



Who Performs Your Hair Transplant Surgery?
Before you book, you should know who examines the donor area, who designs the hairline, who gives the anesthesia, who extracts grafts, who creates the recipient area incisions, who places the grafts, and who remains responsible after surgery.
The clinic name is not enough. A package name is not enough. A technique label is not enough. Hair transplantation is a medical operation on a limited donor supply, so the answer has to be practical, not vague.
A trained team can help during surgery. That is normal. The important distinction is whether the team supports a surgeon-led plan or whether unclear staff members are replacing the surgeon in decisions that should be medically accountable.
Many people compare package prices, hotel transfers, and graft numbers before asking who actually controls the operation. The safer order is the opposite. First clarify responsibility. Then compare price, travel, technique, and convenience.
This question matters because the hairline drawing, donor extraction pattern, density plan, recipient area incisions, and follow-up strategy are not small service details. They decide whether the result can mature naturally or create regret later.
The clinic name is not the surgical plan
A clinic can look polished before surgery. The website can be professional, the coordinator can answer quickly, the transfer can be smooth, and the photos can look convincing. None of that tells you who made the medical decisions on the day of surgery.
On the operating day, the result is created by diagnosis, donor management, hairline planning, anesthesia control, extraction pattern, graft handling, incision angle, direction, density distribution, and disciplined follow-up. A logo does not make those decisions. I treat daily patient volume in hair transplant surgery as part of that accountability, not a separate business detail.
Travelling abroad can make the process feel organized before surgical accountability is clear. A pleasant trip can make the whole process feel organized, but travel organization is not surgical accountability. You are not only buying a service. You are trusting someone with the only donor supply you will ever have.
Assistants and technicians are not the problem by themselves. A trained surgical team matters. The problem begins when the team replaces the surgeon’s judgment, or when the patient cannot clearly understand who is responsible for each critical step.

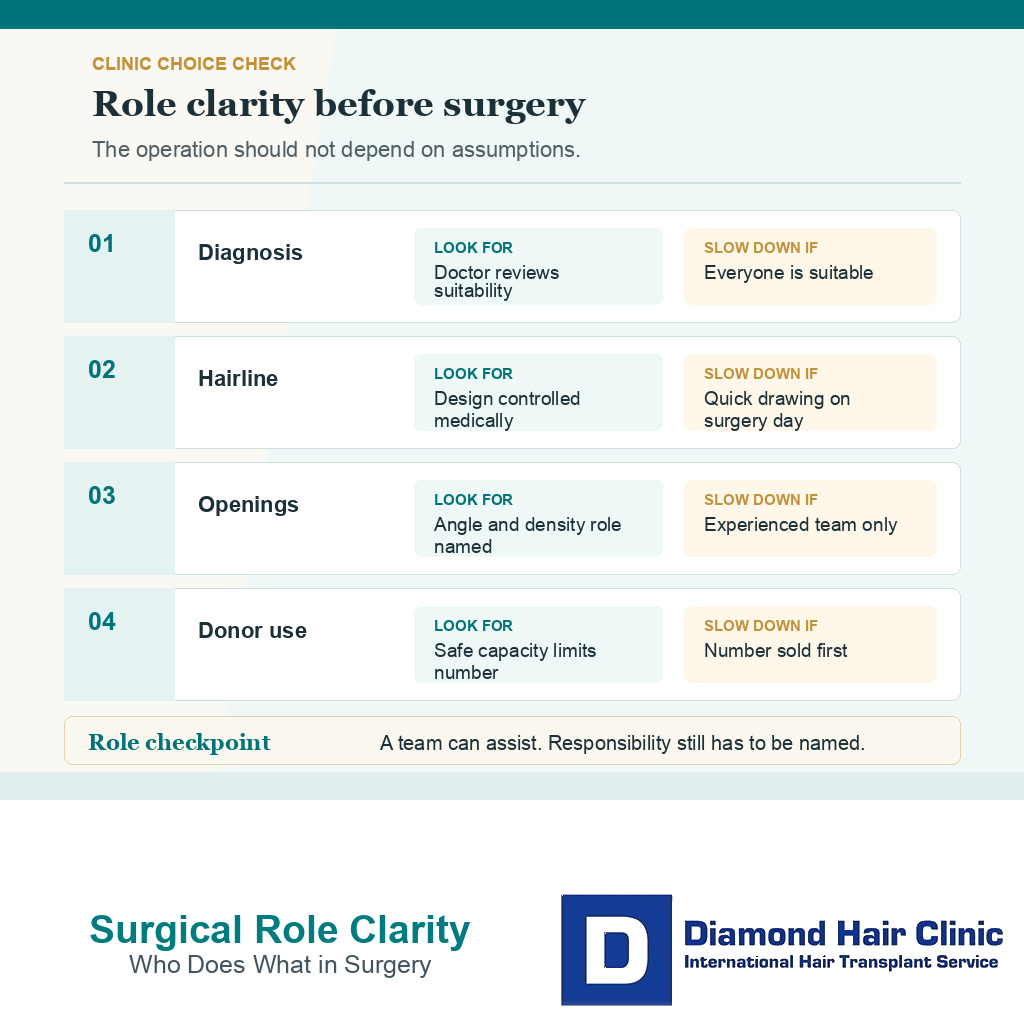
Surgical steps that need clear role ownership
Start with diagnosis and donor examination. A photograph can begin the conversation, but it may not be enough for younger men, diffuse thinning, possible retrograde loss, weak donor areas, previous surgery, or anyone likely to need more than one session.
Hairline design also needs a clear owner. It is not just a line drawn on the forehead. It decides facial framing, age suitability, density distribution, soft irregularity, temple behavior, and whether the result will look natural in ordinary life.
Anesthesia, extraction, recipient area incision creation, graft placement, and graft handling should be explained as one medical chain. Local anesthesia is common, but it still requires careful dosing and monitoring. Extraction affects donor thinning and future reserve. Recipient area incisions decide angle, direction, depth, and distribution. Graft handling affects survival because follicles are living tissue.
When these roles are explained clearly, you can judge the clinic more fairly. When they are hidden behind a package name, the responsibility is not clear enough for permanent surgery.
The 10 role clarity slides below separate named medical ownership, donor review, hairline design, anesthesia, extraction, incision planning, team boundaries, surgery day changes, red flags, and travel decisions. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.

Role clarity before surgery
Make the roles visible before you commit. That means knowing who evaluated the hair loss, who recommended surgery, who designed the hairline, and who will be involved in the operation. A doctor name in marketing is not enough if the critical work is handed to people the patient never properly understands.
Role clarity should be written plainly. The clinic should be able to explain which steps are performed by the surgeon, which steps are assisted by the team, and who remains responsible if the plan changes or a problem appears after surgery.
What I want clear in writing before travel?
Before a patient travels, role clarity needs to be written plainly. The plan needs to name who evaluated the case, who designed the hairline, who decides donor limits, who creates the recipient area incisions, and who remains responsible if the graft number or design has to change.
If the written plan cannot answer those points, the decision is not ready. A patient cannot be asked to discover on surgery day that the surgeon’s role is different from what the clinic suggested before booking.
The same document also has to name what would make surgery smaller, staged, or refused for now. A weak donor supply, unstable hair loss, unclear diagnosis, or a requested hairline that spends too much donor hair should change the plan before payment or travel pressure takes over.
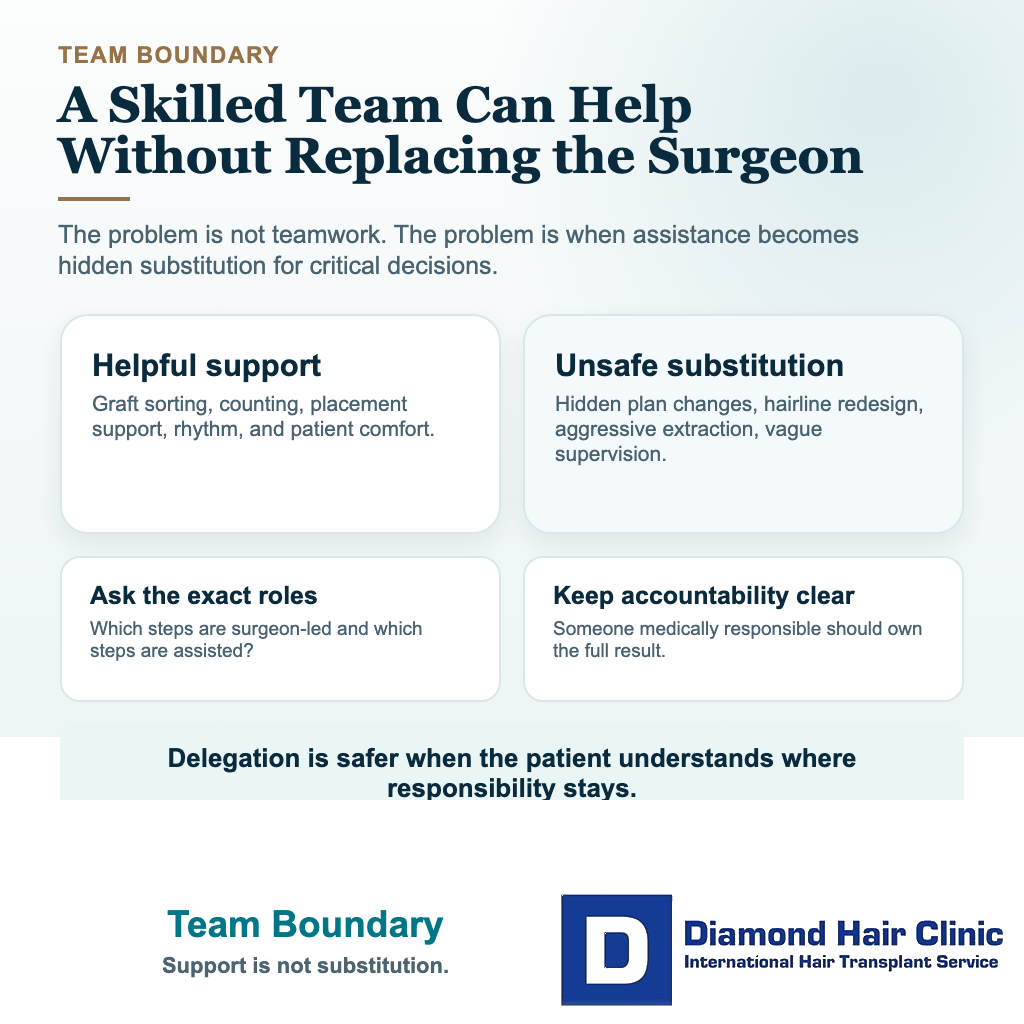
Technicians can help without replacing the surgeon
Yes, when the boundary is clear. Hair transplantation is team surgery. Experienced assistants can help with graft counting, graft sorting, placement support, patient comfort, and the rhythm of the operation.
Delegation becomes unsafe when it turns into substitution. A technician may be skilled, but that does not make the technician the right person to diagnose the case, redesign the hairline, increase the graft number, decide donor limits, or perform critical steps without proper medical responsibility.
Words such as team, doctor supervised, expert staff, or advanced technique can sound reassuring. They still do not answer the practical question. Who is doing what, and who is accountable if the result does not develop as expected?
If a clinic becomes defensive when asked, that reaction matters. A careful clinic can explain its surgical setup without making the patient feel guilty for asking.
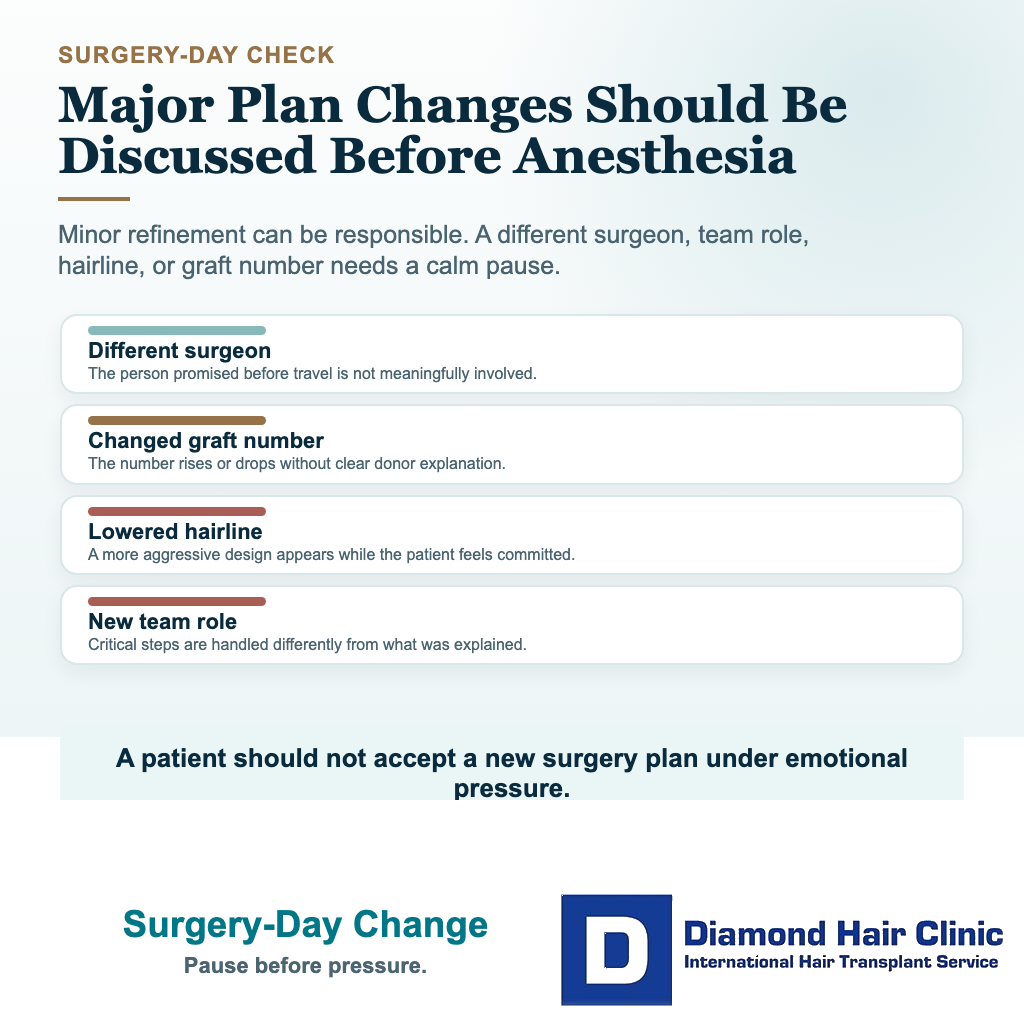
Plan changes on surgery day need surgeon explanation
A plan can change after direct examination. The donor may be weaker than expected, the hairline may need a safer position, or the graft number may need to be reduced. That kind of change can be responsible medicine when it is explained clearly.
What worries me is a different kind of change. If the surgeon named before travel is not meaningfully involved on surgery day, if the graft number increases under pressure, if the hairline is lowered without a real discussion, or if the team role is different from what you were told, pause before anesthesia or extraction begins.
A minor refinement is different from a changed promise. If the plan no longer matches what you understood before committing, it deserves a careful conversation. The guide to a changed graft number on the day of surgery explains this distinction in more detail.

Red flags that suggest surgery is being sold like a package
One warning sign is a confident graft number without proper examination. A number can be estimated from photographs, but a responsible plan needs more than a quick look at the front of the scalp.
Pressure is a serious signal. If a special discount, limited surgery slot, or financing offer is used before the medical plan is clear, the conversation has moved away from surgery and toward sales.
Be careful when FUE, DHI, Sapphire FUE, robotic FUE, or another method is sold like a menu choice. The technique needs to serve the patient. It does not replace diagnosis, donor planning, surgeon judgment, or follow-up.
A clinic that promises maximum density in one session also deserves caution, especially for young patients, advanced hair loss, crown demand, or a weak donor area. Dense packing may sound attractive, but density without future planning can create problems later.
These are some of the same concerns I discuss in the guide to red flags of Turkish hair mills. The issue is not Turkey itself. The issue is any clinic, in any country, that treats surgery like a production line.
Hairline design needs surgeon responsibility
Hairline design is one of the places where people often recognize the problem too late. A low, straight, dense hairline can look exciting immediately after surgery because it seems dramatic and youthful.
But a hairline must belong to the face, age, donor capacity, hair caliber, temple pattern, and future hair loss pattern. A hairline that looks impressive on day one can become unnatural later if it ignores those factors.
In natural hair, the front edge is not a ruler line. It has softness, small irregularities, single grafts at the front, correct angles, and gradual transition. If grafts with several hairs are placed too far forward, the result can look artificial even when the grafts grow.
My responsibility is not to draw the lowest possible line. It is to design a line that can age well and still make sense if native hair changes later. For that reason, hairline design belongs inside the surgical plan, not as a quick drawing before the operation begins.
Surgeon involvement protects the donor area
The donor area has to last for life. Once a graft is removed and used, it cannot be used again somewhere else. A plan that focuses only on first visual impact can spend too much of that reserve too early.
During donor examination, I am not only looking at how much hair exists today. I am judging how much can be removed without making the donor look thin, how future hair loss may progress, and whether a second or third session may be needed later.
This is where surgeon involvement matters deeply. Someone has to know when to say no, when to reduce the graft plan, when to protect the crown for later, and when surgery is not advisable yet.
The way graft numbers are calculated makes the same point. The number itself is not the goal. The goal is careful distribution of a limited resource.
Low price and good photos are not enough to choose a clinic
No. Price comparison is understandable. A lower price can still come from a clinic with a careful process, and a higher price can still hide weak planning. The deciding issue is whether the process still allows enough time, skill, medical responsibility, and follow-up for your case.
Two clinics may both say FUE, quote a similar graft number, and show attractive photos. The actual surgical planning can still be completely different.
Medical tourism can work well when the clinic is transparent and the surgeon is accountable. It becomes risky when the patient is moved through a high-volume schedule with little individual planning.
Do not judge only by selected photos. Ask for healed donor photos, similar cases, ordinary lighting, and an explanation of what happens if growth is poor or the plan needs review.
When missing role proof makes me slow down?
When a patient cannot get a written answer about who evaluates candidacy, who designs the hairline, who makes the incisions, who supervises graft work, and who changes the plan if donor review changes, I treat that as a medical planning problem, not a small communication detail.
I may delay surgery when the answer is still unclear after a deposit, when a coordinator gives medical certainty without surgeon review, or when the plan depends on a graft number without named surgeon responsibility. The patient needs to know role ownership before travel, not while sitting in the preoperative room.
Written role proof does not mean every assistant task disappears. It means critical decisions have a named surgeon, team roles have limits, and any plan change has a medical reason that is documented before surgery continues.
Details you need before you say yes to surgery
Before agreeing to surgery, you should be able to describe your own plan in plain language. If you cannot explain the main responsibilities, the reason for the graft number, the hairline logic, and the future plan, you may not have enough information yet.
By the time you book, responsibility should not feel mysterious. You should know who examined the donor area, who designed the hairline, who controls extraction, who creates the recipient area incisions, who places the grafts, and who supervises the grafts while they are outside the body.
Aftercare also needs to be clear before surgery. Good aftercare is not extra products. It means clear instructions, gentle washing, graft protection, avoiding unnecessary touching, and realistic expectations during shedding and slow growth.
Choose the surgeon and the plan before you choose the package. Choose transparency before convenience. Choose donor preservation before a dramatic first impression.
A hair transplant should not leave you wondering who was responsible. Every step, from consultation to follow-up, should make sense for your face, donor area, future hair loss, and long-term comfort.