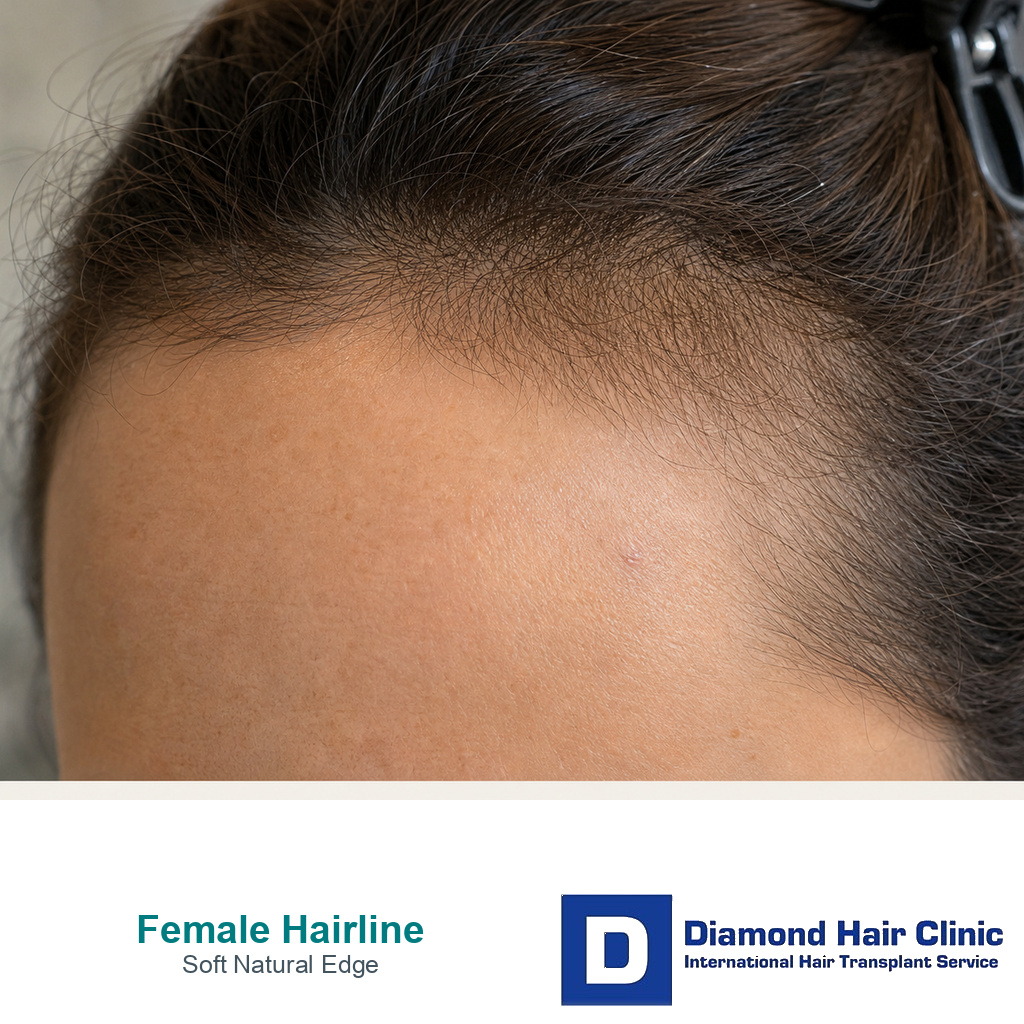
Female Hairline Softness and Natural Design
Women can have a natural hairline transplant, but only when the diagnosis, donor area, and design are right. A female hairline transplant is not just a smaller version of a male hairline transplant. The result should be compared with a result from hair like yours, especially when density, parting pattern, temple shape, and long term loss pattern are different from a typical male hairline case. The goal is softer facial framing, not a sharp border or the lowest possible line. In women after menopause, the hairline plan should also be judged against the wider diagnosis described in menopause hair loss before hair transplant surgery.
I first ask why the hairline looks thin, high, or recessed, not how many grafts can be placed. A woman with a naturally high forehead may be a good surgical candidate. A woman with diffuse thinning, active shedding, PCOS related hormonal hair loss, or a weak donor area may need medical evaluation first.
The decision has to be careful. Female hairline surgery can be very rewarding, but it should be conservative, personal, and diagnosis led. I look at whether we are softening the frame, lowering a naturally high forehead, or rebuilding hair that was actually lost, because those are not the same operation.
Female and male hairline planning are different
I plan it differently. A typical female hairline is usually softer, rounder, and more dependent on temple balance than a typical male pattern hairline. The edge should not look like a hard wall of grafts.
Natural hairline design matters deeply in women because the hairline is part of facial expression. It affects how the forehead, eyebrows, temples, and cheekbones are seen together. A line that looks strong in a drawing can look heavy in real life.
One female template does not work for every patient. Some women need a lower central line, some need corner softening, and some need temple support more than lowering. A feminine result comes from proportion and direction, not from simply moving the whole border down.
I watch how the patient wears her hair. A woman who ties her hair back, parts it in the middle, or stands under bright light will notice details that a standard front photo may hide.
Diagnosis comes before female hairline surgery
Diagnosis comes first because women can lose hair for several different reasons. Some have a naturally high forehead. Some have traction damage from years of tight hairstyles. Some have hair pulling related hair loss. Some have female pattern hair loss. Some have telogen shedding, iron deficiency, thyroid problems, postpartum changes, or medication related shedding.
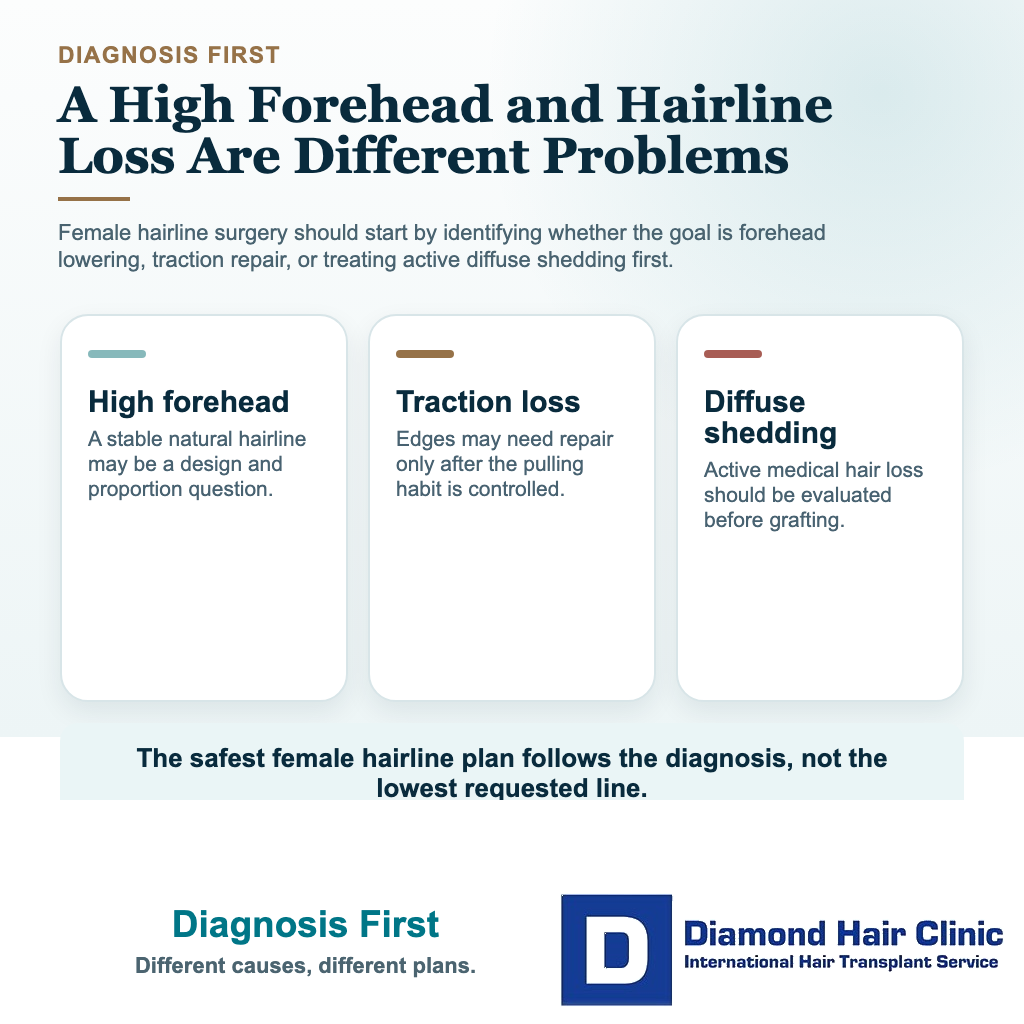
Scarring conditions such as frontal fibrosing alopecia also have to be considered, especially when frontal recession appears with eyebrow thinning, scalp redness, itching, or loss of follicular openings. That is not the same decision as lowering a naturally high forehead.
If I treat all of these as the same problem, I may create the wrong plan. Being a good candidate for a hair transplant means the donor area is safe, the cause is understood, and surgery is likely to solve the right problem.
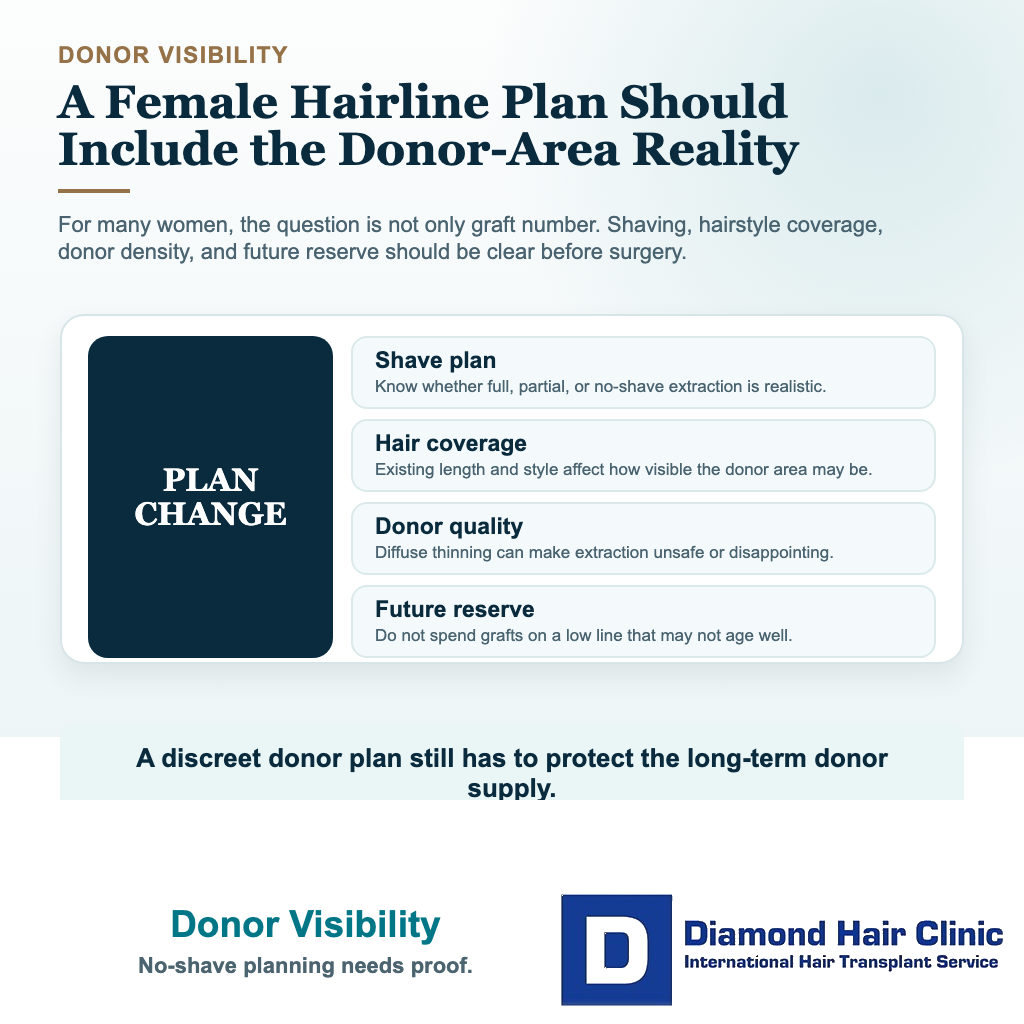
Diffuse thinning needs careful donor review before hairline planning. If the donor area is also miniaturizing, transplanted hair may not behave like a permanent solution. Then, surgery may be technically possible but strategically unwise.
Lowering a naturally high female forehead
A hair transplant can lower a naturally high female forehead in specific cases. The safest candidates usually have a stable hairline, good donor density, no active diffuse loss, and realistic expectations about density and growth time.
A hair transplant for a naturally high forehead must be measured carefully. Lowering the line too far can make the forehead look shorter, but it can also make the result look artificial, dense at the edge and thin behind it, or too heavy for the face.
The line cannot be designed from the patient’s wish alone. I design it from the face, the existing hair, the donor supply, the forehead muscles, the temple shape, and how the result should age.
I also separate lowering the whole frontal line from softening corners or rounding the frame. A small change in the wrong direction can make the face look less natural, not more balanced.
Hair transplant versus forehead reduction surgery
Forehead reduction surgery moves the scalp forward by removing forehead skin. A hair transplant places follicular units into the forehead area to create a new hairline over time. These are very different decisions.
Forehead reduction can create an immediate lowering effect, but it involves an incision along the hairline and depends on scalp laxity. A transplant avoids that kind of linear frontal incision, but the result grows gradually and may need enough grafts to create a soft transition.
Some women are attracted to dramatic lowering because it seems faster. I understand that feeling, but aggressive lowering can create a new problem. If the front is lowered too much without enough density behind it, the result may still look unnatural. Sometimes the most natural improvement is a moderate transplant plan, not the most aggressive lowering.
Donor shaving and visibility
For many women, donor trimming is one of the most practical concerns. In many FUE cases, at least part of the donor area needs to be trimmed so the grafts can be removed safely and accurately. Some women can hide a limited shaved zone under longer hair, but this depends on donor density, hairstyle, graft number, and how the hair is normally worn.
This discussion should not wait until the day of surgery. If a woman needs to return to work quickly or cannot accept visible donor trimming, the plan must be realistic from the beginning. A smaller session, a concealed donor shave, or delaying surgery may be better than surprising the patient with a change she was not emotionally prepared for.
The donor area is not only a technical zone. It is part of the patient’s daily appearance. The surgical plan should include how the donor will look during the first weeks, not only how the hairline may look after full growth.
Use the 10 female hairline planning slides below to review diagnosis, donor visibility, softness, temple balance, and restraint before judging a design. Swipe the carousel, use the arrows for one step at a time, or choose a number below the image to jump to that point.