Transgender Hair Transplant for a Feminine Hairline
A hair transplant can help a transgender woman create a softer, more feminine hairline, but only if the plan is made around her face and future hair loss, not around a generic graft number. It works best when the main issue is recession, temple shape, or a high but transplantable frontal line.
If the main concern is forehead height, brow position, or planned facial feminization surgery, I clarify the sequence before any grafts are placed. A safer result comes from matching the hairline shape to the face, protecting the donor area, and planning around hormone history, future hair loss, and density limits. If a clinic treats this like a standard masculine hairline restoration, the plan is not personal enough.
Moving hair is only one part of the decision. The decision depends on whether the new hairline will make the face feel softer in a natural way, age well, and still leave enough donor capacity for the future.
A transgender hair transplant needs different hairline planning
A transgender hair transplant often has a different artistic goal from a typical male pattern hair transplant. In many male hairline restorations, the plan is to rebuild recession while keeping a mature, slightly angular, age appropriate frame. In a transgender woman, the goal may be to soften the upper face, reduce the visible M shape, round the temples, and create a hairline that supports a feminine appearance.
Some patients search for this as an MTF hair transplant or a hairline feminization hair transplant. I understand those terms, but in the consultation I bring the conversation back to the person in front of me. What should this hairline do for her face? How soft should the temples be? How much donor hair can be used without creating a future problem?
I do not think of it as just adding more grafts. I think of it as hairline design with a very specific facial goal. The direction of the hair, the use of fine single hairs at the front, the transition into the temples, and the height of the central hairline all matter.
A straight, dense, heavy border can look artificial even if many grafts grow. In this type of case, the unsafe part is not only a thin result. The unsafe part is a result that technically grows but still feels wrong to the patient because the outline remains too masculine or too harsh.
For me, the consultation has to begin with the patient’s actual goal. Some transgender women want to correct recession. Some want a softer frame for the face. Some are deciding between a female hairline transplant, hairline lowering surgery, or a combined facial plan. These choices can sound similar online, but surgically they are very different.
A hair transplant is not always enough when forehead shape also matters
Hair transplant may be enough when the main problem is recession at the temples, a high but reasonable frontal line, or a hairline shape that can be softened with grafts. It may not be enough when the forehead height, brow bone, or broader facial structure is the main concern. When that happens, facial feminization surgery or hairline lowering may need to be discussed before the transplant sequence is decided.
Here is the practical difference. A hair transplant creates a hair bearing outline by moving follicles. Hairline lowering or forehead surgery can change the position of the scalp, forehead, or upper facial frame. A graft can soften an outline, but it cannot move the brow bone or physically shorten the forehead by itself. If those procedures are planned later, a transplant designed too early may place grafts in an area that no longer fits the final anatomy.
Timing matters. If a patient is planning forehead surgery or hairline advancement, I need to know that before I design a transplant. A hairline that looks well planned before facial surgery may not be ideal after the forehead position or scalp position changes.
Hairline distress can be real and heavy. Still, rushing grafts into the wrong place can make a later correction harder, especially if forehead surgery changes the position of the scalp or the frame of the upper face.
When the patient mainly has a naturally high forehead, the discussion is closer to lowering a naturally high forehead. When the patient has true recession from androgenetic hair loss, the plan must also include the pattern of loss and the donor reserve. When FFS is planned, the hairline should be part of the wider facial plan, not a separate quick fix.
Sequence hair transplant with facial feminization surgery carefully
If facial feminization surgery may include forehead contouring, brow work, hairline advancement, or scalp movement, I usually want that plan clarified before grafts are placed. The sequence matters. A transplant fixes follicles into the skin, and facial surgery may later change the forehead frame, the scalp position, the scar position, or the shape that the new hairline needs to support.
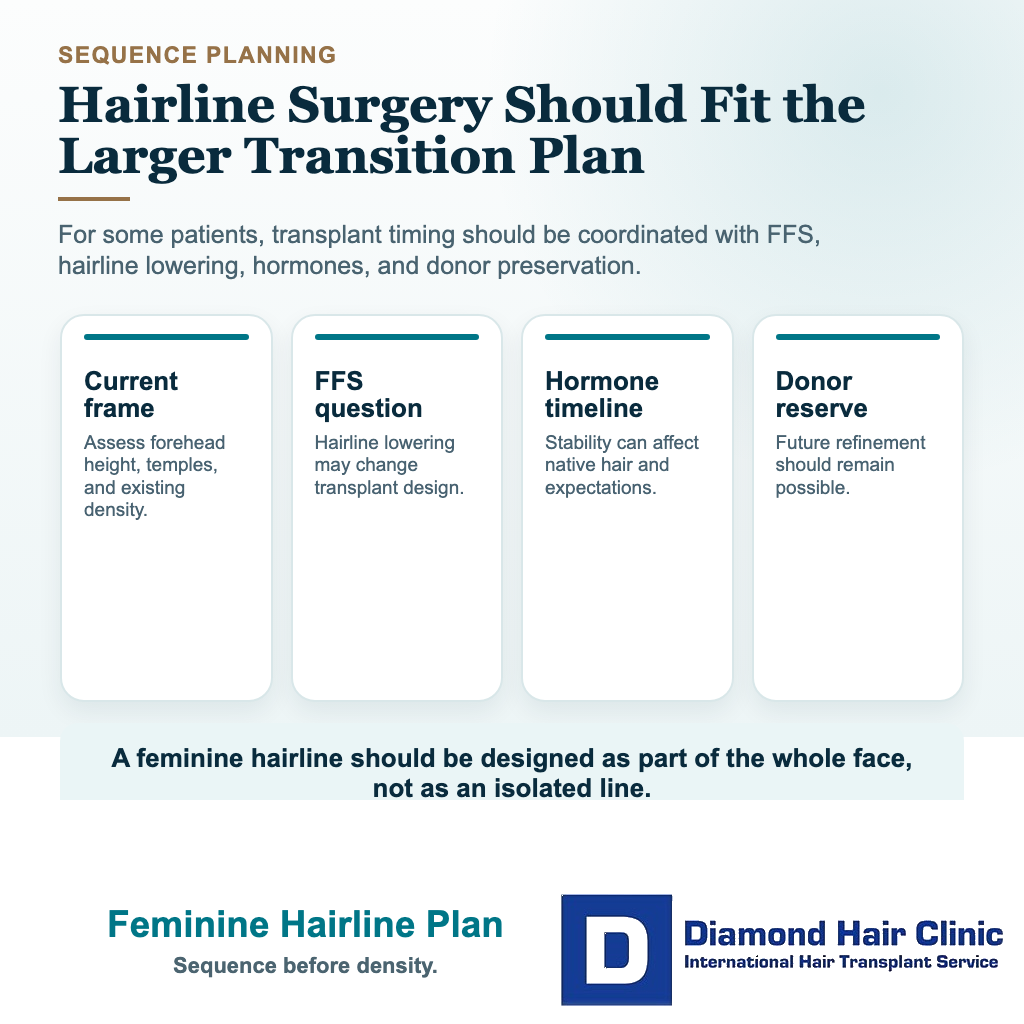
Sometimes the better sequence is facial surgery first, then hair transplant later to soften a scar, refine the temples, close small gaps, or add density once the facial frame has settled. In other patients, a transplant can come first if no forehead or scalp advancement is planned and the main problem is recession, temple shape, or a high but stable hairline.
Bring any FFS plan, surgeon notes, photos, and expected hairline advancement details to the hair transplant consultation. This avoids designing one hairline for today and needing a different one after facial surgery. That is not a delay tactic. It is a way to use donor grafts once, in the position most likely to remain correct.
Choosing the right feminine hairline shape
I start by looking at the whole face, not only the empty corners. The forehead height, temple shape, eyebrow position, frontal hair direction, age, hair caliber, and existing hair density all change the plan. A feminine hairline is often softer and more rounded, but it should not be copied from another person’s photo.
The most common mistake is drawing the line too low or too flat. A low line can look attractive on a screen before surgery, but it may not age naturally. It can also consume too many grafts in the front and leave fewer grafts for future thinning.
I pay special attention to the temple area. It can change facial framing a lot, but it is also unforgiving. If the angle, direction, or density is wrong, the result can look planted. A soft feminine outline needs gradual transition, not a hard border.
The better hairline is usually the one that looks natural and sustainable, not simply the lowest possible position. The plan should help the patient feel more aligned with herself without creating a new surgical problem later.
Donor management still matters after transition
A hair transplant does not create new hair. It moves follicles from the donor area to the recipient area. Donor management still matters in every transgender hair transplant.
Some patients have strong donor hair and limited recession. Others have a history of male pattern hair loss with thinning that may involve the crown, middle scalp, or donor margins. I cannot ignore that history just because the goal is feminine hairline design.
Hormone therapy and medical treatment may change the future hair loss picture for some patients, but I do not treat them as a guarantee. I still examine the donor area, the miniaturization pattern, the family history, and the stability of the hair loss before I decide how much can be safely moved.
The donor area is a lifetime resource. If too many grafts are used to force a very low hairline in one session, the patient may have fewer options later. This matters even more when the hairline carries emotional importance, because a repair after a poor design can be more difficult than doing the first plan conservatively.
Hormone therapy can change the surgical plan
Hormone therapy can be relevant to the surgical plan, but it does not replace a proper scalp examination. Not every transgender woman is on the same hormone plan, and not every hairline responds in the same way. Feminizing hormone therapy and anti androgen treatment may slow androgen driven hair loss in some patients, and in some cases the hair may look stronger with time.
But I do not treat hormone therapy as a surgical guarantee. It may not fully rebuild temple recession, it may not solve a naturally high forehead, and it does not make donor planning unnecessary. The safer approach is to look at the scalp as it is now, understand the medical plan, and decide whether surgery should happen now, later, or in a smaller first stage.
If the hair loss pattern is still changing quickly, the plan needs more caution. If the donor area is strong and the hairline goal is realistic, the plan may be more straightforward. If there is diffuse thinning or uncertainty about future loss, I may recommend waiting, medical coordination, or a more limited first session.
I check the difference between a receding hairline and a naturally high hairline. These two problems can look similar in the mirror, but they are not the same surgically. A patient with active recession needs future planning. A patient with stable high forehead anatomy may need a different design conversation.
For patients already working with an endocrinologist or gender affirming medical team, the hair transplant plan needs to be medically coherent. It should support the patient’s overall medical plan, not create confusion around timing, medication, or future procedures.
Use the 10 feminine hairline planning slides below to connect hairline shape, FFS timing, hormone context, donor reserve, density limits, and respectful surgical planning. Swipe the carousel, use the arrows for one step at a time, or choose a number below the image to jump to that point.