Hair Transplant Regret Needs Calm Review
If regret appears after surgery, do not let the first emotional wave make the next decision. First separate emotional panic from true medical warning signs. Then review the timeline, photos, graft plan, donor area, hairline design, and symptoms with the clinic that treated you.
Early regret can be part of recovery anxiety. It can also point to a real planning problem. Those two situations need different responses.
Do not rush into repair, shaving, aggressive camouflage, or another surgery before the result is mature enough to judge. A week six photo, a red scalp, a shedding phase, or a harsh bathroom light picture is not the same as a final result. If there is fever, worsening pain, spreading redness, pus, dark tissue, open wounds, or clear donor damage, that is no longer only regret. That needs medical review.
Regret is easier to prevent before surgery than to repair after surgery. I do not treat a hair transplant as a quick cosmetic upgrade because it changes the hairline, donor area, daily appearance, and sometimes the emotional state for many months. Second thoughts before hair transplant surgery deserve a calm review before any grafts are moved.
If you were wearing a hair system before surgery, the risk is different. A system can create a density expectation that surgery may not safely match, so the discussion must include density expectations created by the hair system before surgery.
Regret can come from the waiting period, a weak surgical plan, poor clinic communication, unrealistic density promises, donor overuse, a hairline that does not suit the face, or a result that is simply too early to judge. The aim is not only to avoid a bad result. The aim is to avoid a decision that later feels rushed, poorly explained, or poorly matched to your long-term hair loss pattern.
First steps after early hair transplant regret
Start with facts, not another operation. Write down the surgery date, graft number, treated areas, medicines, symptoms, and the exact change that worries you. Take clear photos in normal light from the same distance and angle. Then send them to the clinic that operated on you.
Do not shave the recipient area aggressively, book a repair immediately, start random treatments, or compare your early recovery to someone else’s mature result. If you need to document progress, track hair transplant growth with repeatable lighting, distance, hair length, and camera angle.
The urgent exception is medical safety. Severe or worsening pain, fever, spreading redness, pus, bad smell, dark tissue, black scabbing, open wounds, or a donor area that looks damaged should be reviewed quickly. Those signs belong closer to the urgent concerns described in hair transplant necrosis warning signs.
If the regret is affecting sleep, appetite, work, relationships, or your sense of safety, do not dismiss it as vanity. The scalp can be assessed medically while you also get emotional support. If you feel at risk of harming yourself, seek urgent local medical or crisis support immediately.
Regret deserves attention, but it must not be allowed to make the next surgical decision for you.
Regret can appear before the result has failed
Early regret often appears in the first days, weeks, or months. You look in the mirror and think, “What did I do?” That reaction can feel very real because the early appearance is not gentle. The scalp may be red. The grafts may look obvious. The hairline can look harsher than expected while the skin is healing and the transplanted hairs have not shed or softened yet.
Then the shedding phase begins. Many transplanted hairs fall out temporarily, and it can feel as if the result is disappearing before it has started. Timeline counseling matters before surgery for exactly this reason.
The ugly duckling stage is one of the hardest periods emotionally. A month two or month three photo should not be judged against another person’s month twelve result. That comparison is common, but it is not fair to your scalp or to your mind.
Isolation can make the feeling worse. Some people take a few days off work, then realize they were not prepared for the social discomfort. They avoid friends, avoid photos, check the mirror too often, and treat every scab, hair, or patch as proof of failure.
That does not mean every worry is meaningless. Some worries are premature. Some deserve review. If that question is still unclear, review whether a hair transplant has really failed or is being judged too early before deciding the result has failed.
Starting point details often underestimated before surgery
The starting point matters more than many people expect. Age, donor strength, hair caliber, future hair loss, scalp contrast, crown size, previous surgery, and medical stability can all change the plan. Two men with similar recession can need very different strategies.
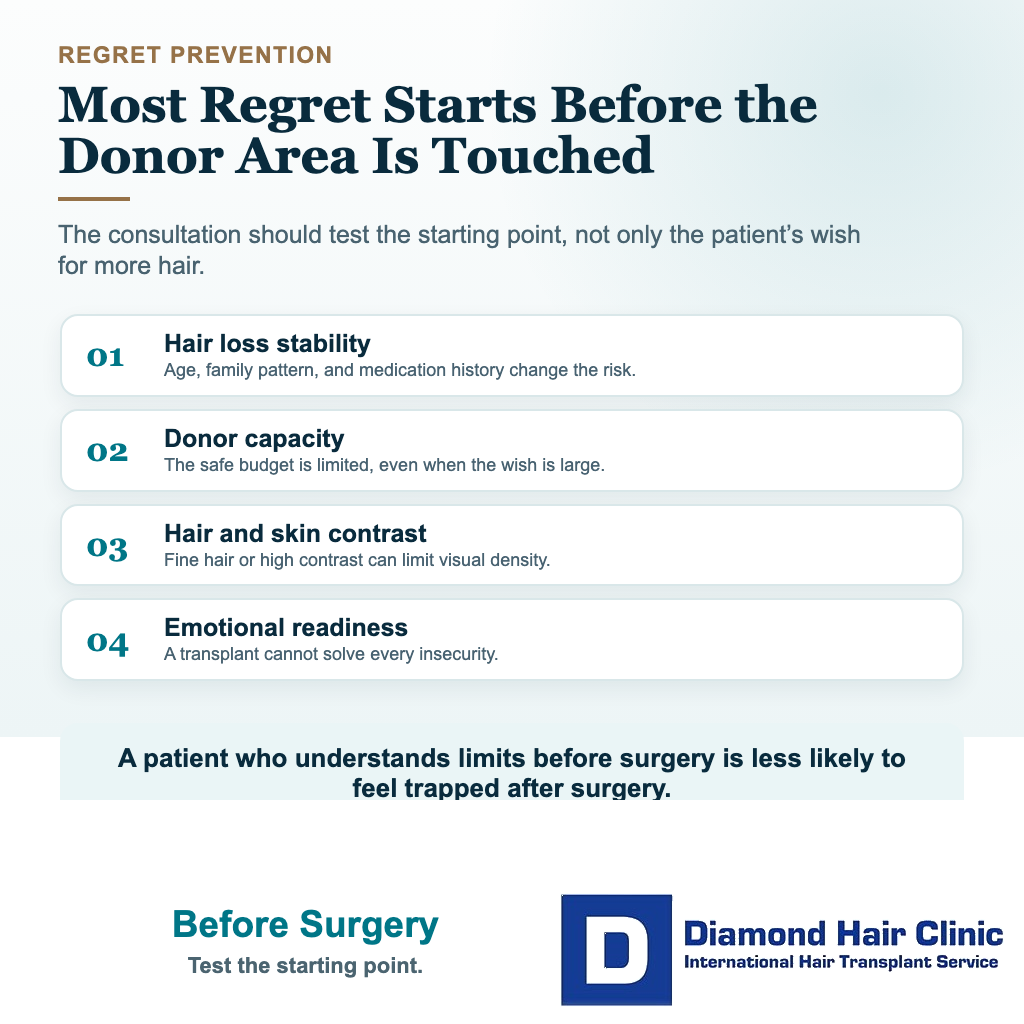
A proper evaluation is not only about how many grafts you want. The first question is whether the operation makes sense at all. Someone who is not a good candidate for a hair transplant yet may have unstable hair loss, unrealistic density expectations, or a donor area that cannot safely support the requested plan.
The emotional weight is also easy to underestimate. Before surgery, it is natural to imagine better photos, easier styling, and feeling more like yourself again. Those benefits can be real, but a transplant should not be asked to carry the entire burden of confidence, dating, personality, or sense of self.
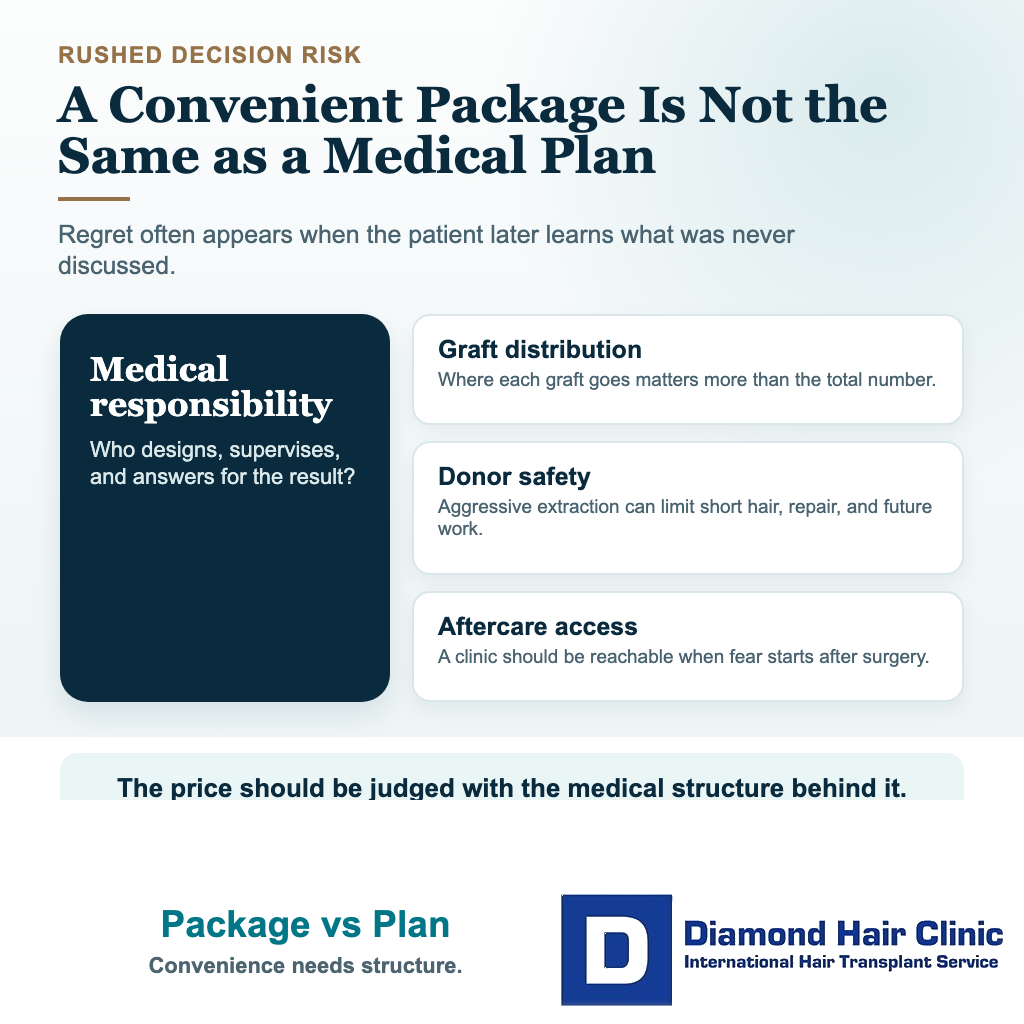
The clinic structure matters too. Before committing, you should know who designs the hairline, who is medically responsible for the recipient area, who performs the critical surgical steps, and whether several people are being treated on the same day. This is not suspicion. It is informed consent before committing to a hair transplant.
Cheap or rushed decisions can create later regret
Price is one of the most common pathways into regret. It is understandable to compare clinics because surgery can be expensive. The problem begins when the visible fee becomes more important than the medical structure behind it.
A cheaper clinic may still produce good results in some cases, but a low fee and hair mill red flags should not be ignored. Proper planning, surgeon involvement, careful graft handling, and long-term accountability still matter.
Packages can make the decision feel solved. Hotel, transfer, surgery, washing, medication, and graft number are placed into one convenient offer. Convenience can help travel planning, but it is not the same as quality.
Regret often appears later when someone realizes the surgeon was not involved enough, the hairline was drawn too quickly, the donor area was harvested too aggressively, or the crown was promised without enough donor capacity to cover it naturally.
A low price becomes expensive when the result needs repair. Corrective work can require more time, more money, more emotional energy, and more donor hair than a careful first operation would have required.
Temporary discounts and urgent booking language deserve caution. A salesperson’s deadline should not decide surgery. The decision should come from a medical plan that still feels sound after the urgency has passed.
The real cost also includes travel, hotel quality, time off work, medicines, follow-up access, communication problems, and possible corrective work. If you are comparing clinics seriously, judge hair transplant cost in Turkey inside that wider decision, not only by the advertised package price.
Donor planning protects future peace of mind
The donor area is the part of the scalp many people understand too late. Before surgery, most attention goes to the front. After surgery, especially if the back and sides look thin, patchy, or overharvested, the donor area suddenly becomes the real budget.
Every graft taken from the donor area has an opportunity cost. It can improve one area today, but it cannot be used again tomorrow. Grafts should never be treated as a plain number to win a consultation.
When too many grafts are removed in one session, options shrink. Short hairstyles may become harder. A fade may reveal uneven extraction. A second procedure may become more limited. Repair may become less possible.
Overharvesting can be emotionally painful because it damages the part of the scalp the person did not expect to worry about. The recipient area may look acceptable, but the back and sides may no longer feel strong enough.
Careful donor management is not weak planning. It means using enough grafts to create visible improvement while still protecting future choices.
The crown is part of this decision. Crown coverage can consume many grafts because the area is round, changes direction, and often looks lighter under overhead light. If donor strength is limited, trying to cover everything in one session can create thin coverage everywhere.
A limitation explained before surgery is easier to accept than an apology after surgery. People can usually accept limits when they are told clearly. Resentment grows when the limit is hidden until it becomes visible.
Donor area overharvesting can limit every repair option later.
Hairline design can create relief or long term frustration
The hairline is emotionally powerful because it frames the face. It changes photos, mirrors, and daily appearance. It is also one of the easiest areas to damage aesthetically if the plan is too aggressive.

Many people ask for a lower hairline because they want to return to an earlier version of themselves. That feeling is real. Hair loss can make a person feel older than they are, and a stronger frame can help.
But the hairline must belong to the face, age, donor capacity, and future hair loss pattern. A very low or very straight hairline may look exciting in the first photo, then become unnatural as the person ages or as native hair continues to thin behind it.
Natural hairlines are not perfect lines. They need softness, small irregularities, correct direction, careful transition, and single grafts at the front. They should not look like a sharp border placed onto the forehead.
Regret often appears when someone realizes that density alone does not create naturalness. A dense but poorly designed hairline can attract more attention than a moderately dense but properly designed one.
The hairline also spends donor hair. Lowering it even a little can require many grafts. If those grafts are spent in the wrong place, the middle scalp or crown may be harder to treat later.
Hairline design follows this same long-term planning logic. It is not decoration. It is surgical planning, facial analysis, donor management, and artistic judgment working together.
Recovery can feel harder than expected
Many people think recovery means protecting the grafts for a few days. In reality, recovery has several layers. There is physical healing, social discomfort, shedding, the long waiting period, and the habit of checking too often.
The first nights can be tiring. Sleeping with the head elevated, avoiding pressure on the recipient area, managing swelling, and dealing with donor tenderness can feel more restrictive than expected.
Itching, numbness, redness, tightness, and scabbing can also create anxiety. Someone may worry that washing will damage grafts, or that a scab with a hair inside means a follicle has been lost. Aftercare needs to be explained clearly, not handed over as a vague instruction sheet.
Clear hair transplant aftercare is not only a list of rules. It is the structure that helps you understand what to protect, what to expect, and when to contact the clinic.
Around days ten to fourteen, many people feel more socially comfortable, but the cosmetic process is still just beginning. This false sense of normality can make them return too quickly to hard exercise, sweating, sun exposure, or unnecessary touching.
Photography can become another problem. Bathroom light, car light, wet hair, harsh sunlight, and different hair lengths can all make the same scalp look different. Structured observation is useful. Daily panic photography is not.
Photos need to be taken consistently, but not obsessively. For follow-up, timing, symptoms, and repeatable pictures help more than a new frightening angle every hour.
Emotional regret is different from real warning signs
Emotional regret usually fluctuates. It becomes worse with the mirror, worse during shedding, and often improves when the timeline is explained. The worry is real, but the clinical signs do not clearly show failure.
When the signs fit that pattern, the better response is time, proper follow-up, consistent aftercare, and realistic observation. Do not make permanent decisions during a temporary emotional phase.
Real warning signs are different. Severe or worsening pain, infection signs, abnormal scarring, obvious pitting, cobblestoning, unnatural growth angles, clear overharvesting, or a clinic that avoids direct answers should not be dismissed.
A plan may be unsafe when it never made sense. A very young person with aggressive hair loss may receive a low, dense hairline without enough discussion of future thinning. Someone with a weak donor area may be promised full coverage of the front, middle scalp, and crown in one session.
Sometimes regret is not about early healing. It comes from realizing that the consultation was shallow. Nobody explained donor limits, nobody discussed future hair loss, and nobody clarified who would perform the critical stages of the operation.
If a second procedure becomes a real consideration, slow down. Do not rush into a small correction at month four or month five just to reduce anxiety. Many results need at least 12 to 18 months, and some need longer, sometimes 24 months, before a responsible repair or second stage decision can be made.
A second hair transplant is worth considering only when the visible benefit justifies the remaining donor cost.
Choices before commitment that reduce regret
The best prevention is slowing the decision down before the donor area is touched. Sometimes that means getting a second opinion before a hair transplant. A rushed person is easier to sell to, but not easier to treat well.
Before committing, you need a real conversation with the surgeon who will be medically responsible for the result. The discussion should cover hairline design, recipient area planning, graft distribution, donor limits, future hair loss, and how many people are treated on the same day.
A total graft number without distribution is incomplete. You need to know how many grafts are planned for the hairline, frontal area, middle scalp, and crown, and why those priorities were chosen.
Follow-up matters too. The clinic should explain how it handles slower growth on one side, dramatic shedding, longer redness, or anxiety after you return home. A careful clinic does not disappear after the operation day.
Ask yourself one private question before committing. Are you choosing the clinic because you trust the medical plan, or because the price, hotel, discount, social media result, or fear of missing the offer made the decision feel easier?
A hair transplant should make your future simpler, not more complicated. Choose a plan you can still respect years later, after the excitement of booking has passed.