


Lowering a Naturally High Forehead With Hair Transplant
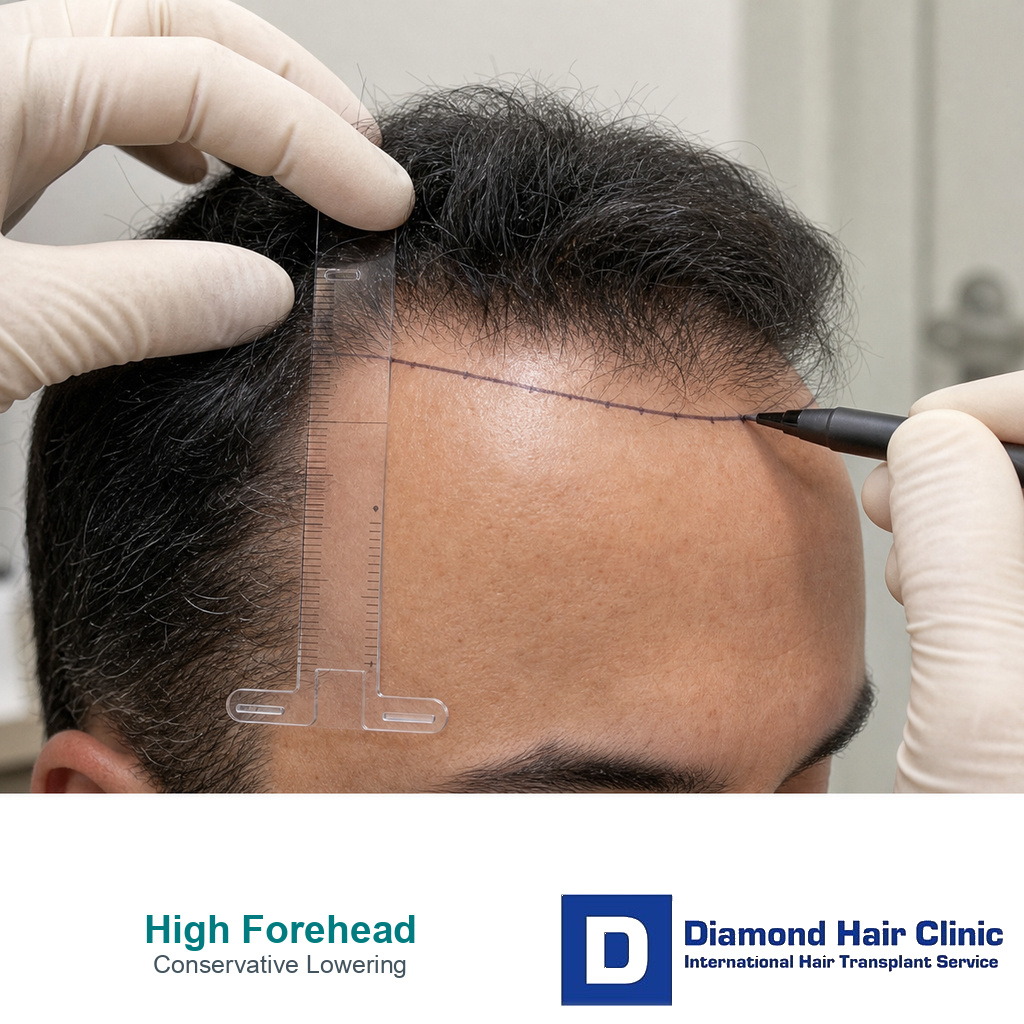
A hair transplant can lower a naturally high forehead in specific cases, but it needs careful planning, not aggressive lowering. Even 1 to 2 centimeters can change the face more than patients expect. When I plan this type of case, I am not trying to draw the lowest possible line. I am checking whether the new hairline will look natural, age well, and protect the donor area for the future. That includes checking where FUE should stop around the forehead muscle before the line is lowered.
This is different from a widow’s peak hair transplant, where the central V shape may need to be preserved rather than lowered away.
A naturally high forehead is not always a hair loss problem. Some patients were born with a high hairline. Others have recession, traction alopecia, temple loss, or early thinning that only looks like a naturally high forehead. A stable high forehead and a receding hairline can look similar in photos, but they are not the same surgical problem.
For this type of case, the result should look as if the hairline could have always belonged to the patient. That means careful hairline design, correct angle, soft irregularity, donor protection, and clear limits.
Naturally high forehead and hair loss are different problems
A naturally high forehead means the patient’s frontal hairline has always sat higher. Hair loss means the hairline has moved backward, thinned, or changed shape over time. These are not the same problem.

Old photos are very useful here. Childhood photos, teenage photos, and photos before thinning can show whether the hairline was always high or whether recession changed the face.
If the issue is a true receding hairline, ongoing hair loss and future planning become central. If the issue is a stable high forehead, the decision is more cosmetic, but it still uses permanent donor grafts.
Safe lowering depends on facial balance
There is no safe universal number. In many cosmetic lowering cases, 1 to 2 centimeters can already be a large facial change. A patient may think 1 centimeter sounds small on a ruler, but on the hairline it changes surface area, graft demand, density, and temple balance. More than that may be possible in some patients, but it should never be promised from a photo alone.
The safe amount depends on forehead height, facial proportions, temple support, hair caliber, donor density, skin quality, age, sex, and future hair loss risk. A line that looks attractive in a drawing can look artificial once real hair grows through the skin.
A modest lowering that still belongs to the face is often safer than a low line that looks exciting for a few months but unnatural for years.
Use the 8 forehead lowering design slides below to separate facial proportion, donor budget, graft direction, density realism, temple relation, procedure choice, future hair loss, and surgeon-led planning. Swipe sideways, use the arrows, or choose a number below the image.
A lower hairline can still look unnatural
A lower hairline can look unnatural when it is too straight, too dense at the front, too low for the face, or disconnected from the temples. A transplant should not create a hard border between forehead and scalp.
The first rows need softness. In most patients, that means fine single hair grafts, careful spacing, correct angle, and a gradual transition rather than a hard border. A low hairline with thick grafts can look more artificial than a slightly higher hairline with a natural transition.
A celebrity hairline or filtered photo is not a surgical plan. The design must fit the patient’s own face, not somebody else’s forehead.
Examination points before accepting this case
The examination has to separate a stable high hairline from recession, miniaturization, traction loss, weak donor supply, poor temple support, and unrealistic expectations about future aging.
The forehead skin and eyebrow movement also matter. A hairline should not be placed too low into mobile forehead skin just because the patient wants the shortest possible forehead. Hair must grow from a zone where the angle, skin behavior, and facial movement can still look natural.
A proper consultation is not only about drawing a line. The issue is deciding whether that line can survive real life, styling, lighting, aging, and future hair loss.
Forehead lowering surgery is a different decision
Forehead reduction surgery and hair transplantation are different procedures. Forehead reduction moves the hair bearing scalp forward and leaves a surgical scar along the hairline. A transplant places individual follicles to create or soften a lower hairline.
Some patients may be better suited to forehead reduction surgery, some to FUE hair transplant, and some should avoid aggressive lowering altogether.
The choice is practical. Forehead reduction can move the hair bearing scalp forward in one operation, but it depends on scalp laxity, scar tolerance, and the patient accepting a surgical incision at the hairline. A transplant builds the lower line with grafts, so it depends on donor supply, graft density, hair caliber, skin quality, and whether the first rows can look soft enough at close range.
With transplant surgery, grafts can soften, lower, and reshape the visible line. They cannot ignore facial proportion, donor supply, or the quality of the skin receiving them.
Women and men need different planning
Female and male hairlines often differ in shape, temple closure, styling habits, density expectations, and future hair loss risk. A feminine hairline goal can be reasonable, but it still has to respect donor limits and tissue quality.
In some women, the purpose is to reduce a naturally long forehead while preserving a soft rounded frame. In men, lowering too much can create a hairline that does not age well, especially if male pattern hair loss develops later.
The discussion of female hairline hair transplant explains why feminine framing needs its own planning rather than simply lowering the central point.
For transgender women, the question may include facial feminization goals as well as donor limits and temple design. This should not be approached like a standard male recession repair. This is the practical point in feminine hairline planning.
Donor management still matters in a cosmetic case
Cosmetic lowering can feel smaller than baldness reconstruction, but it still spends grafts permanently. If a patient develops hair loss later, the donor area must still have reserve.
The donor area is not unlimited. A low hairline can consume many grafts because the new edge must be dense enough to look natural. A weak, see through edge in the front can look worse than a naturally high but stable hairline.
The graft cost of lowering should be calculated before the plan is accepted. A cosmetic improvement today should not make future hair loss harder to treat, especially because lifetime graft supply is limited.
Temple points can decide whether the result looks natural
Lowering only the middle of the hairline can shorten the forehead, but it may leave the sides looking disconnected. The temples and temporal points help frame the face, and they influence whether a lower central line looks natural.
If temple support is weak, a very low central line may be unsafe. This can feel conservative to a patient, but it protects the natural shape of the whole frame.
Temple point hair transplant is one of the most delicate parts of facial framing because the angle is flat, the density is subtle, and mistakes are easy to see.
Density has to be planned carefully
In a high forehead case, the new hairline often sits in a very visible area with no existing hair in front of it. That means the first rows must look natural from close range.
Too little density can create a thin edge. Too much density can create a wall. Thick grafts in the first rows can make the line obvious. The safer plan creates softness at the very front, then enough density behind it to make the new height look intentional rather than drawn on.
A lower line may require more grafts than patients expect. The lower the design, the wider the new area becomes, and the more careful the density plan must be.
Too low can become unnatural
Too low is not one measurement. It depends on the face, age, temple support, hair characteristics, forehead movement, and future hair loss risk. A hairline that looks attractive at 25 may look strange at 45.
The design has to fit the future face, not only the current mirror. A natural mature hairline often ages better than an aggressively low one.
If the requested line resembles the low and flat hairlines that can make hair transplants look artificial, it is safer to say no than to create a result that the patient may later regret.
Future hair loss can change the decision
Future hair loss can change the decision completely. A patient with a naturally high but stable hairline may be a different candidate from a patient whose temples are quietly thinning.
If the hairline is lowered aggressively and the native hair behind it later thins, the patient may be left with a strong front edge and weak hair behind it. That can look more artificial than the original high forehead.
Family history, miniaturization, medication tolerance, and age all matter. A hairline should not only solve today’s mirror concern. It should also survive the next stage of the patient’s hair loss pattern.
Later lowering should be planned cautiously
Sometimes yes, and this is often safer than trying to do too much in one operation. A modest first design can be assessed after growth. If the patient still wants a slightly lower line and the donor area remains safe, a second small refinement may be possible.
The opposite is much harder. A hairline that was placed too low may require graft removal, camouflage, or acceptance of a design that does not age well. Lowering later is usually easier than trying to raise an unnatural line.
The logic is similar to a hair transplant touch up. This is not only about whether another procedure can be done. The practical issue is whether a slightly lower line improves the face enough to justify spending more donor hair.
Edited photos can mislead patients
Edited photos can make a lower hairline look easy because they show a line, not a living transplant. Real hair has angle, density, caliber, growth direction, and texture. It also has to move with the face and blend with the temples.
A drawn line does not show how many grafts will be needed, whether the first rows will look soft, or whether the donor area can support the plan. It also does not show whether the patient will still like that line as the face ages.
Photos help clarify the patient’s goal, but a photo edit should not replace surgical judgment.
Some patients are poor candidates for lowering
Lowering is a poor choice when the requested line is too low, too flat, too dense for the donor, unsupported by the temples, or based on a photo that does not match the patient’s anatomy.
Lowering should also be refused when active hair loss needs diagnosis first. In some patients, what looks like a high forehead is actually early thinning, traction loss, or recession. Those cases need different planning.
If the history suggests pulling hairstyles or frontal loss, traction alopecia hair transplant planning should be considered before treating the case as purely cosmetic.
Facial balance comes before lowering
Facial balance includes forehead height, facial thirds, brow position, temple width, hair caliber, head shape, and the way the patient normally styles the hair. The consultation should also ask whether the concern is visible in normal life or only in one camera angle.
Planning from photos can help, but it has limits. For hair transplant planning from photos, a final design should still be confirmed with proper examination.
In a high forehead case, millimeters matter. A slight change can improve balance, while an aggressive change can make the face look less natural.
Sometimes no surgery is the better recommendation
Sometimes surgery is not worth it. A naturally high forehead is not a disease. If the forehead is high but balanced, if donor reserve is weak, if expectations are unrealistic, or if future loss risk is high, no surgery may protect the patient.
Saying no is not a failure of treatment. It is part of responsible surgery. A cosmetic operation should improve the face without creating a long term maintenance problem.
A careful no may disappoint a patient in the consultation. An enthusiastic yes can harm the same patient for years.
A good result keeps the forehead in proportion
The right result looks like it could have always belonged to the patient. That means softness, irregularity, correct angle, suitable height, and a design that does not fight the temples.
The result should look natural with different hairstyles, not only with the hair combed forward. It should also remain reasonable as the patient ages.
High forehead planning has to consider whether a hair transplant will still look natural as the patient gets older. The best design is not only flattering today. It is still acceptable later.
Useful consultation materials help the planning
Bring old photos, current photos with the hair pulled back, photos under normal light, and a clear explanation of what bothers you. If you have family hair loss, mention it. If you have used medication, mention that too.
I still ask patients to show the lowest line they imagine, even if I may not accept it. This helps me understand the emotional goal, then translate it into a safer surgical plan.
A hair transplant can lower a naturally high forehead, but the strongest result is not the lowest line. It is the line that looks natural, protects donor hair, and still belongs to the face years later.