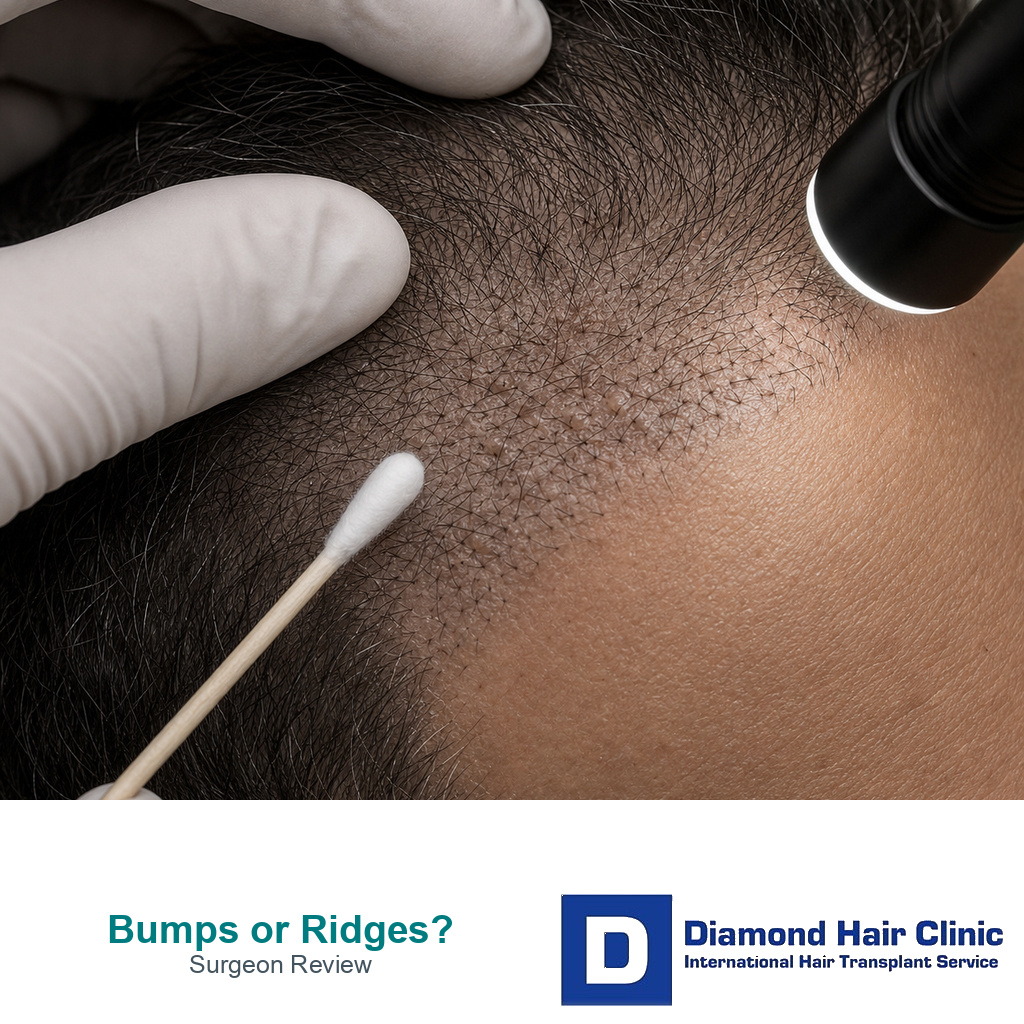
Scalp Bumps and Ridges Need Surgeon Review
Small bumps after a hair transplant can be normal, especially when scabs are loosening, new hairs are trying to grow, or the skin is mildly irritated. But raised rows, firm ridges, spreading painful bumps, pus, heat, or an uneven surface that appears after shedding should not be dismissed without examination. A smooth healing scalp and a raised scar texture are not the same thing. If the surface looks sunken instead of raised, the same careful photo logic applies to a scalp dent after hair transplant. If the surface looks more raised week by week, clear photos and often a direct assessment are needed.
This question makes patients nervous because the scalp becomes the most watched part of the body after surgery. A small change can feel like proof that something has gone wrong, especially when the clinic gives a vague answer or the transplanted hairs have already shed.
Not every bump has the same meaning. Timing, symptoms, pattern, and whether the surface is improving or becoming more organized are the details that separate normal healing from a raised texture that deserves proper medical judgment. When a bump existed before surgery, scalp cyst review before hair transplant is part of the planning record.
Raised scalp texture after a hair transplant
A few small bumps, pimples, or temporary uneven areas can happen during healing, but a firm ridge, a raised surface arranged in a row, or skin that looks thick and folded is not something I call normal from a photo alone. It needs context, timing, symptoms, and a close look at the scalp.
During the first 10 to 14 days, the recipient area is still healing from thousands of small openings. Scabs, dryness, mild swelling, and tiny red points can make the surface look irregular. I do not evaluate final skin quality in the first days.
After the scabs are gone and shedding begins, the surface should gradually look flatter and less irritated. If the skin becomes more raised around week 6, week 8, or later, the question changes. At that stage, the scalp has to be checked for folliculitis, irritation, thick scar response, graft placement depth, dense packing, or another problem.
Some patients send photos and ask whether they are seeing the same issue covered in redness, scabs, and pimples after a hair transplant. Sometimes the answer is yes. Sometimes the texture is more structural than a small pimple, and that changes the advice.
If a bump is small, isolated, and improving, careful observation may be enough. If the scalp surface is forming ridges, rows, or painful swollen areas, do not treat it casually.
Small bumps during normal healing
Small bumps can appear when crusts are lifting, when short hairs are trying to come through the skin, or when the scalp becomes dry and irritated. For some patients, this settles without leaving a permanent surface change. The deciding detail is that the bump should not be growing, spreading, or becoming more painful.
A small bump that looks like a pimple can also appear when a hair is trapped under the skin. This can happen in the recipient area or donor area. It is usually more common during the early growth phase, when new hairs begin to push through and the skin is still reactive.
There is a difference between a small inflamed follicle and a raised sheet of tissue. A pimple has a focal point. A ridge has shape and length. A row of raised skin points beyond ordinary irritation.
The patient’s handling of the area also matters. Scratching, rubbing, picking, harsh washing, or trying to remove every small flake can make the skin more inflamed. The guidance around touching grafts after a hair transplant matters even after the first anxious days.
Mild signs that are improving can often be observed carefully. Pain, heat, discharge, a firm raised surface, or a change that is becoming more visible needs direct review.
Ridges or raised rows that need surgeon review
Ridges or raised rows need a surgeon to examine them when they persist after the early healing stage, when they become clearer after shedding, or when they follow the pattern of the implanted area. I pay special attention when the texture looks organized, because organized texture can sometimes reflect how the recipient area was opened and filled.
The skin should not look as if it has been arranged into ridges by the surgery. A hair transplant should create hair growth, not a new visible skin pattern. If the surface itself is drawing attention, the problem may be cosmetic even before the final hair result is known.
At 6 to 8 weeks, most transplanted hairs have shed or are shedding. The scalp often looks less exciting at this stage, and patients can feel disappointed. But disappointment about density is different from seeing a raised surface. The first may be part of the ugly duckling phase. The second needs closer examination.
The raised area also has to be compared with the original surgical plan. Dense packing, a very large session, aggressive hairline lowering, or a clinic chasing a dramatic result can all affect how the skin responds. The skin has limits, and the plan should respect them.
If the clinic answers every concern with only wait and massage, the scalp needs to be examined more carefully. Waiting is sometimes correct, but it should be based on a diagnosis, not on habit. Massage may help certain healing textures later, but it should not replace proper evaluation of infection, scar response, or technical problems.
Folliculitis compared with ridging
Folliculitis usually looks like small inflamed spots around individual follicles. It may appear as red bumps, tender pimples, or tiny pustules. It can happen when a hair is trapped, when the skin becomes oily, when bacteria irritate the follicle, or when the scalp is reacting during new growth.
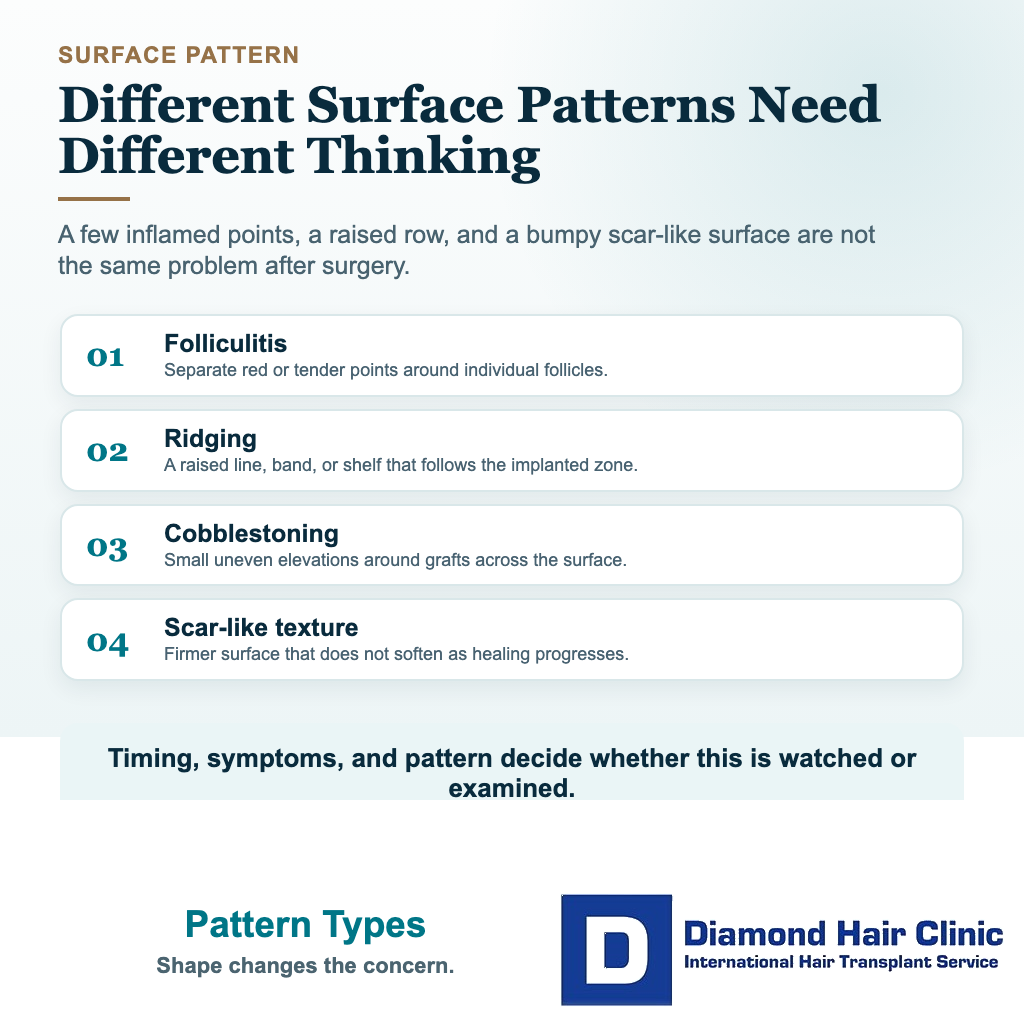
Ridging is different. Ridging is a raised line or band of tissue. Cobblestoning is another type of uneven surface where the skin around grafts looks bumpy, like small elevations and depressions. These are not the same as one or two pimples.
The pattern matters. Folliculitis usually has separate inflamed points. A ridge has direction. Cobblestoning has texture. Scar tissue often feels firmer than ordinary skin irritation. The beard transplant version of this problem is covered in beard transplant cobblestoning in the weeks after surgery, where facial skin and the early timing change the advice.
Symptoms also help. Folliculitis may be tender, itchy, or have a small white head. A ridge may be less inflamed but more fixed. An infection may have spreading redness, warmth, pain, pus, swelling, or fever.
Patients often worry that any bump means grafts are failing. That is not true. Mild folliculitis does not always destroy a result, but more than mild folliculitis needs correct treatment. Even so, a persistent raised surface should not be called folliculitis if it does not behave like folliculitis.
Itching after a hair transplant becomes relevant here. Itching can be normal, but if itching drives scratching and inflammation, the patient can make a small problem worse by trying to fix it with their fingers.
Cobblestoning and ridging are different surface patterns
Cobblestoning and ridging are both surface texture problems, but they do not look exactly the same. Cobblestoning usually looks like many small uneven elevations around grafts. Ridging usually feels more like a raised line, band, or shelf of tissue.
The difference matters because a scattered inflammatory bump, a trapped hair, cobblestoning, and a true ridge do not all need the same response. Separate red points around follicles usually raise the question of folliculitis first. An organized raised surface that follows the transplanted zone raises a different question about graft depth, skin trauma, dense packing, or scar response.
It also matters whether the skin looked smooth immediately after surgery and became raised later, or whether the surface looked uneven from the beginning. Timing gives clues. A temporary inflammatory bump can appear and settle. A structural surface problem tends to be more fixed and more visible when the hair has shed.
You do not have to diagnose these labels alone. The plan needs to describe the pattern clearly so the surgeon can decide whether the issue is normal healing, inflammation, infection, or a technical surface problem.
Dense packing and too many grafts can stress the skin
Overly aggressive density can contribute to skin trauma, poor healing, folliculitis, popping, ridging, or an unnatural surface in some patients. That needs careful wording because not every raised area means the surgeon placed too many grafts. But the risk becomes more realistic when a clinic pushes very high graft numbers into a limited recipient area.
The recipient area is living skin. It has blood supply, elasticity, healing capacity, and limits. It is not an empty field that can accept unlimited grafts simply because the patient wants stronger density.
When too many openings are made too close together, the skin may become stressed. If grafts are placed too shallow, too deep, or under too much tension, the surface can heal unevenly. The patient may later see small elevations, depressions, or a texture that does not look like the original scalp.
This connects directly with too many grafts in one area. Density is not only a number. Density has to respect blood supply, graft survival, natural hair direction, and the skin itself.
Very large sessions need even more caution. A 7,000 graft hair transplant over two days can sound impressive to a patient who wants full coverage, but the decision depends on whether the donor area and recipient area can safely support that plan.
More grafts do not always mean a better result. Sometimes more grafts mean more trauma, more risk, and fewer options if repair is needed later.
Gentle handling matters when bumps appear
You should be careful because massage and picking can help the wrong problem at the wrong time. If the issue is dry skin or mild firmness after proper healing, gentle massage may sometimes be part of aftercare. If the issue is infection, active inflammation, unstable scabs, or a fresh wound, aggressive rubbing can make the situation worse.
Automatic advice can be risky. Massage this, squeeze that, scrub harder, wait longer. The scalp deserves a diagnosis before treatment. A raised area after a transplant may have several causes, and each cause needs a different response.
During the first 10 to 14 days, handle the recipient area very carefully. At this stage, clean healing matters more than force. Scabs need to soften and separate according to the clinic washing routine, not be ripped away by impatience. The hair transplant aftercare guidance explains why gentle timing matters so much during this period.
After the early phase, patients sometimes begin pressing or rubbing the scalp because they feel bumps. This can create more redness and more anxiety. It can also hide the original problem because the skin becomes inflamed from the patient’s own manipulation.
Oils, strong shampoos, concealers, fibers, or topical products used too early can also confuse the picture. Some products irritate the scalp or block follicles when the skin is still settling. The patient may think the transplant created every bump, when irritation added during recovery may be part of the picture.
It would be wrong to read this as every product is harmful. It means timing matters. A scalp that is settled at 3 months can tolerate more than a scalp that is still red, itchy, and healing at 3 weeks.
If a clinic recommends massage, the instruction needs to be specific and based on examination. Ask for the purpose, the timing, the level of pressure, and when to stop. Vague advice can be risky on a healing scalp.
Before trying anything forceful, document the area under normal light and close light. Those photos can help the clinic decide whether the bump looks inflammatory, scarred, or simply part of healing.
Treatment timing and repair timing
Treatment depends on the cause. If the weak point is mild folliculitis, a doctor may recommend local treatment, changes in washing, or medication when needed. If the weak point is irritation from products, the answer may be stopping the irritant and letting the scalp settle. If the issue is raised scar texture, the discussion becomes different.

Many patients try to treat every bump with squeezing, strong oils, aggressive massage, or random creams. The scalp may already be irritated. Adding more trauma can make the story harder to read and sometimes worse.
When the concern is a true ridge or cobblestoning, repair should usually wait until the skin and hair result have matured enough to judge. In selected cases, a doctor may consider treatments for scar response, but that decision requires examination. A cosmetic repair plan should not be made from one early photo.
If the surface problem remains after the result matures, the discussion becomes diagnostic. Is the skin raised, are the grafts too visible, is the hairline pluggy, is the direction wrong, or is the main issue density? A bad hair transplant repair plan only makes sense after the real cause is understood.
Bumps, ridges, and hair growth
They can, but not always. A small temporary bump does not mean the graft under it is lost. A mild pimple that settles properly may have no meaningful effect on the final result. The concern becomes stronger when inflammation is severe, repeated, untreated, or connected to scar tissue.
Hair growth depends on graft survival, blood supply, skin health, and time. If the skin heals without repeated inflammation, the transplanted hairs have a better environment. If the skin is repeatedly inflamed or scarred, predictability can decrease.
Patients often judge too early because the surface looks strange while the hair is absent. The shedding phase can make every irregularity look more obvious. I separate surface healing from density judgment.
A patient who is worried about weak growth should not mix every concern together. The question of low density at 4 months after a hair transplant is mostly about timing and growth biology. A raised ridge is more about skin texture and healing quality. They can appear together, but they are not the same problem.
If hair begins to grow through a mildly bumpy area and the skin is settling, that is reassuring. If the area remains firm, shiny, painful, red, or uneven while growth stays poor, it needs a more careful examination.
Repair planning should not begin too early unless there is an urgent medical issue. Most cosmetic concerns need enough time for the result to mature before a repair plan is fair. Medical problems, infection, black tissue, or worsening wounds are different. Those should not wait for 12 months.
Warning signs that should not be ignored
You should not ignore spreading redness, increasing warmth, pus, fever, worsening pain, thick wet scabs, open wounds, black tissue, sudden swelling, or a ridge that is becoming more obvious instead of softer. These signs do not all mean the same thing, but they all deserve a serious response. If the surface concern sits mainly at the front, review the more specific discussion of a bumpy hairline after FUE as well, because frontal contour can remain visible even after growth improves.
Black scabbing deserves special attention. Most scabs are harmless, but dark, painful, wet, expanding, or open areas require medical attention the same day. Rare complications should be handled without panic, but quickly, especially when judging black scabbing after a hair transplant.
A clinic that refuses to look closely is another concern. A worrying scalp change deserves more than a brief answer. The clinic needs timing, symptoms, photos, washing routine, medications, and whether the area is improving.
If the skin has a raised line but no pain, no redness, and no discharge, it may not be urgent in the same way as infection. But it can still matter cosmetically. A surface texture problem near the frontal hairline can remain visible after hair grows.
Psychological pressure also matters. If the patient is repeatedly checking the scalp under harsh light, they may need reassurance and structure. But if the physical sign is real, reassurance should not become dismissal.
Panic does not help, but vague reassurance does not help either. The useful step is a proper diagnosis.
Prevention starts with careful clinic planning
Prevention starts with responsible density planning, recipient area openings made with the right angle and depth, respect for blood supply, careful graft selection, and surgery that is not turned into a race for the biggest number. This is true whether the procedure is a small refinement or a larger FUE hair transplant session.
The surgeon should understand the patient’s skin, hair caliber, donor capacity, recipient area needs, and future hair loss. If the plan is too aggressive, the scalp may pay the price. The responsible graft number is not always the largest number.
Naturalness is not only about hair direction. It is also about how the skin heals around the hair. A hairline can grow hair but still look artificial if the skin surface is uneven or the graft placement looks harsh.
This connects closely with pluggy hairline after a hair transplant. Thick grafts, wrong placement, poor angulation, and visible surface change can all make the front look less natural, even when growth technically occurs.
Surgeon involvement matters because the recipient area design is not a minor step. The person who creates the openings controls direction, angle, depth, spacing, and density. These decisions influence both growth and surface appearance.
Skin condition should also be documented before surgery. A patient with previous acne scarring, recent isotretinoin use, psoriasis, seborrheic dermatitis, folliculitis history, thick scar tendency, or previous surgery may not heal exactly like a patient with skin that is settled and not inflamed. The plan should respect that difference.
Recipient area planning is not only about how many grafts can fit. It is also about how the skin will accept them. Patients rarely see this detail in advertisements, but it can affect how natural the result looks later.
Know who performs your hair transplant before you book surgery. A clinic that cannot clearly explain surgical responsibility is not giving the patient enough information to consent intelligently.
The consultation should not be built only on photos. Photos can start the discussion, but they cannot show skin thickness, scarring tendency, inflammation, and many details of scalp quality. The limits of a hair transplant plan from photos alone become very clear when the concern is healing quality.