Uneven Hairline Growth Needs Timeline Review
An uneven hairline after a hair transplant can be temporary, or it can be a real design issue. Early swelling, scabs, lighting, camera angle, uneven shedding, and one side growing faster can all make the hairline look unbalanced before the result is mature. A true design problem is different. It remains visible after healing, conflicts with the agreed plan, or looks mismatched at normal conversational distance.
Separate healing distortion, normal soft irregularity, uneven growth timing, and structural imbalance. Those are not the same problem, and they do not need the same response. Early anxiety needs good photos and time. A changed or poorly designed hairline needs a surgeon to review the plan directly.
The hairline can look uneven early in recovery
In the first days and weeks, the recipient area is not a clean design drawing. Swelling can settle more on one side. Scabs may be thicker along one temple. Redness can be stronger in one corner. A phone held slightly off center can make a small difference look dramatic.
At that stage, judging hair transplant day one photos needs caution. A day one photo can show the intended placement, but it cannot prove final symmetry, density, or growth. The skin is still reacting to surgery.
A fair way to check the hairline
A fair check uses comparable photos, not random mirror moments. Take a straight front photo, both side angles, relaxed forehead, same lighting, same distance, and no tilted phone. Compare those with the preoperative marking photo and immediate postoperative photo if you have them.
Do not judge the hairline from one close selfie under bathroom light. Close photos exaggerate tiny differences. Raised eyebrows, a turned head, or uneven forehead muscles can also make one side look higher or lower.
If the concern changes from photo to photo, it is often distortion. If the same imbalance is visible in several fair photos after swelling and scabs have settled, it deserves closer review.
Some asymmetry can be normal in a natural hairline
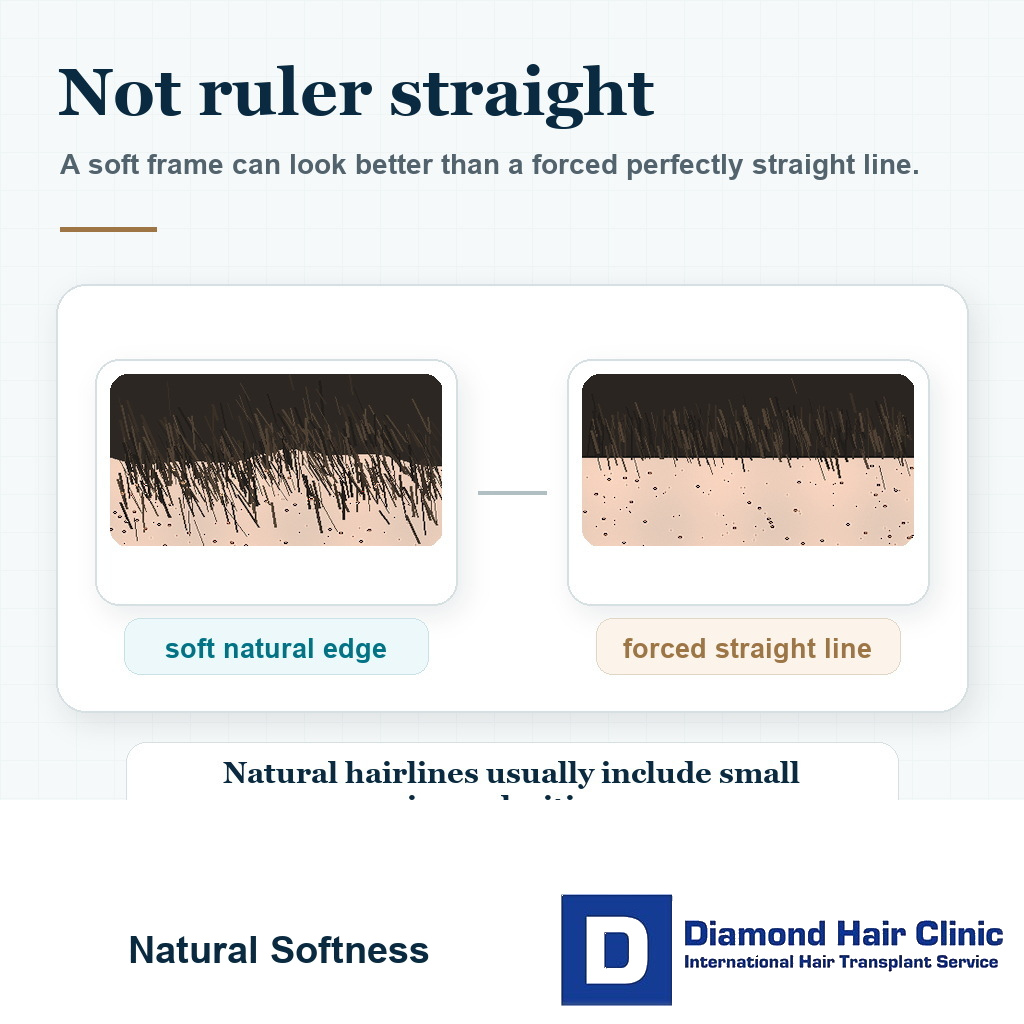
Yes. A natural hairline is not a ruler line. Real hairlines have small irregularities, softer front hairs, different corner behavior, and slight asymmetry that fits the face. Exact mirror symmetry can look artificial.
Hairline design in hair transplant is not only about lowering the line. The surgeon has to consider age, donor reserve, face shape, temple recession, hair caliber, future hair loss, angle, direction, and how the line will age.
A natural result does not require the left and right sides to be copied exactly. It requires a hairline that fits the face.
Unevenness becomes a design problem when the pattern persists
I become more concerned when one side sits clearly higher or lower, the corner shape is very different, the implanted line does not match the approved marking, or the imbalance is visible from normal distance without zooming.
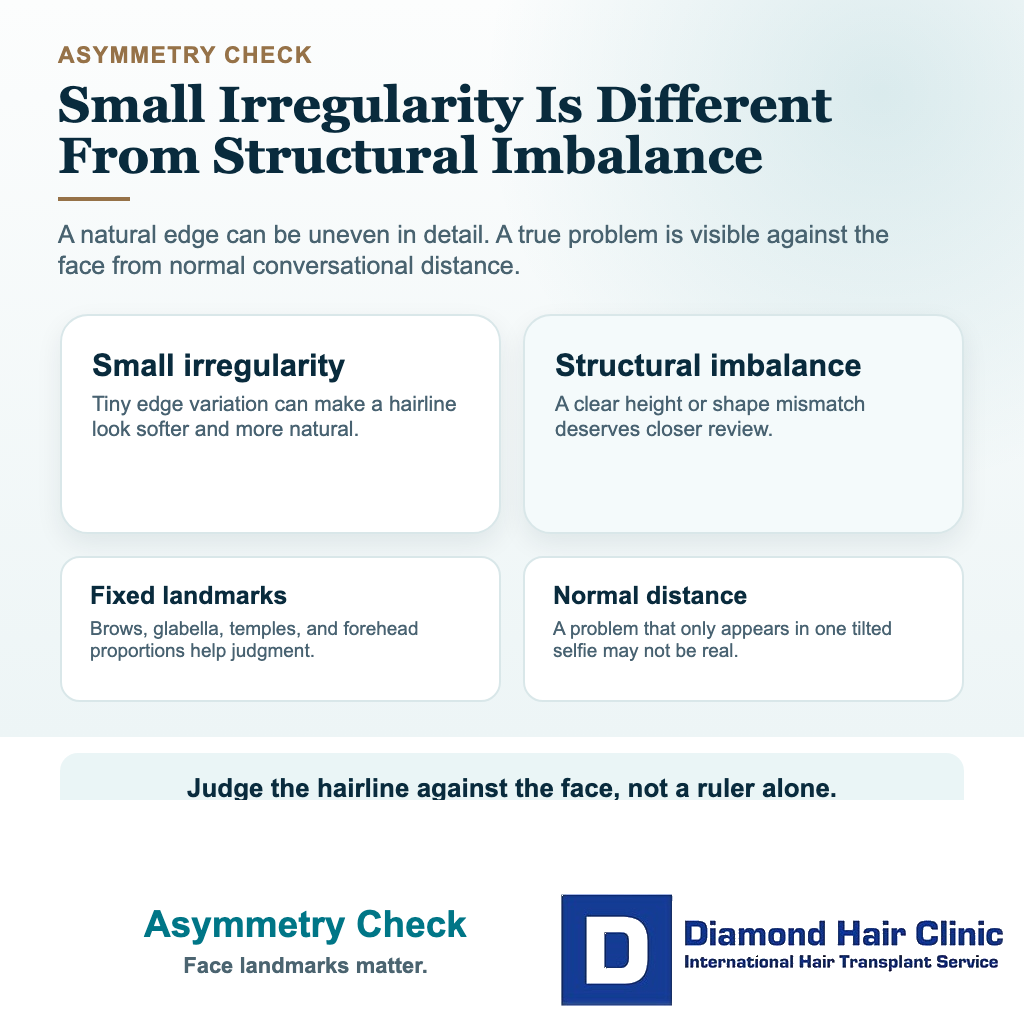
Small softness at the front is different from structural imbalance. Small irregularity helps a hairline look natural. Structural imbalance changes the way the face is framed.
Useful landmarks include the central point, temples, eyebrows, forehead shape, and facial asymmetry. A human face is not a measuring grid, so small differences must be interpreted clinically. But facial asymmetry should not be used as an excuse for a poorly controlled recipient area.
One side can grow more slowly
Yes. One side can shed earlier, wake up later, or look thinner for several months. That does not mean the design was wrong or that grafts failed. Growth is biological, and both sides do not always mature at the same pace.
If the main concern is growth rather than planted shape, compare it with one side of the hair transplant growing slower. A hairline can look uneven because density is behind on one side, not because the line itself was misplaced.
A month eight hairline check is usually more useful than a week two judgment when the concern is growth timing. The final decision often needs the 12 month result, and sometimes longer in slower growers.
The surgeon should explain any changed hairline plan
If the clinic marked one hairline and implanted a meaningfully different shape, the concern is serious. The patient deserves a clear explanation from the surgeon, not vague reassurance from a coordinator.
In the hairline zone, recipient area planning is one of the most visible surgical decisions. Angle, direction, depth, density, transition softness, and corner shape determine whether the result belongs on the face. That is one reason who performs the decisive parts of surgery matters.
If the hairline plan changes, it should be explained with surgical reasoning, not dismissed as patient anxiety.

A lower, straighter hairline is not always better
No. A very low, flat, sharp hairline can look exciting immediately after surgery and still age badly. It can consume donor grafts, fight the natural shape of the face, and create a repair problem if future hair loss continues behind it.
A mature design is not a timid design. It is a design that protects naturalness and donor reserve. The answer is not to make every uneven concern lower and straighter. The answer is to decide whether the current shape is healing normally, naturally irregular, growing unevenly, or structurally wrong.
If the issue is hairline position rather than side by side balance, hairline height after a hair transplant needs a separate review.
The right time to ask for a review
Ask for a review if the imbalance is clear in fair photos, if the implanted line does not match the agreed marking, if one side has a different shape that does not fit the face, or if the clinic cannot explain who made the design decision.
It is reasonable to ask for the preoperative marking photo, the immediate postoperative hairline photo, and a calm explanation of whether any design change was made during surgery. The clinic should be able to have that conversation clearly.
A consistent sequence of comparable photos is more useful than daily close-ups under different lights. Document the same view and give the tissue time to settle unless there is pain, infection concern, or another medical issue.
These 10 uneven hairline review slides separate early growth asymmetry from design mismatch, photo evidence, repair timing, graft direction, donor reserve, and when a surgeon should review the plan. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.