follicular unit extraction may be discussed as a way to remove follicles inside visible AKN papules. That is different from using scarred or reactive nape skin as a donor supply for cosmetic coverage. Treating a lesion and harvesting a donor area are not the same decision.
A small test session can be safer in selected cases
In selected cases, a small test session can be safer than jumping straight to a full FUE. This is not a shortcut to approval. It is a way to observe how donor skin heals after a limited number of extractions. If there is a strong scar tendency, active AKN history, or serious concern about donor healing, a test can prevent an oversized first step.
The test must be planned properly. It should not be taken from the worst inflamed nape skin just to prove a point. It should be placed where the surgeon can learn something about healing while keeping the person safe. Then the area needs enough time for review. A quick glance after a few days is not enough when the concern is raised scarring or delayed inflammation.
If the test heals poorly, that answer is useful. It may prevent a larger operation that would have been difficult to manage. If the test heals well and the disease remains quiet, the discussion can continue with better information. A test reduces uncertainty, but it does not guarantee that a full operation will behave perfectly.
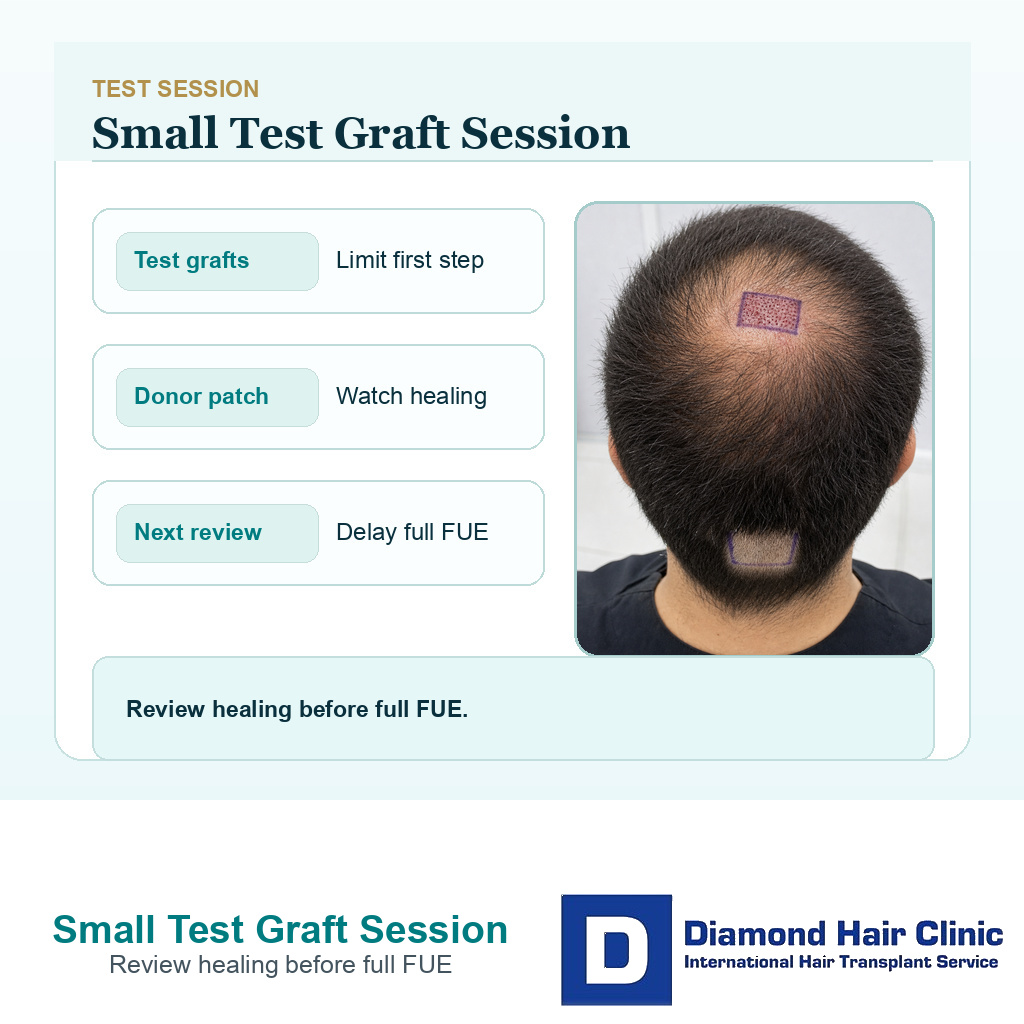
A small test graft session can show how the recipient and donor areas heal before a full FUE plan.
Donor reserve still decides the plan
Even if the AKN is controlled, there still has to be enough safe donor hair. This is where the consultation becomes practical. How many grafts can be taken without entering the inflamed nape zone? How much coverage does the recipient area need? Would a more moderate hairline protect the long term plan better than a low aggressive hairline?
AKN can reduce flexibility. If the lower donor area should be avoided, the available graft reserve may become smaller. In a young man with advanced hair loss, that can change the entire strategy. The answer may be fewer grafts, a higher design, medical stabilization, a staged approach, or no surgery for now.
I also explain that repair is harder than prevention. An overharvested donor area is already difficult to improve. If overharvesting happens in someone whose nape skin scars easily, the repair options become narrower. The first operation should leave the donor area acceptable with short hair, not just chase a large graft number.
Photos and treatment history should be reviewed first
Before I make a surgical recommendation, I need clear photos of the full donor area, the lower nape, both sides above the ears, and the recipient area. The hair should be shown at normal daily length and, if possible, after the type of haircut that triggers symptoms. Blurry photos weaken this decision because nape texture and scar pattern are easy to miss.
I also ask about previous treatment, including antibiotic creams, steroid injections, oral medication, laser hair removal, isotretinoin, surgical excision, and how long each treatment helped. A history of repeated treatment for painful plaques is different from a few quiet bumps after an old haircut.
Photos after past flares help as well. The disease may look quiet on consultation day while older pictures show repeated swelling, drainage, or thickening. That older history belongs in the surgical decision. I am trying to decide whether the scalp is ready for a planned surgical wound pattern, not whether it can look acceptable in one good photo.
Warning signs should pause FUE with AKN
The operation should pause if the nape is painful, hot, draining, crusted, or recently infected. It should also pause if firm plaques are expanding inside the proposed donor area, if the diagnosis is unclear with scarring hair loss, or if the graft plan depends on harvesting low into the nape because the upper donor reserve is weak.
Declining surgery can be the safer medical decision. If unstable skin disease, weak donor reserve, unrealistic coverage expectations, and pressure for too many grafts all meet in the same case, the operation may create more regret than benefit. A careful refusal is not a lack of confidence. It means the scalp is not offering a safe surgical path today.
There are also quieter warning signs. Daily scratching, repeated razor fades despite flares, or changing treatments every few weeks all make the healing environment less predictable. Those habits can often be improved. Once the skin is settled and the history is clearer, the transplant question can be reopened with less risk.
Pain, drainage, spreading plaques, unclear diagnosis, or a low donor plan should pause the operation.
Short hair expectations can change the donor plan
People with AKN often worry about the nape because short haircuts expose it. FUE can also leave tiny donor marks, even in excellent healing. If the lower nape already has bumps, scars, and uneven texture, a very short fade may not hide the combined pattern well.
Short hair after FUE donor scars belongs in the discussion before surgery. The question is not only whether the recipient area can grow. The donor area must also fit the grooming style. If the desired skin fade is exactly what triggers AKN, the haircut plan after surgery needs to be realistic.
Plain discussion before surgery is better than disappointment afterward. A slightly longer donor haircut, a higher extraction border, or a smaller session may be the price of safer healing. If that tradeoff is unacceptable, it is better to know before the donor is touched.
FUE can be reasonable when AKN is quiet
AKN does not mean every person has to be rejected from hair transplant surgery. It means the plan has to be selective. The skin disease should be quiet, the diagnosis should be clear, the safe donor zone should be mapped, and the graft number should respect the usable reserve. The nape should not be treated as spare donor territory.
When the case is suitable, I avoid active nape disease, reduce unnecessary trauma, and give clear follow-up instructions. After surgery, early photos matter because redness, pustules, itching, or thickening need fast review. With an AKN history, waiting months for a donor area flare to declare itself is not sensible.
That follow-up mindset is part of being a good candidate for a hair transplant. The person needs to understand the limits, send clear photos, and keep the scalp routine steady. If symptoms appear, follow-up after hair transplant surgery becomes a safety tool, not an administrative detail.
If you have acne keloidalis nuchae, do not book FUE based only on a graft quote. The decision is not a simple approval question. It is whether the skin is quiet, the lower nape can be avoided, donor reserve still supports a reasonable goal, and your surgeon is willing to say no if the plan would be unsafe. A safer transplant begins before the first graft is removed.