Where Should Hairline Lowering Stop With FUE?
FUE hairline lowering should stop before the new edge is forced into lower forehead skin that moves strongly when you raise your eyebrows. That sounds simple, but it is one of the easiest design mistakes to miss in consultation. A low line can look attractive in a still photograph, then look artificial once the face is animated. If a patient is asking for a sharp lower border, I compare the request with low straight hairline planning before final approval.
Drawing a lower line is not enough. The harder test is whether it still behaves like scalp that naturally carries hair when the eyebrows lift, the forehead wrinkles, the temples are seen from the side, and future hair loss changes the hair behind it.
The stopping point is a surgical judgment, not a ruler measurement. I use the frontalis movement, donor reserve, hair caliber, age, native pattern, and temple shape together. If one of those points argues against more lowering, the safer line is often the one that looks slightly higher on drawing day and more natural in real life.
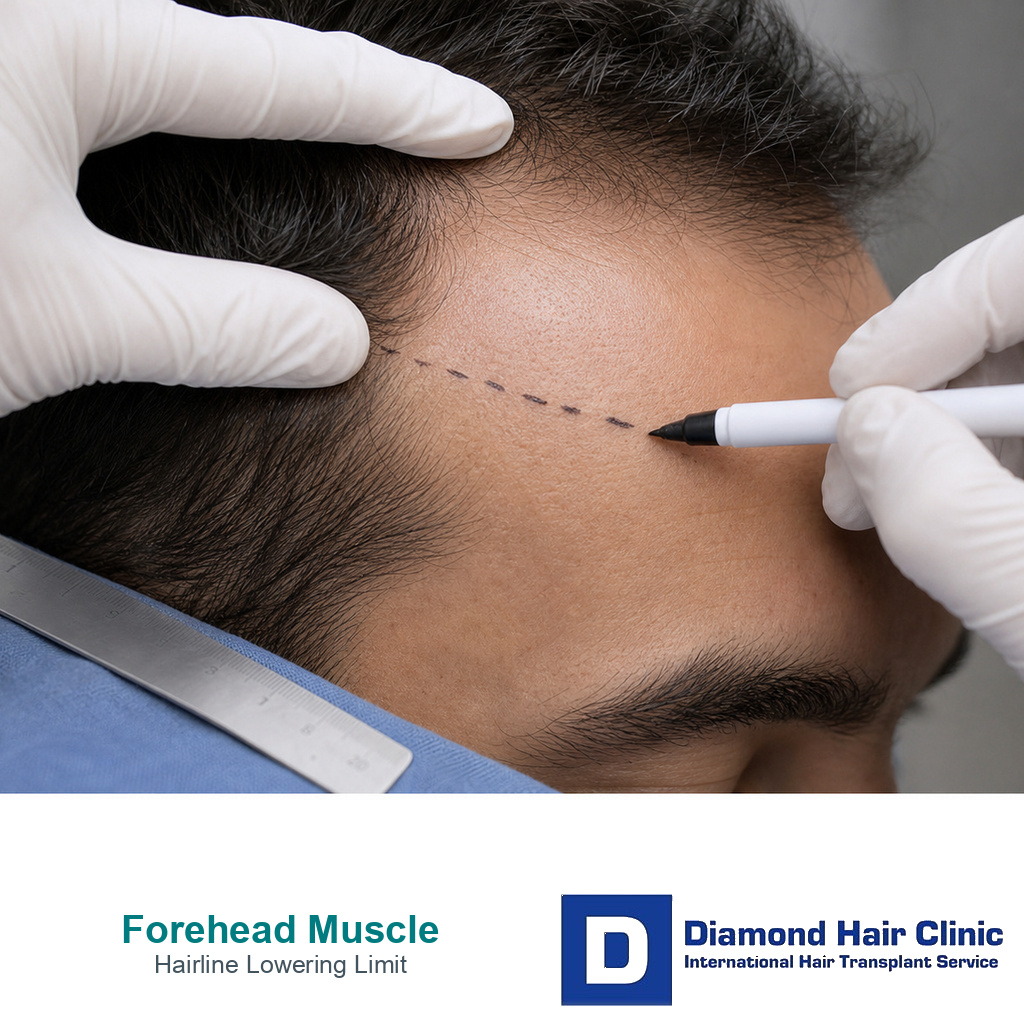
Forehead muscle is a moving boundary
The frontalis muscle helps lift the eyebrows and produces horizontal forehead lines. For hairline lowering, that movement gives useful information because it shows where the lower forehead is behaving like expressive facial skin rather than stable scalp. It is not a perfect border, and it is not identical in every patient, but it is a clinical warning zone.
When I assess hairline design in a hair transplant, I ask the patient to relax the face first. Then I ask for eyebrow elevation. I look at the depth and position of the forehead lines, the amount of skin movement, the natural temple transition, and the original direction of hair growth. A proposed hairline that drops into skin that folds and lifts strongly deserves caution.
Grafts may grow in lower forehead skin, but growth is not the only question. The visual behavior matters. If the transplanted edge is placed too far below the natural scalp zone, it can seem to move with the forehead. The same hairline may look acceptable in a clinic mirror and still feel strange when the patient speaks, smiles, frowns, or raises the brows.
High forehead lowering is not the same as forehead reduction surgery
FUE can lower the visible hairline in selected patients with a naturally high forehead. It does this by moving follicles from the donor area into a newly designed frontal zone. It does not remove forehead skin, advance the scalp surgically, change the frontalis muscle, or stop expression movement.
This difference matters when someone asks about lowering a naturally high forehead with a hair transplant. Some patients have a stable high hairline with good density behind it. Others have recession, open corners, early diffuse thinning, weak temples, or a family pattern that is still unfolding. Those situations should not receive the same line. The same consultation should first separate a mature hairline from a receding hairline so the request for lowering is not treated as automatically surgical.
If the donor area is strong, the pattern is stable, and the face can support it, modest lowering may improve facial framing. If the patient is young, the corners are actively changing, or the crown and middle scalp may need grafts later, an aggressive low design can spend grafts that would be better preserved. A lower hairline can become the wrong hairline when it spends the future graft budget.
Lowering boundary lens
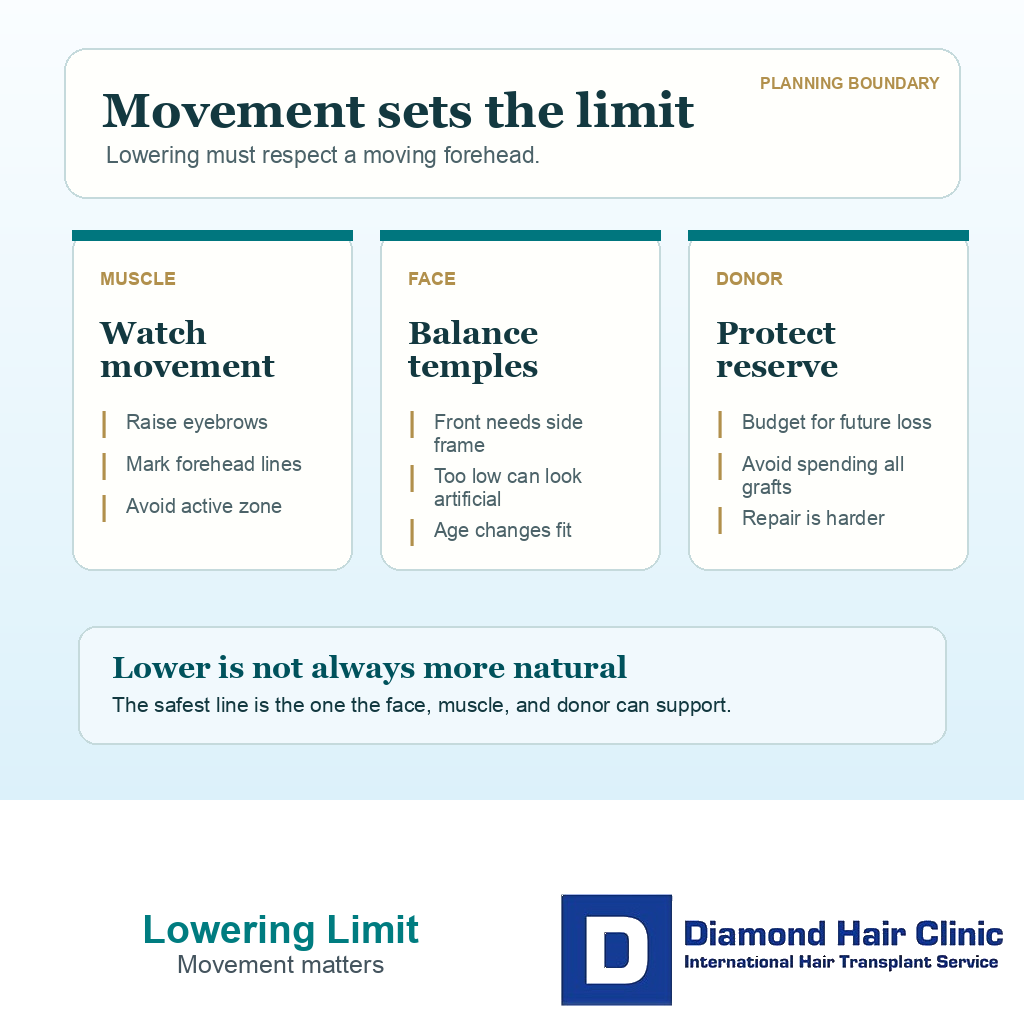
Four limits before lowering a hairline further
A lower hairline has to pass more than a mirror drawing. Forehead movement, donor reserve, temple fit, and repair difficulty all shape the safe stopping zone.
Forehead movement
Does the line enter moving forehead skin?
The frontalis muscle can make a very low line look unnatural when the eyebrows lift or the forehead wrinkles.
A line that sits too low can move with forehead skin. That can make the result look less like natural scalp hair in expression.
Use this as a planning frame, not a diagnosis or approval for surgery. The final plan still depends on donor reserve, recipient area anatomy, hair type, medical history, and future hair loss risk.
I decide the practical stopping zone
I begin with the relaxed face because the relaxed frame is what most people notice in ordinary conversation. Then I test the raised eyebrow view because excessive lowering often reveals itself there. I am looking for a line that remains natural in both states, not one that works only in a still front photo.
The safest stopping zone usually keeps the new edge above the skin that shows obvious lower forehead movement. The front edge should still allow softness with single hair grafts, small irregularities, a gradual transition, and a design that does not look like a painted border. The lower the line goes, the more demanding every technical detail becomes.
Old photographs can help, but they should not control the design by themselves. A teenage photo may show thicker hair, a different pattern, or a face that no longer matches the current donor budget. I may use old photos to understand the patient’s natural direction and proportions, but I do not try to recreate every millimeter if the anatomy and future loss risk say no.
Overly low line is hard to repair
A hairline that is placed too low creates several problems at once. It uses grafts early, increases the surface area that must be filled, pushes the temple points into a harder position, and leaves less room for future thinning behind the line. It can also shorten the forehead in a way that does not match the rest of the face.
Repair is the larger issue. A transplanted hairline that is too low is usually harder to correct than a line that was kept slightly conservative. Raising it may require selective removal, electrolysis, laser reduction, camouflage, staged redesign, or a combination of methods. None of those options is as clean as making the first design correctly.
Some patients notice the problem only after the grafts mature, when the density becomes more visible or the temples no longer support the central line. Others notice it later, after native hair behind the transplant continues to thin. The first surgery should protect the second decision. If the first design leaves no room, the patient loses options.
Hairline that feels high still needs a full diagnosis
A hairline can feel too high because of anxiety before surgery, early recovery appearance, open corners, weak temple points, a long forehead, or a conservative mature design. That feeling is worth discussing, but it does not prove that lowering is safe or necessary.
With a high hairline after a hair transplant, I separate three questions. Is the line truly too high for the face? Is it high because the corners or temples are weak? And can the donor area support lowering without weakening the plan for later years?
If the answer is yes, refinement may be reasonable. If the answer is no, simply moving the center down can create a new imbalance. The forelock, corners, temple points, middle scalp, crown risk, and donor reserve all have to support the lower position. A lower center with unsupported sides rarely looks natural.
Photos and video that make the limit clearer
For this question, one flattering front photo is not enough. I want a relaxed front view, a raised eyebrow front view, right and left side views, a top view, and preferably a short video showing facial movement. The raised eyebrow view is especially useful because it shows how low the forehead lines sit and whether the proposed hairline would cross into active movement.
Hair transplant planning from photos alone can start the conversation, but it cannot replace donor examination and live assessment. I still need to assess miniaturization, hair caliber, donor density, the contrast between skin and hair, growth direction, and how the face moves in real time.
The side views matter more than many patients expect. A lower central line often demands stronger side framing. If the center is lowered without checking the temples, the result can look narrow, heavy, or disconnected. A design that survives only from the front is not a finished design.
Age and future pattern change the answer
Age affects how much uncertainty remains. A younger patient may appear to have only a high forehead or early corner recession, while the final pattern is still not visible. If the first operation creates a very low hairline, later loss behind it can force the patient into a lifetime of chasing the original drawing.
The age, pattern, and donor risk discussion is not only about the birth date. I look at family history, medication options, miniaturization, donor strength, crown risk, and whether the proposed line will still make sense if hair loss progresses.
Older patients can also need careful planning. Age may make the pattern clearer, but it does not create unlimited donor hair. The design still has to respect facial proportions, temple shape, future crown demand, and the quality of the donor area. A safe stopping point is the one that still works if the hair behind it changes.
Donor reserve sets the surgical budget
Every millimeter of lowering uses grafts. A small change at the front can add a surprisingly large recipient area, and the lower line may also require temple reinforcement so the face does not look strong in the center and weak at the sides.
The same logic behind lifetime graft planning and donor limits applies here. The donor area is finite. If too many grafts are spent on a low frontal edge, fewer remain for the middle scalp, crown, future density work, or repair.
I also judge the hair itself. Fine straight hair, strong color contrast, low density, or visible miniaturization can make a low edge harder to soften. Thick or wavy hair may cover better, but it can also look heavy if the first rows are not selected and angled carefully. Donor planning decides how low the line can responsibly go.
Temple points decide whether the front belongs to the face
A central hairline cannot be designed in isolation. If the center is lowered but the temple points stay weak, the face can look wide at the sides and compressed in the middle. If the temple points are overbuilt to chase an aggressive central line, the side frame can look newly drawn.
Temple point restoration is unforgiving because angle, direction, hair caliber, and density are highly visible. The lower the front is placed, the more pressure there is to make the sides match. That pressure can spend more grafts and increase repair complexity.
In forehead and hairline lowering planning, the better operation is often not the lowest possible line. It is a modest central lowering, careful corner work, and a temple transition that belongs to the face. That can soften a high forehead without turning the whole frontal frame into a forced design.
Warning signs before accepting a low design
A very low proposed line raises concern if eyebrow movement has not been checked, if the clinic gives a graft number before examining donor quality, or if the plan does not explain what happens when future hair loss continues. A line that is very straight, dense, and symmetrical should also be questioned, because natural hairlines are not built like a border.
A second opinion before hair transplant surgery is useful when the consultation feels rushed or the design is based mainly on a patient’s desired photo. A second review is not about being negative. It tests whether the plan can defend its own stopping point.
During that review, I want to see the donor area, old photos, current loss pattern, temple shape, facial movement, proposed graft distribution, and the exact reason the line stops where it stops. If the answer is only “because you asked for it lower,” the plan is incomplete.
Use the 10 hairline lowering slides below to separate forehead movement, the temptation to place the line too low, donor budget, temple balance, old photos, future hair loss, warning signs from a line that looks too straight, soft edge planning, repair difficulty, and the final stop rule. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.