



One Side Growing Slower Needs a Timeline Review
One side can grow slower after a hair transplant and still be within normal recovery, especially before month 6. I judge it by timing, scalp health, the original plan, and whether the weaker side is changing month by month.
If the scalp is settled and you can see gradual change, the next step is usually careful observation with consistent photos. If one side remains clearly empty near month 12, or if there is pain, pus, spreading redness, heavy scarring, bleeding after trauma, or a wound problem, the case needs surgeon review. A hair transplant touch up belongs later, after the first result has declared itself.
This worry is understandable because the eyes compare left and right automatically. A close photo can make one temple look like a failure even when the area is still waking up. The useful question is not whether both sides look identical today. It is whether the weaker side is following a normal growth path, or whether the evidence points to poor survival, native hair loss, planning, or healing trouble.
Uneven growth after a hair transplant can be normal, but it should not be answered with empty reassurance. Timing and evidence matter together.
One side growing slower is not always a sign of failure
Not by itself. At 4, 5, 6, or even 7 months, many transplanted hairs are still short, fine, and immature. One side may show new hairs earlier while the other side needs more time before the hairs gain length and thickness.
When I review this concern, density is only one part of the picture. Fine new hairs, skin quality, the day one placement pattern, hair direction, and change from one month to the next all matter. If there are small soft hairs in the weaker area, the concern may be closer to baby hairs after a hair transplant than to a failed transplant.
Growth and coverage are also different. Growth means hairs are coming through. Coverage means those hairs are long enough, thick enough, angled well enough, and placed in a pattern that reduces scalp visibility. A side can be growing and still not give coverage yet.
The concern becomes stronger when the weaker side stays almost unchanged for months, the skin looks unhealthy, or the visible pattern does not match the surgical plan. That is when I start separating delayed growth from a truly failed result or a result judged too early.
Reasons one side can grow slower than the other
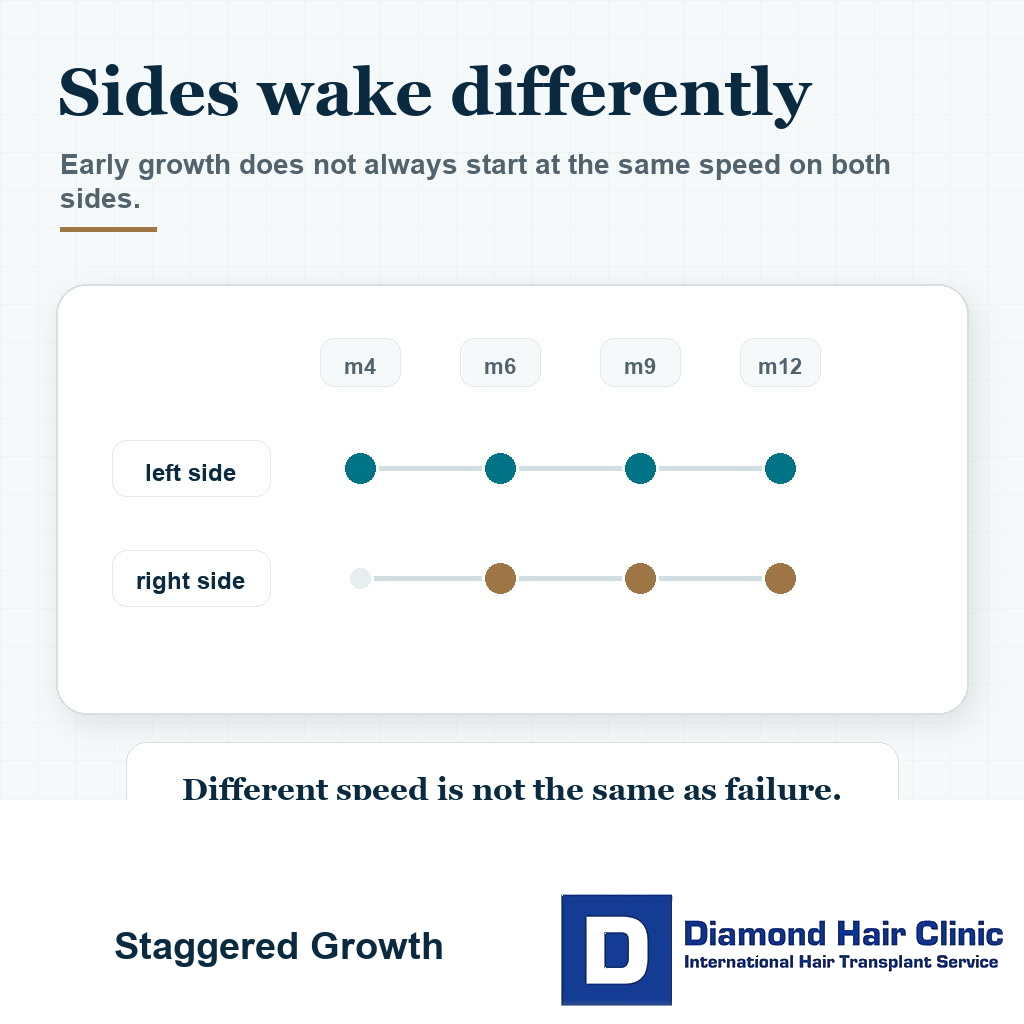
Hair does not return like paint being applied evenly to both sides. Follicles can enter and leave the resting phase at slightly different times, even after careful graft handling. One side may wake earlier, while the other side still has living follicles that are not yet cosmetically useful.
The starting condition also matters. One temple may have had more miniaturized native hair before surgery, more scalp contrast, different hair direction, or a slightly different recession pattern. If the surrounding native hair was weaker on one side, that side can look behind even when transplanted hairs are growing.
Local healing can also differ. Redness, mild swelling, scab behavior, skin thickness, inflammation, and hair direction can make the same number of hairs appear different from right to left. A few millimeters of hair length can change the impression, which is why early left and right inspection can be misleading.
Habits matter too. Combing one side more, touching one temple, photographing from a sharper angle, or checking under harsh bathroom light can make a small delay look dramatic. I try to remove those variables before I judge the surgery.
Early months are too soon to judge uneven growth
Month 2 and month 3 are too early for a serious left and right density verdict. This is the shedding and early recovery period, and many areas look worse before they look better.
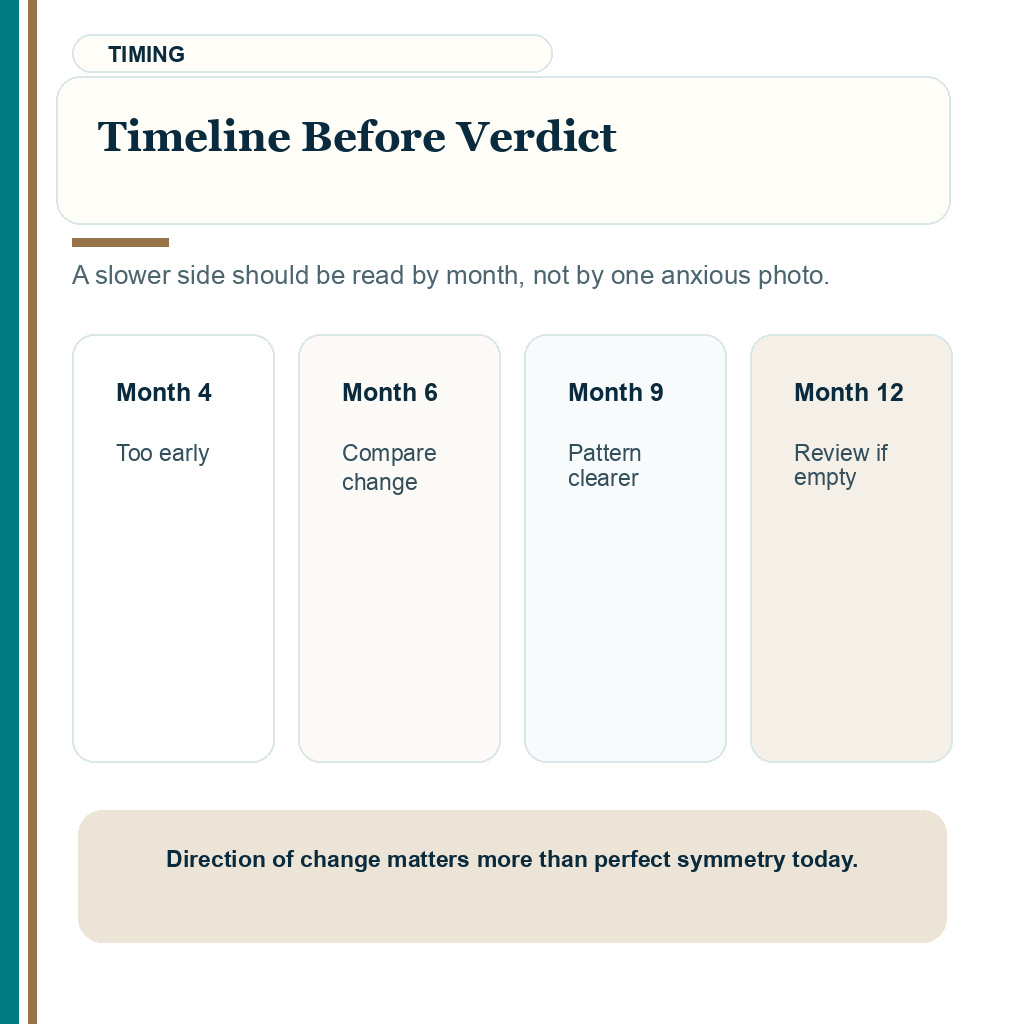
Month 4 is still early. Some new hairs may appear, but coverage is often weak and uneven. This is the reason low density at 4 months after a hair transplant can feel frightening while still being biologically unfinished.
At 6 months, I compare the weaker side with its own month 4 photo, not with the final result the person wants. If it is improving, even slowly, that is useful evidence. Between months 6 and 9, the pattern becomes more meaningful because growth, caliber, and blending should be easier to see.
By 12 months, a clearly empty or poorly changing side deserves a more serious review. Some cases, especially fine hair or slower maturing zones, can continue improving toward 18 months. Waiting does not mean ignoring the problem. It means judging it at the correct biological time.
Compare direction, not perfection. More short hairs, better texture, and less shine than the previous month suggest delayed maturation. The same empty look for many months suggests a different conversation.
These 8 one side growth review slides separate timing, photo variables, warning signs, sleep or trauma context, native hair, the original plan, photo milestones, and touch up timing. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.


Sleeping on one side rarely explains slow growth by itself
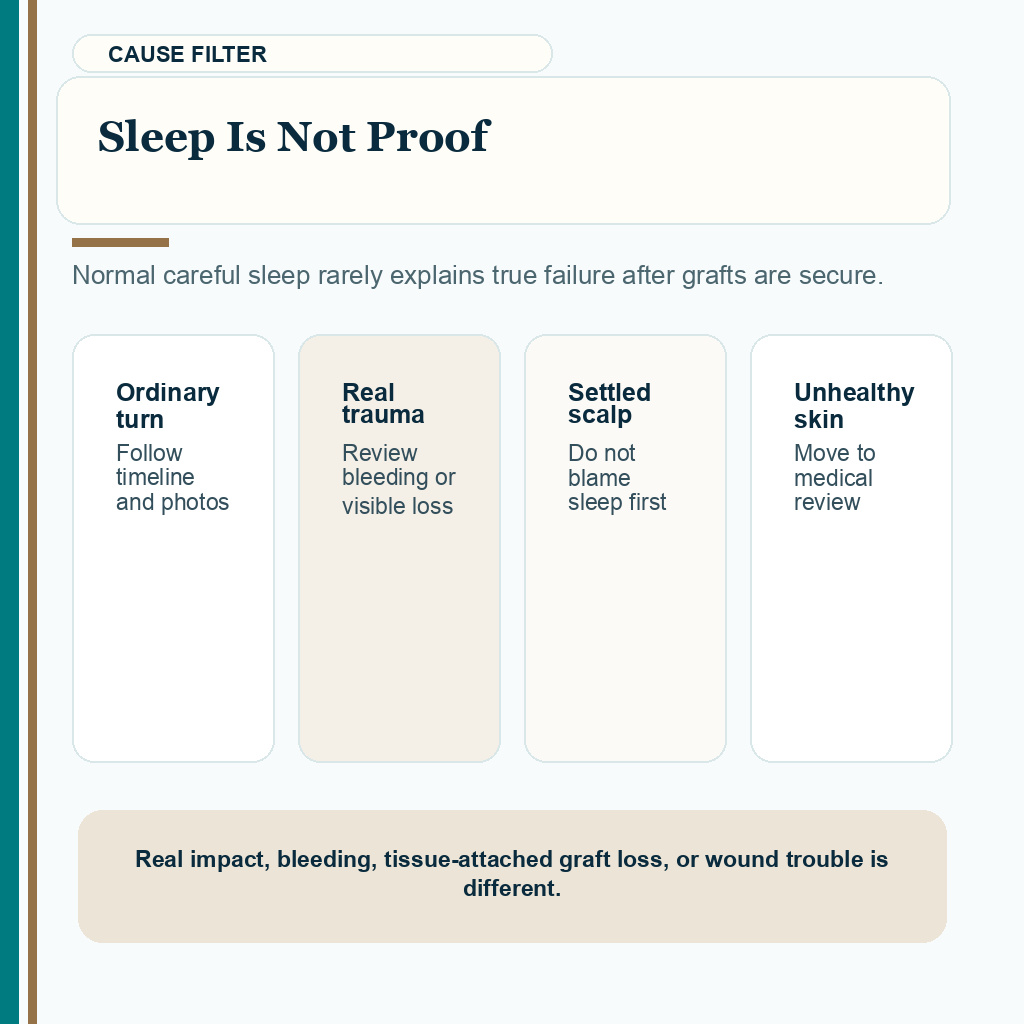
Normal careful sleep rarely explains true failure after grafts are secure. The important protection window is the first 7 to 10 nights, when friction, pressure, scratching, and accidental rubbing matter most.
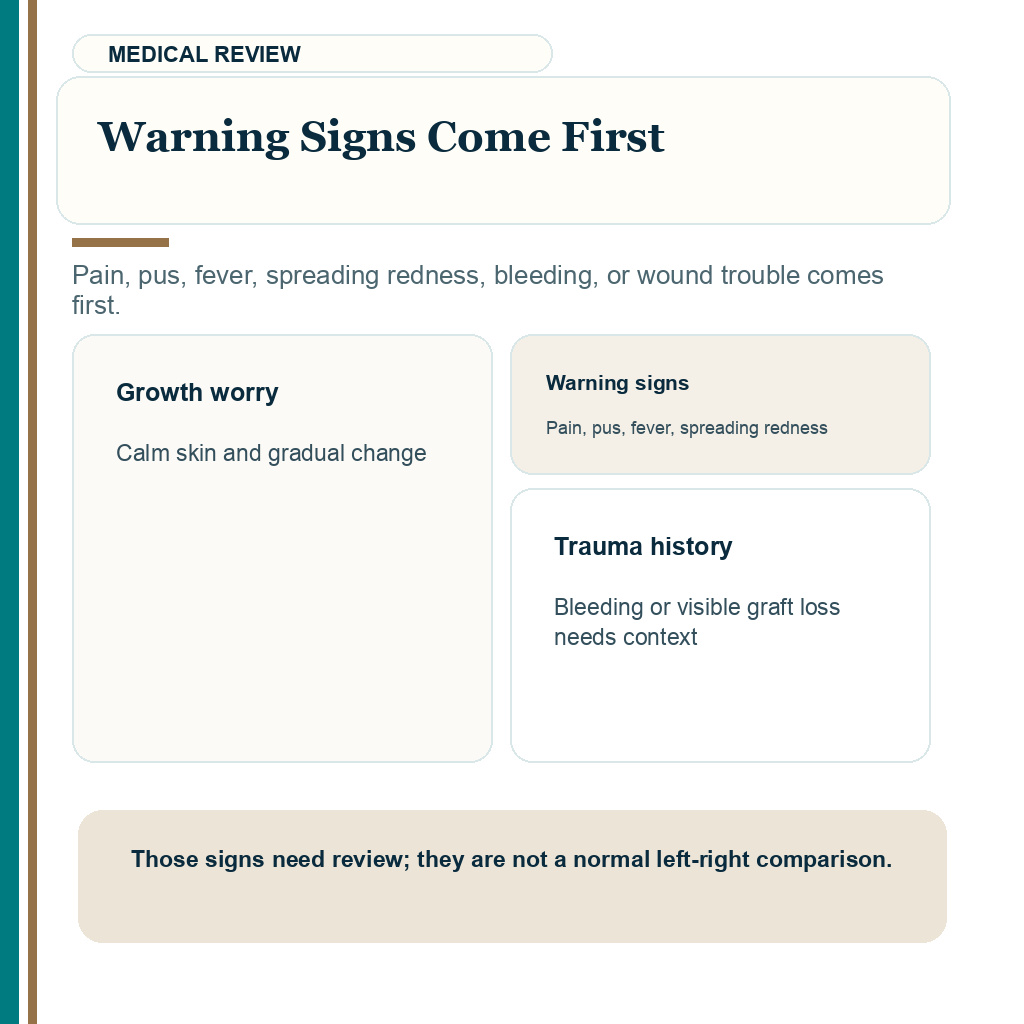
Waking up slightly turned to one side is different from rubbing the recipient area aggressively, hitting it, causing bleeding, or removing grafts with tissue attached. The second situation needs review. The first one usually does not prove graft loss.
Grafts become more secure during the first days. By the end of the early protection window, ordinary light contact is much less likely to remove a graft. Sleep can still affect swelling, redness, or irritation on one side, so the area may look flatter or thinner for a while without meaning that the follicles died.
If there was no bleeding, no visible graft loss, no infection, and the scalp is settling, I do not blame sleep first. I follow the growth timeline and the photo evidence. Clear hair transplant aftercare helps because it teaches the difference between protecting grafts and turning every movement into fear.
Signs that separate slow growth from a real problem
The first sign I assess is change. A slow side with small new hairs, less shine, and better coverage in comparable photos is different from an area that stays empty month after month.
The second sign is scalp health. Settled skin is reassuring. Increasing pain, heat, pus, spreading redness, bleeding after trauma, scarring, skin breakdown, or repeated inflammation changes the priority from growth anxiety to medical review.
Some people confuse shape with growth. One side may look weaker because the hairline was designed with natural irregularity, or because the camera angle exaggerates one corner. That can overlap with an uneven hairline after a hair transplant, where design, swelling, lighting, and growth speed need to be separated.
I also judge by zones, not by emotion. The frontal edge, temple corner, mid frontal density, and transition into native hair can each behave differently. A whole side may feel failed when only one small zone is delayed.
A smooth shiny gap with no visible new hairs late in the timeline needs more attention. It still may not mean immediate repair, but it should not be dismissed with a casual answer.
Native hair can make one side look weaker
Yes. A hair transplant does not freeze the surrounding native hair. If one side had more miniaturized native hair before surgery, that side may shed more, weaken more, or create less coverage during recovery.
I examine the whole scalp, not only the transplanted area. The cosmetic result depends on transplanted grafts and on the native hairs around them. These are not the same biological problem.
Native hair shock loss can make one side look worse for a period of time. If the native hairs were fragile before surgery, they may react more strongly to surgical stress. That finding does not prove the transplanted grafts failed.
Medication may also be part of the discussion, depending on diagnosis and suitability. If miniaturization is active, surgery alone cannot protect every surrounding hair. In selected cases, medications after a hair transplant may help protect native hair around the transplanted area.
The key question is what was transplanted, what was native, and what was already weak. Without that distinction, it is easy to blame the wrong cause.
Surgical planning can explain a weaker side
Sometimes. The two sides may not have started from the same condition. The graft numbers, density distribution, native hair quality, and hairline design may have been different from the beginning. Symmetry in surgery is not always identical arithmetic.
A natural hairline also needs small irregularities. It should not look stamped onto the forehead. This is part of natural hairline design, but it can be mistaken for uneven growth if the patient expects both sides to mirror each other exactly.
There is also the more serious side of planning. Poor graft handling, excessive time outside the body, traumatic placement, wrong angle, overpacking beyond tissue capacity, or inconsistent work between zones can affect survival and appearance.
Surgeon-led planning matters here. The relevant questions are not only how many grafts were promised. They are who designed the plan, who controlled extraction, who created the recipient area incisions, how the grafts were distributed, and whether the donor supply was protected with long-term judgment.
One side can also look weaker when a clinic tried to cover too much with too little. A large area spread thinly may look uneven because the plan was too ambitious from the start.
Day one photos can help review uneven growth
Yes, but they must be read carefully. Day one and scab phase photos cannot prove final growth. They can help show the original placement pattern, density distribution, hairline design, and whether the two sides were planned differently.
If early photos show a balanced plan and one side looks slower at month 5 or month 6, I first think about growth rhythm, native hair shock loss, lighting, hair direction, and normal delay. If early photos already show a clear difference in graft distribution, the later difference may partly reflect the original plan.
Judging hair transplant day one photos is useful only when the photos are treated as context, not as a verdict. A useful set includes day one, two weeks, month 4, month 6, month 9, and month 12 photos taken in similar conditions.
Better photos for reviewing one side growing slower
Good photos reduce false alarms. Take them in the same location, with the same light, the same hair length when possible, the same angles, and dry hair. If every photo is different, comparison becomes almost useless.
Do not judge the weaker side from one flash close-up. Flash, wet hair, overhead bathroom light, and hair pulled apart with fingers can make normal recovery look worse than it is.
For left and right comparison, take front, left angle, right angle, top, and close hairline photos. A monthly comparison is more useful than daily inspection because small changes are difficult to see day by day. If you need a structure, use a monthly comparison rather than repeated panic photos.
Do not press, scratch, or manipulate the recipient area just to expose the comparison. Documentation should help the review, not irritate the scalp.
The right time to ask the clinic to review one side
Ask for clinic review immediately if there is increasing pain, pus, fever, spreading redness, bleeding after trauma, or an obvious wound problem. Those are medical concerns, not normal growth concerns.
If there are no warning signs and you are before month 6, careful observation with consistent photos is often enough. Between months 6 and 9, a structured review becomes more useful if one side is still much weaker. Near month 12, a clearly empty or poorly growing side deserves a proper assessment.
That assessment should include the original plan, graft distribution, donor quality, scalp condition, hair direction, native hair status, and the timeline. A casual opinion from someone who does not know the surgical record is not enough.
This is where who performs the hair transplant surgery becomes important. Months later, a person with a concern needs medical accountability, not only a sales conversation.
When you ask for review, be specific. Send the month, the exact area, comparable photos, and whether the area is changing. That gives the surgeon something useful to interpret.
Safe timing for discussing a touch up or repair
Early touch ups need caution. Operating too soon can spend donor hair unnecessarily, disturb tissue that is still maturing, and make someone chase a result before the first surgery has finished developing.
Repair decisions are usually safer after at least 12 months, and sometimes closer to 18 months if there is continued maturation. This is especially true when fine new hairs are present and the scalp looks healthy.
If a correction is needed, it should be precise. A weak side should not be filled blindly with a large graft number. First we need to know why it is weak. Low survival, poor hairline design, ongoing native hair loss, and limited donor planning are different problems.
Some people ask whether they need a second hair transplant because one side looks thinner. My answer depends on donor capacity, future hair loss, the first surgical record, scalp quality, and the realistic cosmetic gain.
Before any correction, I examine the donor area. A request for 500 or 1,000 more grafts may sound small, but donor supply is limited. When the first surgery has created a real structural problem, bad hair transplant repair may be part of the discussion. The decision still has to come from examination, donor reserve, and the likely cosmetic gain, not from frustration in a difficult month.
The best way to judge whether uneven growth is normal
Separate timing from evidence. Before month 6, uneven growth is often part of recovery. Between months 6 and 9, the pattern becomes more meaningful. Around 12 to 18 months, the result can be judged much more fairly.
Do not ignore the scalp while waiting. Calm skin, gradual improvement, and small new hairs are reassuring. Pain, infection signs, thick scarring, or a side that remains unchanged for many months deserves surgeon review.
The next step is not to stare harder. Take consistent photos, protect the scalp, follow your surgeon’s instructions, and review the change at the right time.
Perfect symmetry at every stage is not the standard I use. I want to see a natural, stable result when the transplant has truly matured, with the donor area protected in case more planning is needed later.