


Widow Peak Hairline and Transplant Planning
A hair transplant can sometimes soften a widow’s peak, but the better plan is often to preserve part of it rather than erase it. A true widow’s peak can be an inherited V shaped hairline, not a defect. It becomes a transplant question when the temple corners recede around it, the front edge thins, or the central point is so sharp that it no longer fits the face.
For a small refinement, the plan may need only 300 to 800 grafts. If both temple corners need real rebuilding, the number may move toward 800 to 1,800 grafts. If the whole frontal hairline is being lowered, the operation becomes larger and much more demanding for long term donor management.
A transplant adds hair. It does not remove the native hairs that form the central point. So the real decision is not simply whether the peak can be changed. It is whether filling around it, softening it, or keeping part of it will look natural now and still make sense as the surrounding native hair changes in the future.
Widow’s peak is different from ordinary recession
A widow’s peak and a receding hairline are not the same thing.
A true widow’s peak is a V shaped or slightly pointed shape in the center of the frontal hairline. Some people have it from childhood. In that case, it is usually a hairline trait, not a sign that the hairline is failing.
A receding hairline is different. The temples move backward, the front edge becomes weaker, the hair miniaturizes, or the outline changes over time. The common confusion happens when the central peak stays in place while the corners move back. The peak then looks stronger, sharper, or more isolated, even though the real problem is often recession around it.
Before I call it recession, I like to compare old photos with new photos under the same conditions. The hair should be pushed back, with no fibers, no wet look gel, and the same camera angle. If the central point is stable but the corners are moving, the surgical question is usually corner support, not flattening the whole peak.
A stable widow’s peak does not always need surgery. If the hairline is dense, age appropriate, and unchanged for years, flattening the peak can make the line look lower, broader, and less natural. If the temples are truly receding, the plan may need to protect the central shape while rebuilding the corners carefully.
Widow’s peak planning lens
Four checks before changing a widow’s peak
A widow’s peak is not just a point to remove. The better plan depends on whether the shape is inherited, whether recession has changed the corners, and whether softening will still fit the face later.
Inherited shape
Is the peak part of the natural hairline?
Some peaks are inherited and can suit the face. Removing the central point can make the whole front look too flat.
Often no. First decide whether the corners need support while part of the central shape is preserved.
Use this as a planning frame, not a diagnosis or approval for surgery. The final plan still depends on donor reserve, recipient area anatomy, hair type, medical history, and future hair loss risk.
Transplant can soften a peak more safely than erase it
A hair transplant does not remove the native hairs that create the central point. It changes the visible outline by adding grafts around that point, usually in the corners or along the frontal edge. That can make the peak look softer, less isolated, or less sharp, but it is not the same as erasing the original hairline.
This distinction matters when the central point already sits low. If I try to hide a low point by filling both sides heavily, I may be pushed into a lower and broader frontal line than the face actually needs. That uses more grafts, leaves less flexibility for future hair loss, and can make the result look obviously constructed.
When someone wants the peak completely gone, I first ask what is really bothering them. Sometimes it is temple recession. Sometimes it is hairstyle, forehead shape, or an old photo that no longer fits their age. Often, the better surgical plan is not to remove the peak, but to soften the contrast around it while keeping enough irregularity for the hairline to age well.
Do not try to solve this by plucking, waxing, electrolysis, or laser hair removal on the central point before a proper assessment. Those native hairs may be useful for the final design. If true hair removal is needed, it should be planned separately from transplant design, because transplant surgery adds coverage. It is not a hair removal procedure.
Surgery is reasonable when recession changes the shape
A hair transplant becomes reasonable when the widow’s peak is part of a wider frontal hairline problem that can be planned safely. That usually means the temples have recessed, the front edge has thinned, or the goal is a modest refinement that fits the face and does not spend too much donor hair.
In my planning, I separate three different goals. One plan preserves the peak and fills the temple corners. Another softens a very sharp central point. Another lowers the whole front. These are not the same operation, and they should not use the same design.
If the goal is only to soften the transition around the peak, the graft number can be modest. If the plan tries to erase the peak visually and create a broad, low, straight hairline, the graft demand rises quickly and the result may look artificial. I treat widow’s peak planning as part of hairline design in hair transplant, not only as a graft count discussion.
A good plan protects the donor area, respects the remaining native hair, and avoids a shape that looks exciting on the day of surgery but too low, too flat, or too demanding years later.
Stable widow’s peak can be left alone
I am cautious when someone is very young, has no clear hair loss, or is mainly trying to remove a feature that is actually helping the face.
That central point can frame the face naturally. It can make the hairline less flat and help avoid the painted on look that appears when every small irregularity is erased. In many men, a slight central point with softer temple corners looks more natural than a perfectly horizontal line.
If someone is 18, 19, or in the early twenties and the hair loss pattern is not stable, surgery around the widow’s peak can be a mistake. The corners may keep moving back. The transplanted edge may remain while the native hair behind it weakens. That can force a second procedure earlier than expected. This is the same reason mild recession and Norwood 2 hair transplant cases need slow planning.
If the concern is active thinning rather than shape, the first step may be diagnosis and stabilization. In selected cases, surgery is still possible without finasteride, but the design has to be more conservative because future native hair loss is less protected. The medication decision is different from shape design. That is where hair transplant without finasteride becomes relevant.
Design should avoid an artificial peak
The most obvious mistake is making the widow’s peak too sharp. Natural hairlines have irregularity, softness, and transition. They are not graphic shapes drawn with a ruler.
At the very front, the edge needs finer single hair grafts, subtle spacing, low angle, correct direction, and a soft transition into the native hair. When I create the recipient area incisions, I am not only placing hair into an empty space. I am deciding how each hair will leave the skin and how the new edge will blend when the hair is combed back.
The direction of the existing peak matters. Some central hairs lie forward, some curve to one side, and some meet a small cowlick like change in direction. The grafts around the peak have to respect that direction. If the new hairs stand too upright or point against the native flow, the line can look artificial even when the graft count is reasonable.
Behind that front edge, stronger grafts can create more visual density. If thick multi hair grafts are placed at the edge of a peak, the result can look pluggy or theatrical, especially when the hair is wet or brushed away from the forehead.
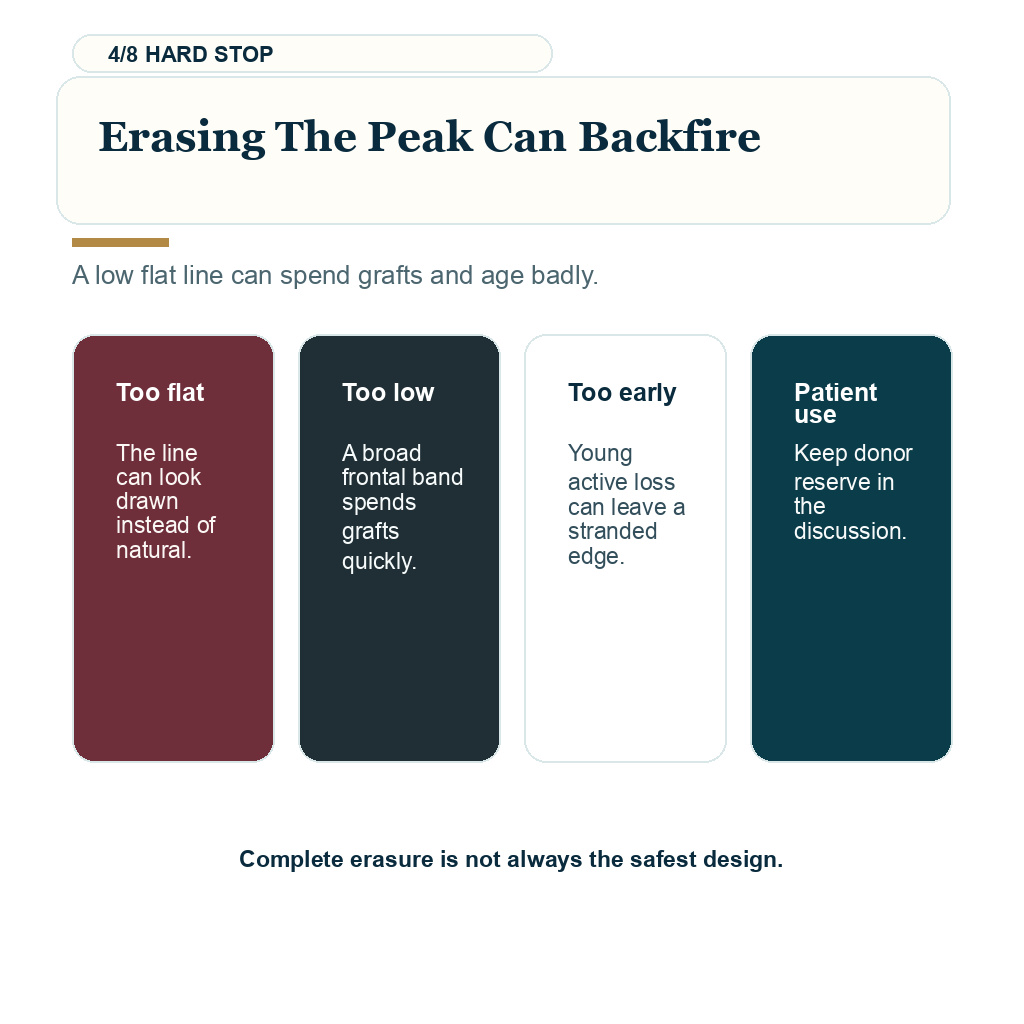
The second mistake is flattening the whole hairline to remove the peak. Low and flat hairlines may look clean in a mirror, but they become a warning sign when the design ignores age, temple shape, hair direction, future hair loss, and donor capacity.
The third mistake is forgetting the side transition. A central peak cannot be judged alone. The temple corners, frontal temporal angle, and true temple points all influence whether the face looks balanced. If the side temple area is weak, you may also need to understand the limits of a temple point hair transplant, which is a more delicate area than many people expect.
Graft numbers depend on the corners and frontal line
For a very small central or corner refinement, the plan may be around 300 to 800 grafts. For both temple corners with a visible V shaped hairline, many cases are closer to 800 to 1,800 grafts. If the plan includes major frontal lowering, wide temple reconstruction, or dense frontal band rebuilding, the number may move higher.
These numbers are not a promise. They change with hair caliber, skin hair contrast, recession depth, donor density, hair direction, and future hair loss risk behind the planned edge.
A small softening procedure is not the same as rebuilding the whole front. If the design becomes broader, lower, and denser, it spends more grafts and leaves fewer options for later thinning.
Many people ask for a graft number before the design is even safe. That order is backwards. First, I decide whether the proposed shape should exist. Then I decide whether the donor area can support it. Only after that does the graft number become meaningful.
If the main problem is the temple corners rather than the central point, planning depends more on how many grafts are needed for the temples. If the goal is lowering a naturally high forehead, that becomes a different discussion from a narrow widow’s peak refinement, and the risks are closer to a hair transplant to lower a naturally high forehead.
Young patients need more caution
Grafts can grow there. The real concern is using permanent donor grafts to chase a hairline shape before the future pattern is clear.
A young person may have a natural widow’s peak, early temple recession, or active androgenetic hair loss. These can look similar in casual photos. If surgery is done too early and the native hair keeps thinning behind the transplanted line, the result can age badly even if the transplanted grafts themselves grow.
Before planning surgery, I review miniaturization, family pattern, rate of change, donor strength, medication history, and tolerance for future maintenance. When hair loss is still moving quickly, the concern is similar to having a hair transplant too early while hair loss is active.
In a young case, a conservative design can be wiser than a dramatic correction. A softer corner, a slightly preserved peak, and fewer grafts may protect more options than a dense low line that uses too much donor hair at the front.
Women need a different hairline assessment
For women, the question can be different. A patient may ask about a widow’s peak because she wants a softer frame, a less pointed center, or a more rounded feminine hairline. The decision still depends on diagnosis.
A woman with a stable naturally high or V shaped hairline may be a candidate for careful frontal refinement. A woman with diffuse thinning, hormonal hair loss, traction damage, or active shedding needs a different assessment first. The transplant should not be used to hide an unstable diagnosis.
The design is also different. A female hairline usually needs softness, facial framing, and careful transition at the temples. Trying to make every female hairline perfectly round can look heavy, while leaving a small central point may sometimes look more natural. For broader planning, the more relevant page is female hairline hair transplant.
Before and after photos need several checks
Do not judge a widow’s peak result only from one front facing photo under flattering light. Ask whether the hairline still looks natural when the hair is combed back, under harsh light, from the sides, wet, dry, and on someone older than the ideal marketing age.
For your own consultation, send photos with the hair clean and dry, brushed straight back, and also in the style you actually wear. A short video turning from front to both sides can show whether the peak, temple corners, and side transitions belong together. Avoid fibers, concealer, or heavy styling product in those review photos.
Look at the front edge. It should not look like a hard border. Look at the center point. It should not become a sharp triangle unless that shape truly belongs to the face. Look at the corners. They should blend into the temples instead of forming a disconnected cap.
Also check whether the surgeon preserved enough irregularity. Some asymmetry is normal in a natural hairline, but true imbalance after surgery is a different problem. If your concern is an existing result that looks uneven, an uneven hairline after hair transplant needs to be judged by separating swelling, early healing, natural irregularity, and a real design issue.
A strong widow’s peak result usually does not announce itself. It frames the face, softens the recession, and still looks like the person could have been born with that hairline.




Result must still fit as you get older
This is the part I check before drawing a lower or flatter line.
Correction of a widow’s peak can look wrong at 40 if the line looked good at 25 but was too low, too dense, too flat, or disconnected from the temples. The face changes. Native hair may keep thinning. The crown may need attention later. Donor hair is finite.
Designs that age naturally leave some room for the face and the remaining hair to change. Sometimes that means keeping part of the widow’s peak instead of erasing it. Sometimes it means filling the corners only enough to soften recession. Sometimes it means refusing surgery for now because more time, medication response, or diagnostic clarity is needed.
A strong hairline is not always the lowest hairline. A strong result is one that still looks reasonable years later. The same long term thinking applies to every hair transplant that should look natural as you get older.
My decision starts with stability and facial fit
I respect a widow’s peak before changing it.
If the peak is natural and the surrounding hair is stable, the right decision may be to leave it alone. If recession has made the peak look too sharp, a careful transplant can soften the corners without destroying the character of the hairline. If the request is to erase the peak completely and build a low flat front, I become much more cautious.
For me, a good widow’s peak transplant is not the one that creates the most dramatic new shape. It is the one that makes the face look more balanced without making the surgery obvious. That requires conservative planning, fine graft selection at the front edge, correct angle, careful temple transition, and clear judgment about future hair loss.
If the design protects those things, a hair transplant can help. If it does not, the safer answer may be to wait, stabilize the hair loss, or preserve the widow’s peak as part of a natural adult hairline.