Norwood 2 Hair Transplant When Early Surgery Is Worth It
A hair transplant at Norwood 2 can be worth considering, but it is often too early. If the recession is mild, the hair loss is still changing, the patient is young, or the proposed hairline is very low, I do not rush to use donor grafts. At Norwood 2, technical possibility is not enough. The decision is whether surgery is strategically wise.
A mild widow’s peak can make this decision more confusing, because the center may look strong while the corners are just beginning to recede.
One patient may have a Norwood 2 shape that has settled into a mature adult hairline and only needs small, conservative refinement. Another may look similar in one photo but still be actively moving. I treat those situations differently, because donor hair is limited and a small decision at the front can affect the whole lifetime plan. When the pattern has already crossed into deeper corners, Norwood 3 hair transplant planning needs a different donor and design conversation. I make that same mature hairline or receding hairline distinction before treating a Norwood 2 outline as a graft request.
Norwood 2 needs careful judgment
Norwood 2 usually means there is recession around the temples, but the central forelock and overall density may still look strong. Some men keep this shape for years and it becomes a mature adult hairline. Others are only at the beginning of a pattern that will move toward deeper temple recession, frontal thinning, crown thinning, or diffuse loss.
I judge Norwood 2 from more than the label. I look at age, family history, hair caliber, miniaturization, donor area strength, medication history, and whether the hairline has changed recently. These details decide whether the patient is a good candidate for hair transplant surgery or someone who should wait.
The risky decision is to treat every small corner recession as a defect that must be filled immediately. A transplanted hairline is a surgical commitment. If it is placed too low or too aggressively, the patient may look good for a short time but become difficult to manage as natural hair loss continues behind it.
I also separate appearance from urgency. A Norwood 2 hairline may bother the patient every time he looks in the mirror, but that concern does not by itself mean the scalp is ready for surgery. My responsibility is to judge whether the operation will still look sensible when the patient is older, not only whether the corners can be filled today.
Early hairline decision lens
Four checks before using grafts at Norwood 2
Norwood 2 can be a real concern, but mild recession does not mean I would operate right away. Stability, age, donor reserve, and line design decide the safer path.
Stability
Is the recession stable or still changing?
A small corner can feel urgent, but recent change, miniaturization, or new crown thinning can make early grafts a weak choice.
It can make sense when recession is stable, donor strength is good, the goal is modest, and the design will still look natural later.
Use this as a planning frame, not a diagnosis or approval for surgery. The final plan still depends on donor reserve, recipient area anatomy, hair type, medical history, and future hair loss risk.
A Norwood 2 hair transplant makes sense only in selected cases
A Norwood 2 hair transplant can make sense when the recession is stable, the donor area is strong, the patient understands future hair loss risk, and the planned hairline is conservative. The case is easier to justify when the patient is not trying to recreate a teenage hairline, but wants a natural adult shape that will still look appropriate later.
The most suitable cases are usually modest, not dramatic. The goal may be to soften deep temple corners, improve framing, or correct asymmetry without pretending that the patient has no future risk. In that case, surgery can be a precise refinement rather than an emotional reaction.
I also separate temple corner work from temple point work. Closing a small frontal corner is not the same as rebuilding the side temple angle near the outer forehead. Temple points use very visible grafts, so I only add them when they truly fit the face, hair direction, and future donor plan.
A very sharp hairline drawing needs particular scrutiny. A natural result often depends on small irregularities, age appropriate height, and a transition that does not look artificial under harsh light. At Norwood 2, the difference between elegant refinement and overcorrection can be only a few millimeters.
A transplanted hairline must live with the rest of the scalp. If the frontal third, middle scalp, or crown begins to thin later, the early hairline choice should still make sense. In this part of the decision, natural hairline design matters more than simply lowering the line.
Fixing only one temple at Norwood 2 can create imbalance
Sometimes one temple can be refined, but I do not design it as an isolated triangle. Even if one side bothers the patient more, the whole frontal hairline has to be judged together so the result looks balanced from the front, from the side, and as the patient ages.
Natural hairlines are not perfectly symmetrical. One side may sit slightly higher, one temple may open sooner, and one side may photograph worse under harsh light. If I force one side to look too perfect while the other side remains a normal adult temple, the result can look more operated than natural.
If one temple is truly progressing faster, I look for miniaturization and compare old photos before making the decision. A small one sided refinement can be reasonable in selected stable cases, but if both corners are still changing, surgery on only the more worrying side may simply create a short lived correction.
Norwood 2 can be too early for surgery
Norwood 2 is often too early when the patient is very young, especially below the mid twenties, or when the hairline has changed quickly in the last year. Diffuse thinning, weak donor quality, crown involvement, or a strong family history of advanced baldness also make the decision more conservative.
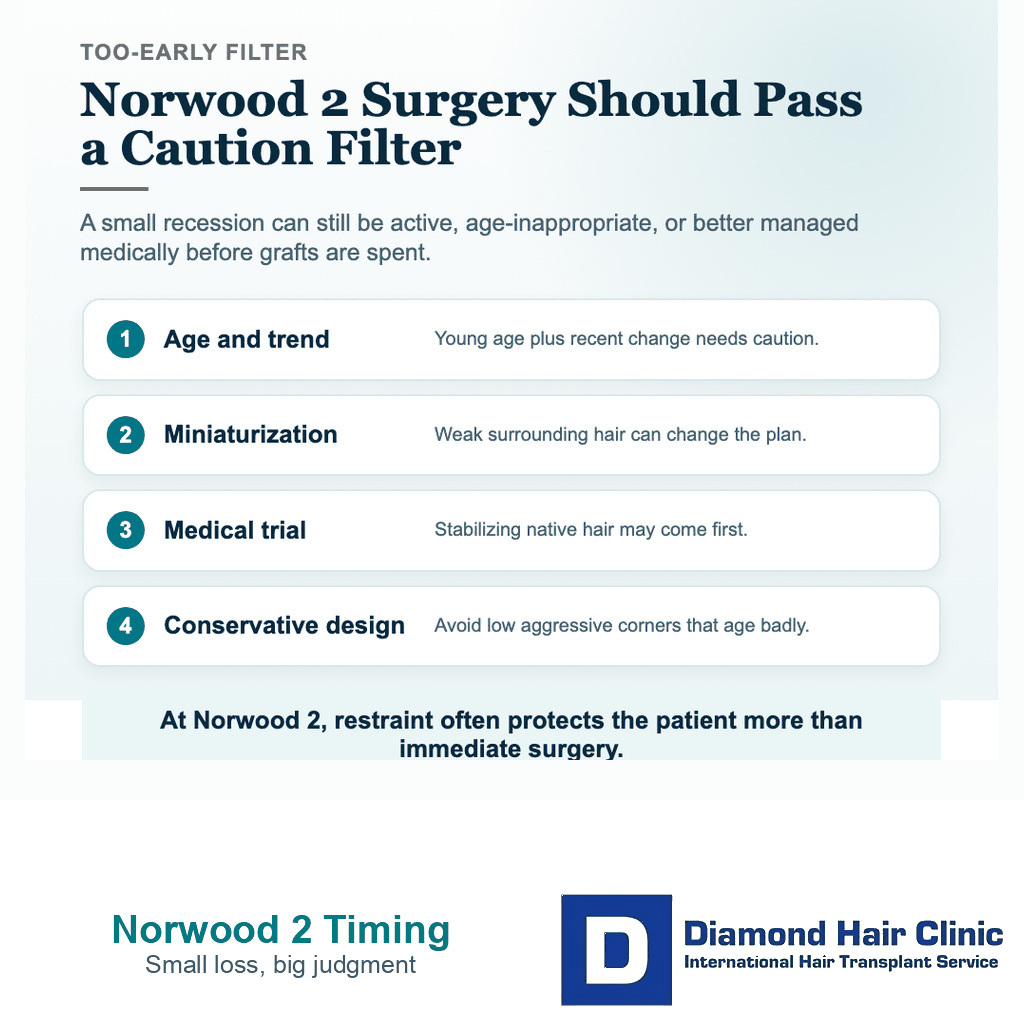
In many young patients, I often need to see at least 12 months of stability, observation, or response to medical treatment before using grafts. That point should not be taken to mean every patient must take the same medication. It means the plan needs enough information to show whether the pattern is stable or still moving.
If a patient is panicking because the corners look slightly higher in photos, that anxiety should not be the reason for surgery. First, we need to understand the hair loss pattern. A patient with early active loss may need a plan closer to trying medication before a hair transplant than rushing into surgery.
There is another reason to wait. If the patient keeps changing his requested hairline after looking at different online results, the target may not be mature yet. Surgery needs planning from the patient’s anatomy and long term pattern, not from one impressive online result.
Separate a mature hairline from active hair loss
I separate the shape from the behavior. A mature hairline may sit a little higher at the temples but then remain stable. Active hair loss behaves differently. It keeps changing, the miniaturized hairs become weaker, styling becomes harder, and the frontal area may lose density rather than only shape.
Old photos are useful when the patient has them. I compare the hairline over time, not only under one bathroom light or one harsh camera angle. I also examine the surrounding hair. I look at whether the area behind the recession is strong enough to support the new line in the future.
Understanding a receding hairline is useful, but the surgical decision is narrower. The same temple recession can be watched, treated, styled, transplanted, or left alone. The right choice depends on whether the recession is stable and whether surgery would protect or harm the long term plan.
Miniaturization is often the clue. If the hairs behind the corners are becoming thinner and weaker, filling only the empty triangle may not solve the real problem. The patient may need stabilization first, because the new grafts can grow while the native hair behind them continues to fade.
Reasonable graft numbers at Norwood 2 are usually limited
There is no responsible single graft number for every Norwood 2 patient. For limited temple refinement, the discussion may sometimes be around 800 to 1,500 grafts, but it can be lower or higher depending on hairline height, temple depth, hair caliber, density goals, and the surface area being rebuilt.
I also separate a small corner refinement from lowering the whole frontal line. Closing a shallow triangle at the temples may use a modest number of grafts. Moving the central hairline down, squaring the corners, or adding temple points can turn a small Norwood 2 case into a much larger lifetime commitment.
What concerns me is not the number alone. It is the reason behind the number. If a clinic suggests 2,500 or 3,000 grafts for mild Norwood 2 recession without explaining the long term plan, safe donor supply, and future loss risk, that is a reason to pause.
A small case can still be poorly planned if the hairline is too low. A larger case can be reasonable if the patient is not truly Norwood 2 and has more frontal loss than he realizes. The useful discussion is the logic behind the number, and why a page about whether 1,000 grafts can be enough may be more helpful than chasing a large number.
The graft number should match the design. If the design is conservative, the graft use should also be controlled. If the design requires a large number of grafts, I look at whether the proposed hairline is too ambitious or whether the patient has been classified too lightly as Norwood 2.

Use the 10 Norwood 2 planning slides below to compare pattern stability, conservative corner design, donor reserve, age context, medication history, one sided recession, adult hairline planning, density budget, and the final choice to proceed or wait. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.