


Hair Transplantation History From Early Experiments to FUE
Hair transplantation is often described through modern labels such as FUE, Sapphire FUE, robotic hair transplantation, artificial intelligence, or hair cloning. Those labels can make the field look very new.
It is not new. It moved slowly from reconstructive experiments and punch grafts to classification systems, FUT, FUE, recipient area refinements, robotic assistance, AI planning tools, and today’s careful discussion about follicle regeneration.
Here is the practical lesson. A technique becomes valuable only when it helps the surgeon protect donor supply, respect hair direction, plan future hair loss, and create a result that looks natural outside the clinic photograph.
For someone choosing surgery now, this history separates real surgical progress from a fashionable label.
A short practical timeline of hair transplantation
The early story was reconstructive. Dieffenbach opened the experimental idea, Hodara worked with scarred scalp in Istanbul, and Okuda showed more systematic punch grafting in Japan. The first question was whether moved hair could survive at all.
The 1950s added the principle of donor dominance and made modern hair transplantation clinically possible. Then the plug era proved a hard lesson. Growth alone was not enough if the result looked artificial.
Mini and micro grafting softened the old plug look. FUT then pushed the field toward natural follicular units, but it left the trade off of a linear donor scar. FUE changed donor harvesting by removing grafts individually, but it also made donor discipline more important because overharvesting could still create permanent cosmetic damage.
The current era is more complicated. Sapphire blades, robotic systems, body hair, AI, and hair cloning all belong to the story, but none of them removes the central requirement. The result still depends on diagnosis, donor management, hairline design, recipient area angle and direction, and long-term surgical judgment.
Why does this history still matter for a patient?

The first question in hair transplantation was simple. Could moved hair survive?
The harder question came later. Could moved hair survive, grow, and still look natural years later?
That second question changed the field. It pushed surgeons away from crude coverage and toward donor protection, smaller grafts, hair direction, irregular distribution, future loss planning, and softer hairline design.
In consultation, history is useful because it shows that the best progress did not come from the newest word or the most impressive graft number. It came from learning which surgical decisions age well and which decisions leave the patient with an obvious or difficult result.
When a person understands that difference, he asks better questions. He wants to know who is planning the operation, how the donor will be protected, how the recipient area will be created, and whether the result will still make sense if hair loss continues.
Which lesson should clinic choice take from history?
The practical lesson is simple. Do not be impressed only by the newest word, device, package name, or graft number. Every era had fashionable promises, and some of those promises later produced unnatural results.
Before choosing a clinic, ask who is responsible for the plan, who designs the hairline, who protects the donor area, who creates the recipient area incisions, and who follows the case after surgery. Who performs hair transplant surgery matters more than a technique label.
This becomes even more important when comparing clinics abroad. If the offer is built mainly around low price, high graft numbers, hotel packages, and fast booking pressure, slow down before trusting it. Choosing a hair transplant clinic in Turkey should still come down to surgical judgment, donor protection, and planning.
History should not make the patient nostalgic. It should make the patient harder to mislead.
The earliest era began with reconstruction, not cosmetic fashion
When people think about the history of hair transplantation, many imagine that the story starts in the 1950s with modern male pattern baldness surgery. That is understandable, because that is the moment when hair transplantation began to look more recognizable to us today. But the deeper history begins much earlier, not with polished cosmetic surgery, but with rough reconstructive thinking.
One of the earliest names associated with that beginning is Dr. Johann Friedrich Dieffenbach. Back in 1822, he conducted experiments involving goose quills, feathers, and hair.
By modern standards, those experiments were primitive. They were not hair transplants in the way we mean them today, when we speak about frontal restoration, crown coverage, or follicular unit surgery. But Dr. Dieffenbach still matters historically because he belongs to the era when surgeons were beginning to ask whether living tissue, or structures similar to living tissue, could be transferred in a way that enabled restoration rather than simple wound closure.
What makes this early phase interesting is that it did not yet think in the language of modern cosmetic restoration. It belonged to the language of experimentation, reconstruction, and possibility. That detail reminds us that hair transplantation did not begin as a beauty industry procedure. It began much closer to the broader medical instinct to restore what had been lost.
In that sense, even very crude experiments deserve historical respect, not because they resemble modern practice, but because they opened the conceptual door.
That early conceptual door became much more clinically meaningful in 1897, when Ottoman dermatologist Dr. Menahem Hodara carried out one of the earliest genuine hair restoration experiments in Constantinople, today’s Istanbul.
Dr. Hodara was working not with male pattern baldness, but with favus scars, bald scarred areas left behind by severe scalp disease. That context is very important.
The earliest truly meaningful clinical efforts in hair restoration were rooted in reconstructive need rather than vanity. They were trying to restore hair where disease had permanently destroyed it.
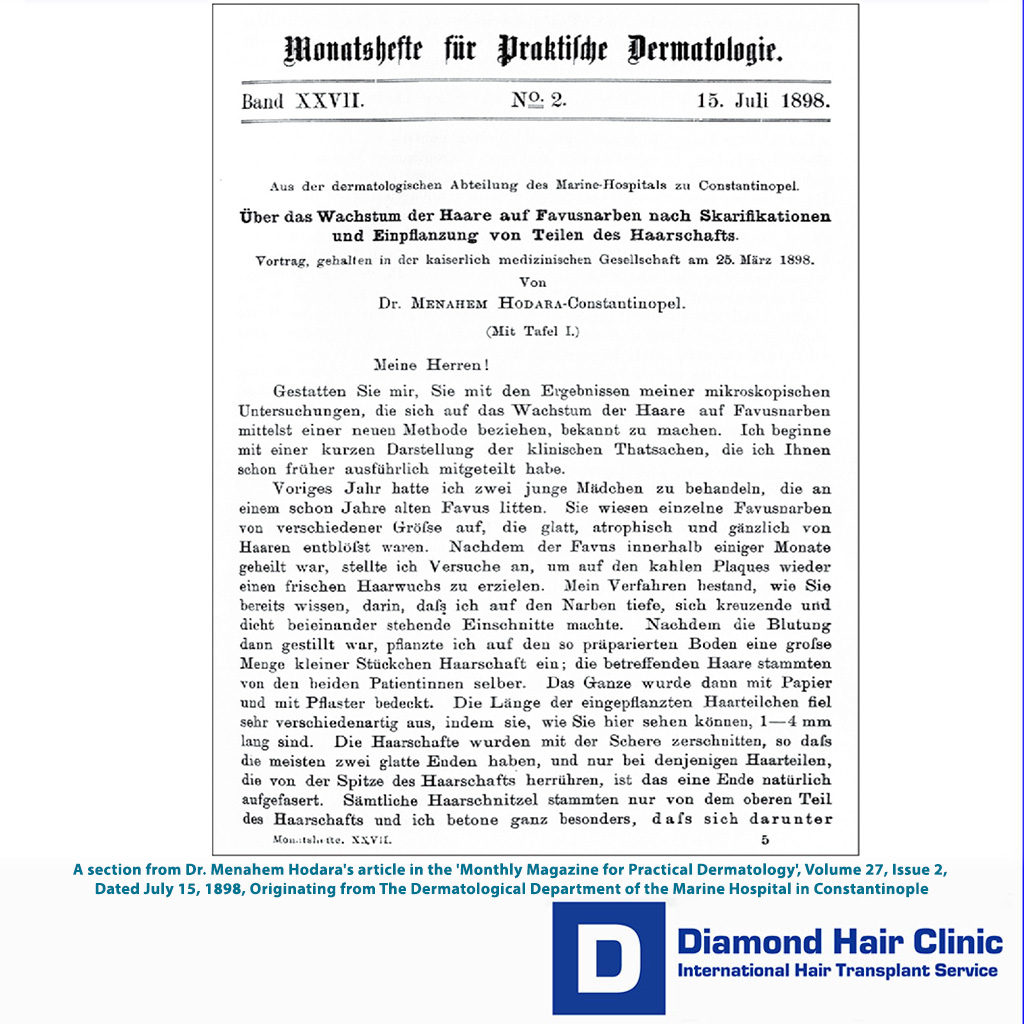
Hodara’s 1898 presentation matters because it described a real clinical attempt to bring hair back to scarred scalp after favus. The method was primitive by modern standards, but the intention was not cosmetic fashion. It was repair of damaged skin using the patient’s own hair.
I keep that historical reference concise. The important lesson for a modern patient is not the old technique itself. The lesson is that hair restoration began with medical limitation, scar tissue, and careful observation long before it became a global cosmetic industry.
Dr. Hodara’s method was surprisingly thoughtful for its time. He trimmed the patient’s hair very short, carefully prepared the scarred area, made fine incisions, and implanted small pieces of the patient’s own hair into the prepared skin. Then he observed what happened over time. Some hairs failed. Others survived and later showed stronger growth.
Dr. Hodara’s work is more than a historical curiosity. I see it as one of the first moments when hair restoration stopped being only experimental in spirit and became recognizably clinical. It was still primitive, yes. But it was already trying to solve a real problem in a real patient. That changes its place in history.
It is also one of the reasons I think Istanbul has a more meaningful relationship to the history of hair restoration than many people realize.
What happened next in Japan is equally important and, in many ways, even more technically decisive. In the late 1930s, Dr. Shoji Okuda carried out pioneering work using sharp punches to restore hair in patients with scars and cicatricial alopecia. His papers from 1939, later known as the Okuda papers, are among the most substantial early contributions from one physician in hair transplantation history.
One of the most revealing details in Okuda’s work is that he did not use 1 mm punches. He used larger punches, generally 2 to 4 mm. That matters historically because it shows that even at that early stage, surgeons were already confronting one of the deepest tensions in the field, how to balance invasiveness against graft preservation.
A smaller punch may sound more elegant, but if it transects the follicle, elegance means very little. Okuda understood that follicular survival mattered more than making the instrument superficially smaller.
What makes this chapter even more striking is that the world largely failed to absorb it at the time.
The Okuda papers were written in old Japanese script, and the disruptions of World War II helped bury them from wider international recognition. It was not until 2004 that Dr. Yoshihiro Imagawa, a retired gynecologist trained in the United States, helped rediscover and translate them into English.
It is also worth noting that Dr. Yoshihiro Imagawa was the father of Japanese hair transplant surgeon Dr. Kenichiro Imagawa. Medical progress is not only built through invention. Sometimes it is rescued through rediscovery.
When you place Dieffenbach, Hodara, and Okuda together in one line of historical sight, something very important becomes clear. The earliest era of hair transplantation was not one single event or one single country. It was a long, uneven reconstructive era in which different physicians, in different times and places, slowly pushed the field from abstract curiosity toward technical and clinical reality.
The early history deserves more room than it usually receives.
It helps us see that modern hair transplantation did not appear suddenly.
It was assembled, piece by piece, over generations.
Reconstructive origins shaped hair restoration philosophy
I think one of the mistakes people make when reading the history of hair transplantation is focusing too much on the techniques and not enough on the mindset behind them.
The earliest meaningful work in this field was largely reconstructive in spirit. It was not yet dominated by the modern cosmetic question of how to restore the temples of a Norwood 3 patient or how to blend frontal density into existing miniaturized hair.
The initial question was more basic and, in some ways, more serious. Can hair be restored to skin that has lost it due to injury, disease, or scarring?
That reconstructive origin matters because it gave the field its first moral and clinical backbone.
In reconstructive work, the surgeon does not begin with the fantasy of perfection. He begins with damage, deficit, and limitation.
That way of thinking leaves a mark on a field. It teaches patience. It teaches respect for tissue. It teaches that success may come partially rather than perfectly.
In a strange way, I think that reconstructive beginning gave hair transplantation one of its most enduring virtues, the understanding that scalp restoration is never just about adding hair. The real work is managing compromised biology, visible skin, and finite resources.
That perspective became even more important later, when hair transplantation shifted from scars and cicatricial alopecia toward patterned baldness.
Once the field entered the cosmetic era more fully, it gained scale, popularity, and commercial power, but it also became more vulnerable to superficial thinking. I believe the reconstructive roots should not be forgotten. They remind us that the field originally matured under the pressure of limitation, not excess.
And that memory is still useful today.
Where does Istanbul fit in early history and modern scale?
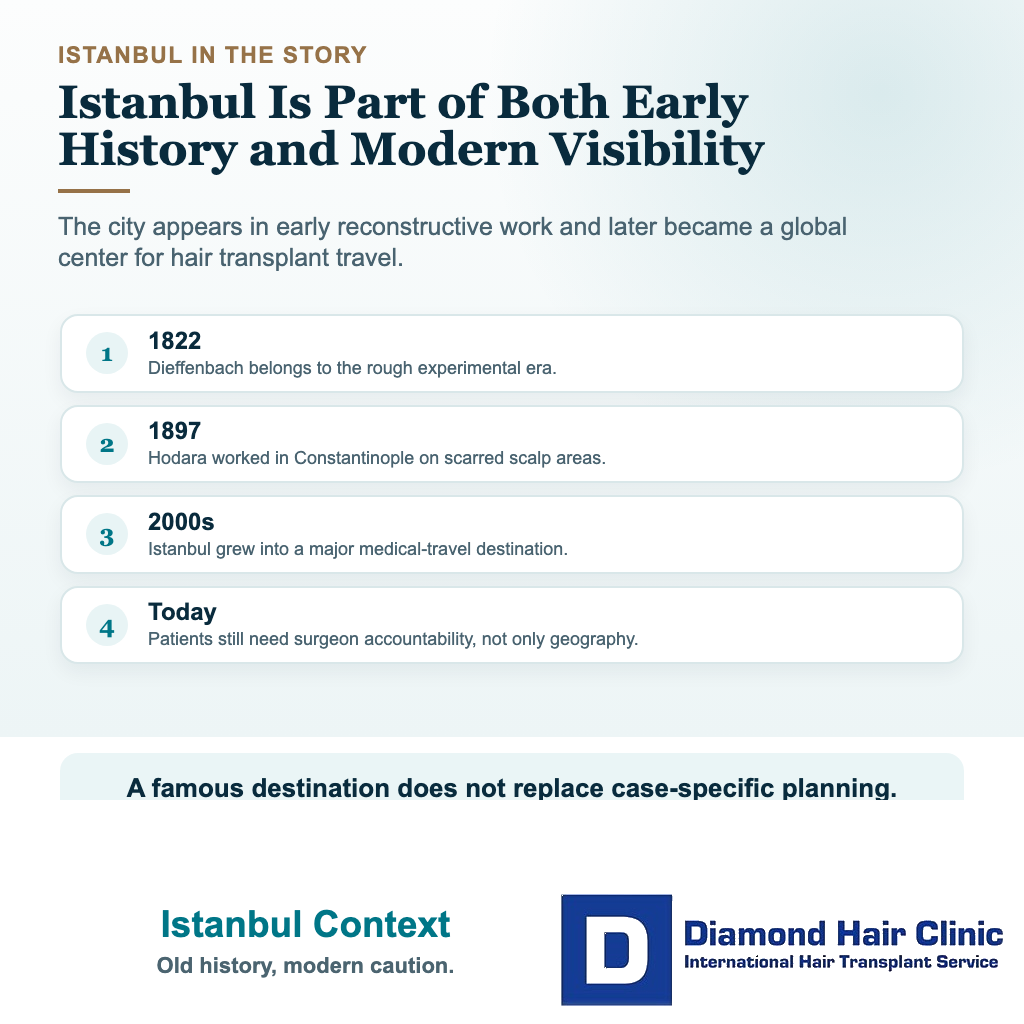
Turkey’s place in hair transplantation has two separate layers.
The first layer is historical. One of the earliest genuine clinical hair restoration experiments was carried out in 1897 in Constantinople, today’s Istanbul, by Dr. Menahem Hodara. He was working with favus scars, not ordinary male pattern baldness. That connects Istanbul to the reconstructive roots of the field, long before modern FUE tourism existed.
The second layer is modern. Over the last two decades, Turkey and especially Istanbul became one of the most visible destinations for hair transplant patients. Geography, air access, lower pricing, procedure volume, surgeon experience, medical tourism logistics, and online visibility all contributed to that rise.
Low price alone does not explain it. If Turkey had only been cheap, it would not have become so dominant. The high procedure volume also created repetition, practical familiarity, and a large professional ecosystem around hair restoration.
But scale cuts both ways. Istanbul became home to excellent surgical work, and it also became a place where the modern hair mill problem became very visible. The same medical tourism structure that can make surgery easier for international patients can also be used to sell speed, volume, and delegation instead of medical responsibility.
For that reason, Turkey’s role in the history of hair transplantation is not a simple success story. It is a story of access, experience, global visibility, and contradiction. Istanbul helped make hair transplantation in Turkey more accessible to the world, but it also showed why popularity and quality must never be treated as the same thing.
The 1950s brought donor dominance and pattern classification
The 1950s changed everything because the field finally moved from an interesting concept to a clinically meaningful treatment.
One of the important names of that period was Dr. James Bruces Hamilton, usually referred to simply as James Hamilton. His work on male pattern baldness, based on observations in more than 300 men, led to the Hamilton Scale in 1951.
That scale was extremely important because it framed baldness as a recognizable, progressive pattern rather than a random cosmetic loss. Surgery cannot be planned intelligently if hair loss is understood only as how the patient looks on one day. It has to be understood as a process. Hamilton helped bring that understanding into the field.
At around the same time, Dr. Norman Orentreich made the breakthrough that shaped modern hair transplantation more than any other, the principle of donor dominance.
This principle showed that hair follicles taken from the more permanent donor zone retain much of their original character even after being moved into balding areas.
In simple terms, donor hair behaves like donor hair even after transplantation. Without that insight, modern hair transplantation would not exist. The entire logic of the field depends on it.
Dr. Orentreich also began using large punches in the early 1950s, initially as large as 6 to 12 mm, later refining the method toward 4 mm punch grafts. These grafts proved that hair could survive transplantation. That alone was revolutionary. For the first time, baldness could be treated surgically in a way that produced actual growth.
But solving survival created the next major problem the field had to confront, and that problem was not biological.
It was aesthetic.
The plug era proved growth was not enough
Because the field achieved one kind of success and still created a new kind of failure.
The early punch graft era proved that transplanted hair could grow. That was a real medical success. But the grafts were often too large. They were often too grouped. And they were often too obvious.
The result became known as the plug look or the doll hair look. That phrase survived for a reason. It described something people could see instantly. The transplant did not disappear into the patient’s face. It announced itself.
That kind of visible unnaturalness has a special psychological cost.
A person who loses hair often wants to look more like himself again. But a person with a visibly pluggy transplant can end up feeling that he has exchanged one form of self consciousness for another. He no longer looks bald in the same way, but he may now look surgically altered. That is a very important distinction, and I think it explains why the plug era damaged the field’s reputation so deeply. It was not only that the results were imperfect. It was that many of them were socially legible as surgery.
The practical burden of the plug era made things worse. Deep frontal recessions could require around 150 to 200 plugs over 3 to 4 months, and larger frontal and crown cases could require 400 to 500 plugs over 7 to 8 months.
The donor area also paid a price, because the large punches created large wounds and visible scarring. So the patient could be left with an aesthetic compromise in both the recipient and donor zones.
And then came the next problem, repair. Once a pluggy result existed, it was not easy to soften, and later generations of surgeons had to devote considerable creative and technical effort to correcting the consequences of this era. Plugs had to be reduced, removed, redistributed, camouflaged, or visually broken up.
In other words, part of the field’s future labor was consumed by cleaning up the visual language of its own past. The plug era did not simply precede refinement. It actively forced refinement by making the cost of crude coverage impossible to ignore.
The plug era taught the field one of its hardest lessons. Survival is not enough. A transplant can grow, cover, and be biologically successful, yet still fail aesthetically if it betrays itself socially.
That is a lesson the field should never forget. Even in 2026, whenever a clinic becomes too obsessed with dramatic numbers, hard frontal lines, or visual punchiness rather than naturalness, I think we are seeing a modern variation of the same old mistake.
Better baldness classifications made planning more mature
As surgical techniques evolved, doctors also became much better at classifying hair loss.
That mattered far more than many patients realize.
In 1975, Dr. O’Tar Norwood revised Hamilton’s classification after studying around 1,000 patients. He recognized patterns that Hamilton had not fully included and added the Type A variant, helping create what became the Hamilton Norwood Scale, still the standard framework for male pattern baldness.
That was a major step in surgical maturity because it helped surgeons think not only about what the patient looked like that day, but also about where the pattern might go in the future.
Norwood is also historically interesting for another reason. He later questioned donor dominance in its most absolute form after observing that recipient areas might influence certain characteristics of transplanted hair, including texture. Whether one fully agrees with that interpretation or not, the discussion itself is valuable because it shows that even central medical ideas continue to be examined and refined.
For women, Dr. Erich Ludwig made an equally important contribution with the Ludwig Scale in 1977. He studied women with patterned loss and created a classification system specifically for female pattern baldness, which follows a very different visual pattern from male baldness.
This was not a minor side development. It was a major step toward making hair restoration more intelligent because good surgery depends on a good diagnosis, and a good diagnosis depends on understanding the actual pattern of loss.
This whole stage in history matters because it made planning more realistic.
A surgeon who understands only graft placement but not the natural history of hair loss is incomplete.
A patient is not just a scalp on one day.
He is a moving timeline.
And once the field began to take that idea more seriously, the surgery itself became wiser.
The field moved away from plugs through smaller grafts
The 1980s were a transition period, and one of the key names here is Dr. Bob Limmer.
He helped advance mini and micro grafting by using stereoscopic microscopes to dissect donor strips into smaller grafts. Compared with the old plug era, this was a major aesthetic improvement. Smaller grafts allowed softer hairlines, better density planning, and more refined cosmetic outcomes.
Mini grafts were often used to improve density, especially in the mid scalp and crown (vertex), while micrografts containing one or two hairs were used to create a more natural frontal hairline.
This was not yet the final form of modern hair transplantation, but it was an extremely important bridge between crude plug surgery and anatomically respectful grafting.
Still, mini and micro grafting still had limitations. Graft size could still be inconsistent. Some mini grafts could still look a bit coarse. Some micrografted areas could look too sparse. And because the technique had not yet truly centered on natural follicular unit anatomy, recipient areas often had to be larger than ideal, resulting in larger wounds and more variable healing.
Still, this era matters enormously because it marked a philosophical change.
The goal was no longer simply to place more hair into a bald area. The goal was to place hair in a way that looked softer, more natural, and more appropriate for the face.
That shift in thinking changed everything that came later.
Older flap and reduction procedures also damaged trust
It was not only the plugs that created problems.
During the same broader era, methods such as scalp reductions and flaps were also used in some patients. These approaches aimed to reduce bald area size or move hair bearing scalp in larger blocks, but they often created results that looked unnatural or difficult to hide.
When surgery becomes too focused on coverage and not focused enough on naturalness, the patient may technically have more hair but still look surgically altered.
The history of hair transplantation includes not only progress, but also correction.
The field had to learn, sometimes painfully, that the scalp is not just a surface to fill. It is a visible part of the face and identity. Once the result appears mechanical, aggressive, or obviously surgical, patient trust is damaged. Later refinement mattered so much.
It also explains why older generations of patients sometimes carry a deep suspicion toward hair transplantation in general.
For many years, the public image of the field was shaped not by its best work, but by its most visible mistakes.
That kind of reputational damage can last a very long time, and in some ways, I think the field is still recovering from it.
Mega sessions increased coverage but kept old limitations
In the mid 1990s, hair restoration entered the era of mega sessions, in which much larger numbers of mini and micro grafts were used in a single surgery.
This was a natural progression from mini and micro grafting, but it also made the weaknesses of that transitional method more obvious. Graft sizes remained inconsistent. Mini grafts could still produce a slightly pluggy appearance. Micro grafted areas could still seem too sparse if used alone. And because the method did not yet fully align with the true anatomy of follicular units, recipient areas often had to be larger than ideal, resulting in larger wounds and less predictable healing.
So mega sessions were historically important because they increased ambition and scale, but they also exposed the need for a more anatomically correct solution.
That solution was Follicular Unit Transplantation (FUT).
And this transition deserves more attention than it usually gets.
Because the movement from mini and micro grafting to FUT was not just a technical upgrade. It was a conceptual clarification.
Mini micro grafting had already moved the field toward smaller, softer, more refined grafts. But FUT went further by asking a more fundamental question.
Why are we still creating graft categories based on our own surgical convenience instead of following the natural structure that already exists in the scalp?
The shift from mini and micro grafts to FUT clarified the unit
This transition was an important turning point in the whole history of hair transplantation.
Mini micro grafting had already improved the field by yielding softer, more refined results than the old plug era. But it was still a transitional method. It was an improvement over something worse. It was not yet the most anatomically faithful way to transplant hair.
The deeper problem was that mini grafts and micrografts were still categories created largely by the surgeon’s dissection style. They were better than plugs, but they were not always identical to the scalp’s own natural organization.
FUT changed that.
It pushed the field toward respecting how hair naturally grows rather than continuing to impose artificial groupings onto the scalp.
That was not a small difference.
It meant that the aesthetic improvement was now being supported by a stronger biological logic.
Instead of saying, “Let us make the graft smaller so it looks better,” the field began saying, “Let us follow the natural follicular grouping itself.”
That idea is more mature surgically.
FUT became a milestone because it respected follicular units
In the 1990s, hair transplantation took another major step forward with Follicular Unit Transplantation, or FUT.
Dr. William Rassman played a very important role in this transition.
Later, together with Dr. Robert M. Bernstein, he helped formalize the idea of transplanting hair in naturally occurring follicular units rather than in larger artificial groupings.
Their work on follicular transplantation helped clarify this approach, and Bernstein’s later presentations gave it broader professional visibility.
This was a major leap.
FUT moved the field much closer to true naturalness by respecting how hair actually grows. Instead of creating arbitrary graft groupings, it worked with the natural follicular architecture already present in the scalp. That changed hair transplantation from a more approximate cosmetic camouflage method into something much more biologically and aesthetically coherent.
FUT also had practical strengths. It allowed many small grafts to be transplanted in one surgery. It required only limited shaving. It made discreet recovery easier for some patients. And in the hands of surgeons comfortable with large sessions, it made very high graft count procedures possible. That dramatically raised what the field thought was achievable.
Of course, FUT had a major trade off, the linear donor scar.
Even when later refinements, such as trichophytic closure, improved that scar, it remained an important limitation, especially for patients who wanted to wear very short hair.
So FUT was not the end of the story. It raised the aesthetic standard dramatically, but it also created strong pressure to develop a donor harvesting method that could avoid a visible linear scar.
Repair surgery became a chapter because old mistakes remained visible
Because once the field had produced enough unnatural work, it was forced to become skilled at undoing its own past.
Repair surgery became its own chapter in hair transplantation history when surgeons began confronting the aftermath of plug grafts, harsh frontal lines, poorly designed hairlines, visible scarring, depleted donor areas, and badly distributed density.
Corrective work could involve plug reduction, punch excision, redistribution, camouflage grafting, scar revision, and careful softening of the hairline. Quite often, repair work was more demanding than primary surgery because the margin for error was smaller and the donor supply had already been partially spent.
This is a very important part of the historical story because it shows that the field did not evolve solely through improvements in first time surgery. It also evolved by being forced to fix its own mistakes.
Repair surgery taught surgeons humility. It taught them that bad design can linger for decades, that donor mistakes are expensive, and that every aggressive decision made in the first operation narrows the options later.
In that sense, repair surgery helped deepen the field’s ethics as much as its technical skill.
Unfortunately, this is not only a historical problem.
Even today, many of the same mistakes are still being repeated, especially in lower profile cheap clinics, hair mills, and places where the surgeon is absent or barely involved.
The tools may look more modern, the marketing may sound more polished, and the package may appear more attractive, but the underlying mistakes are often very old, poor hairline design, aggressive donor use, unnatural graft distribution, and surgery performed with far more focus on speed and volume than on long-term quality.
In that sense, repair surgery is not only a chapter from the past. It is still a timely reminder of what happens when hair transplantation is treated like a commercial product rather than a careful medical procedure.
FUE emerged from the need to harvest without a strip scar
FUE did not arrive from one person in one moment.
Its development was layered, and that is exactly why the real history is more interesting than the simplified version many people hear.
The conceptual groundwork dates back to Dr. Masumi Inaba, who described using a 1 mm needle to extract follicular units. That is historically important because it shows that the roots of individual follicular extraction predated FUEs widespread recognition.
Later, Dr. Ray Woods in Sydney pushed direct individual follicle extraction further in practical terms.
Then, Dr. Robert M. Bernstein and Dr. William Rassman brought FUE into mainstream professional awareness through their influential 2002 publication.
After that, the technique continued to evolve. In 2005, Dr. Harris described a two step sharp/dull punch method, in which a sharp punch initiates the incision and a blunt punch continues deeper. That detail matters historically because it shows that even after FUE emerged, the extraction side of the procedure was still being actively refined.
FUE was not born fully perfected. It had to be improved, and the true history of FUE is not the story of one inventor but the story of early conceptual groundwork, practical development, formal publication, and continued technical refinement.
That gives a more reliable way to understand how modern FUE came into being. Patients wanted a way to avoid the linear donor scar associated with FUT, and FUE offered something extremely attractive, the ability to harvest grafts individually, leaving tiny scattered wounds instead of one long strip scar.
FUE became popular because the promise sounded simple
That made it very appealing to patients who wanted shorter hairstyles and less obvious evidence of surgery. It also fits the broader medical trend toward less invasive procedures.
As more clinics adopted it, FUE became a cornerstone of modern hair restoration.
But popularity also created misunderstanding. FUE is not scar free, it is not risk free, and it is still surgery. If it is done carelessly, it can still deplete the donor area or leave the donor visibly thinned when extractions are too aggressive or poorly distributed.
It is also still possible to overharvest, which is why FUE should never be described as a simple technical upgrade. The method changed the field, but it also demanded a new level of judgment from the surgeon and the team.
Another important anatomical limitation that many patients never hear clearly enough, FUE is partly a blind procedure.
The lower anatomy of the follicular unit cannot be directly seen during extraction. Hair angles and divergence change beneath the skin, which means transection is always a real risk if technique, planning, or punch control are weak.
That is one of the reasons I believe FUE should never be discussed as if it were simple or purely mechanical. It was a revolution, yes, but in many ways it demanded a new level of precision.
That is the reason the change in terminology from Follicular Unit Extraction (FUE) to Follicular Unit Excision (FUE) was meaningful. The familiar abbreviation stayed the same, but the newer wording more reflected the surgical nature of the procedure.
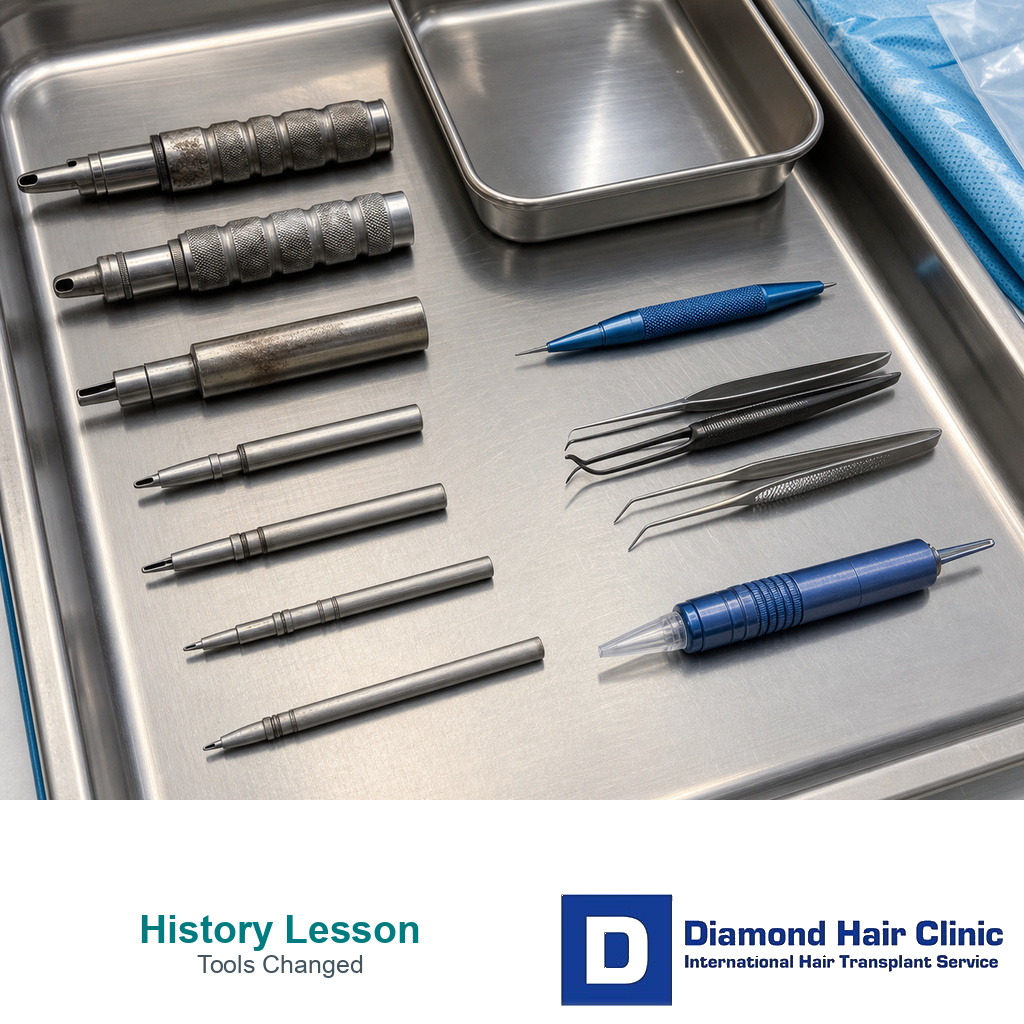
FUE tools changed precision, but not the need for judgment
A great deal.
Since the early 2000s, FUE punches, motors, and extraction systems have improved significantly.
Earlier tools were more manual, less forgiving, and more likely to damage follicles. The development of surgical micro motors and more refined punches made the procedure safer and more efficient.
These tools reduced trauma, lowered the risk of transection, and made the extraction process faster and less physically demanding.
These improvements mattered because the success of FUE depends heavily on graft viability.
If extraction damages the follicles, the surgery may sound impressive on paper but disappoint badly in growth. Better tools help protect follicular integrity, improve speed, reduce trauma, and make recovery easier.
They also make larger sessions more realistic in suitable patients. In the modern era, sessions of around 4,000 to 4,500 grafts may be possible in strong donor cases, though these remain lengthy procedures lasting 7 to 9 hours.
But even here, one truth remains unchanged. Better tools do not remove the need for better judgment, and an advanced punch in weak hands is still a problem.
This change shaped the way serious surgeons now think about the field. In the early years, especially during the plug era, the donor area was often treated more as a simple source area than as a finite strategic resource, and the focus was heavily on how much hair could be moved.
Over time, especially through the progression from plugs to mini and micro grafting, from mini and micro grafting to FUT, and then from FUT to FUE, the field slowly learned a harder lesson, the donor area is not endless. Every graft taken matters, every extraction pattern matters, and every mistake in donor planning has long-term consequences.
The donor area became the central strategic limit
I think this is part of the deepest lessons in the whole evolution of hair transplantation.
A patient may focus on the front because that is what he sees in the mirror, but a surgeon must think like a strategist.
The donor area is the bank account. Once it is spent carelessly, correction becomes much harder.
Modern hair transplantation has improved not only because recipient work has improved, but also because donor thinking has become more disciplined.
This change also shaped the field’s ethics. Once donor hair was understood to be finite, serious surgeons had to become more selective, more conservative, and more reliable.
They had to learn to say no to some plans, stop promising unlimited density, and stop pretending that one surgery could solve every future problem. That was another sign of maturity.
What makes the crown such a difficult area?
The crown has exposed the limits of almost every era in hair transplant history.
Even before modern FUE refinement, surgeons understood that the vertex was different from the frontal scalp. In 1985, Dr. Paul M. Goldman discussed punch grafting of the crown and vertex, which already treated this area as a special challenge rather than another bald surface to fill.
The reason is anatomical as much as surgical. The crown has a spiral or whorl pattern. Hair changes direction around a central point, so the surgeon must recreate flow and geometry, not only coverage.
As the field moved from plugs toward follicular transplantation, the crown remained one of the clearest places where naturalness mattered. Crown restoration can require a large number of grafts, often with less visible cosmetic return than the same grafts placed in the frontal half. A modest crown area can use 1500 to 2000 grafts, and the visual payoff still depends on pattern, hair caliber, contrast, and future loss.
For the crown, the important point is that it is not just coverage. Timing, whorl direction, graft demand, and donor reserve all matter at the same time.
I am careful with younger patients who want the front, mid scalp, and crown treated all at once. Sometimes the stronger plan is to build the frontal frame and mid scalp first, allow the result to mature, and then decide whether the crown deserves a second operation. That may sound less attractive than full coverage in one session, but it can protect the donor area and give the patient a safer path over time.
Medical tourism pressure can make this harder. A person travelling to Turkey may not want to return for a second surgery. High-volume clinics understand that psychology and may sell the idea of treating everything at once even when the donor capacity, age, crown expansion, and density expectations do not support it.
When grafts are spread too thin across the front, mid scalp, and crown, the patient can lose both ways. The front may be weaker than it should be, and the crown may still look thin because the area consumes grafts quickly.
For that reason, the crown should never be treated as a small extra area. It needs strategy, donor discipline, and the willingness to stage the plan when that is safer.




Female hair transplantation needed its own planning logic
Female hair transplantation deserves its own place in the story because female hair loss is not simply male baldness in another patient.
For a long time, one of the biggest problems was that hair transplantation developed mainly around male pattern baldness.
Many of the early surgical assumptions, visual priorities, and planning habits were shaped by male patients.
For that reason, Dr. Erich Ludwig’s contribution was so important. Once female pattern hair loss was more clearly classified (Ludwig Scale), the field could begin treating women with greater medical seriousness instead of forcing them into a male framework.
This was a very important step, because women often present very differently from men. In female patients, I have to think much more carefully about diffuse thinning, donor stability, part line density, frontal framing, and the possibility that the donor itself may not be as stable as it first appears.
In many women, the concern is not a clearly isolated bald zone like we often see in men. The thinning can be broader, softer, and much more complex. That means the surgery cannot be planned with the same logic.
As the field matured, female hair transplantation improved when surgeons became more selective and more careful.
The real progress came when the field stopped treating women as mere variations of male cases and began to respect the actual biology before it. It became more about proper candidate selection, proper miniaturization assessment, and a much more realistic understanding of where surgery can truly help and where it may be the wrong decision.
The history of female hair transplantation mirrors the field as a whole. It improved when surgeons moved away from simplistic formulas and toward more thoughtful medical judgment.
Unfortunately, this is also one of the areas where modern hair mills and weak medical tourism clinics still make serious mistakes. As a hair transplant surgeon, I still see women who had surgery in Turkey at clinics that clearly had very little understanding of female hair transplants, female hair loss patterns, or female hairline characteristics.
In many of those cases, the woman seems to have been treated almost as if she were simply a male transplant patient with longer hair. That is a very dangerous misunderstanding.
Female hair restoration often requires more diagnosis, more caution, and more careful judgment, not less. The donor must be judged very carefully. Diffuse thinning must be taken seriously. Frontal design must be approached differently. Central density and part line concerns often matter greatly.
And sometimes the most correct decision is not surgery at all, but medical treatment, further evaluation, or simply refusing the case.
When a clinic does not truly understand these realities, the surgery may still look busy and professional on the day, but the underlying planning can be deeply flawed.
The hair mill clinic model is already risky in men. In women, it can be even more dangerous, because female cases often require more nuanced judgment before a single graft is taken. Unfortunately, many women are still being treated as if female hair transplantation were just a minor variation of male surgery. It is not. And that misunderstanding continues to produce poor outcomes that could often have been avoided with better judgment from the outset.
Reconstructive cases still reveal the field’s deepest limits
Reconstructive hair transplantation still matters because the field did not outgrow its reconstructive roots. It simply added cosmetic sophistication on top of them.
In fact, reconstructive needs came before the modern cosmetic boom. Some of the earliest meaningful hair restoration efforts were not aimed at ordinary male pattern baldness but at areas where hair had been lost due to disease, scarring, or injury.
That is one reason I think reconstructive work deserves more respect in the historical story. It reminds us that hair transplantation did not begin only as a cosmetic wish. It also began as an attempt to restore something that had been visibly damaged or permanently lost.
That early foundation is important because it helps explain why reconstructive work still carries such a special place in the field.
That historical line never disappeared.
Modern hair transplantation is still used in burn scars, surgical scars, facial scars, eyebrow loss, beard defects, and other reconstructive settings where the challenge is not ordinary patterned baldness, but compromised skin and distorted anatomy.
In these cases, the surgeon is not working with a normal scalp and normal blood supply. He is often working with tissue that is stiffer, less vascular, less predictable, and much more unforgiving. That changes the rules immediately. It means the surgery usually requires more caution, more patience, and more humility than a routine cosmetic case.
As the field became more refined, reconstructive work did not disappear. It evolved along with the rest of hair transplantation.
A useful historical figure here is Dr. A. Barrera, whose 2005 paper on reconstructive hair transplantation of the face and scalp helped demonstrate how hair grafting could be used not only for ordinary scalp baldness but also for scars and reconstructive problems involving the scalp and face.
That places reconstructive transplantation clearly inside the modern follicular unit era rather than leaving it trapped as an old side topic. In other words, reconstructive work was not abandoned when cosmetic hair transplantation advanced. It continued to evolve with it.
Another important name is Dr. Bessam Farjo.
His 2015 review on hair transplantation in burn scar alopecia is especially valuable because it makes clear that post burn restoration is often a multistage process and that scarred tissue changes what can be expected from transplantation.
I think that point is very important. Reconstructive hair transplantation is not simply “regular hair transplantation in a different place.” Scar quality, tissue mobility, vascularity, and recipient area behavior all become much more important.
Burn cases, especially, remind us that hair transplantation is still very much a part of reconstructive surgery, not only aesthetic surgery.
The same pattern appears when we look beyond the scalp itself.
The same is true in eyebrow and facial hair reconstruction. Dr. Marcelo Gandelman was an important figure in that field, and later Dr. Jeffrey Epstein contributed significantly to the literature on eyebrow, beard, sideburn, and other facial transplantation.
That work matters because facial reconstruction by hair transplantation requires even finer control of angle, direction, and density than ordinary scalp work. A transplanted eyebrow or beard cannot hide behind the general mass of scalp hair. Its design is visible immediately, which means reconstructive facial cases often become one of the clearest tests of refined surgical skill.
More recent literature also shows that reconstructive cases continue to evolve rather than stand still.
Modern reconstructive work on eyebrow restoration after burns, facial scar management by hair transplant, and combined approaches that improve scar quality before grafting all point in the same direction. The field is still trying to solve the old reconstructive problem with better tools and better biological preparation.
Recent reconstructive approaches also explore improving scar tissue first, using methods such as laser therapy, fat grafting, or related recipient area preparation before transplantation, precisely because scarred skin does not behave like ordinary skin. That is another reminder that reconstructive transplantation remains one of the most medically demanding parts of the field.
And even in the modern era, some surgeons continue to advance the reconstructive side of the field by focusing on the hardest cases rather than the easiest.
A modern example of that ongoing reconstructive spirit is Dr. Sanusi Umar.
I think Dr. Umar is relevant here because his work is not centered on easy routine cases. It is centered on the kind of difficult patients that expose whether a surgeon truly understands the deeper limits of hair transplantation, severely scarred and donor depleted repair patients, advanced baldness where beard and body hair have to be used intelligently, technically difficult Afro textured hair extraction, eyebrow and facial hair reconstruction, and complex inflammatory or scarring scalp disorders such as acne keloidalis nuchae, folliculitis decalvans, and other cicatricial alopecias.
These are not cases where a surgeon can simply follow a standard cosmetic formula. These are cases where tissue quality, scarring, inflammation, donor depletion, curl pattern, and prior damage all change the rules.
For me, his work fits naturally into the reconstructive side of hair transplant history. It reminds us that even today, some of the most meaningful progress in this field still happens where cases are hardest, where tissue is compromised, and where standard, easy solutions are no longer enough.
Seen together, all of these examples point back to the same deeper truth.
I think this matters historically because it closes a circle. The field began with reconstructive need before it became a large cosmetic industry, and reconstructive work still remains one of the clearest tests of real surgical judgment.
It requires patience, tissue respect, conservative planning, and the willingness to accept that compromised skin changes the rules.
In a routine cosmetic case, a surgeon may be tempted to focus on density and visual impact. In a reconstructive case, he is often forced to think more carefully about survival, perfusion, direction, and whether the tissue itself is even ready for transplantation.
That mindset gives reconstructive hair transplantation a special value. It keeps the field grounded in medicine instead of letting it drift into sales language.
That ongoing reconstructive chapter gives hair transplantation more medical depth and dignity than people sometimes realize.
It reminds us that this field is not only about making people look younger or denser. It is also about restoring normality after visible damage, and in some patients, that may be one of the most meaningful things a hair transplant surgeon can do.
The internet changed visibility and marketing
The internet changed hair transplantation in two opposite directions.
It made the field more transparent. Weak results, overharvested donor areas, plug repairs, poor growth, and unnatural hairlines became harder to hide once patients could publish photos and follow-up diaries. That public record helped protect people from the old problem of invisible bad work.
It also gave patients a stronger voice. A person who felt isolated after a disappointing surgery could compare healing phases, ask questions, and understand whether the problem looked temporary, expected, or serious.
But online visibility also created new distortions. The internet can reward the most dramatic photograph, the highest graft number, the hairline that looks densest, or the clinic with the strongest marketing system. None of those things proves careful donor management or a plan that will age well.
Many patients get confused at exactly this point. A twelve month photo under ideal lighting is not the same as a durable surgical result. Popularity alone does not make a clinic safe. A dense first line can look impressive online and still be too hard, too low, or too expensive for the donor area.
The internet also changed clinics. Some learned how to present selected cases, videos, testimonials, and package offers more effectively than they learned how to protect the donor area. In that sense, the internet did not only spread information. It also commercialized perception.
For me, the patient lesson is direct. Use online material as a starting point, not as proof. Ask whether the clinic can explain diagnosis, donor reserve, recipient area design, graft distribution, aftercare contact, and what should not be done.
Modern hair restoration split into two models
By the time FUT and FUE had made hair transplantation more refined, the field was no longer facing only a technical question. It also faced a delivery question.
One path moved toward individualized, surgeon-led restoration. In that model, donor protection, hairline design, recipient area planning, patient selection, and long-term planning remain central.
The other path moved toward high-volume commercial production. The same technical words could be used, but the structure underneath was different. Speed, delegation, package selling, and turnover became more important than surgical depth.
This split became especially visible from the late 2000s into the 2010s as FUE became easier to market internationally. Medical tourism, online photos, package offers, and clinic videos made the procedure more visible, but they also made weak clinic models easier to sell.
Two clinics may both say FUE. One may be practicing careful restoration around one patient’s donor reserve and future loss. The other may be running a production model where the acronym is modern but the judgment is thin.
The difference is not the acronym. It is the structure. Who examines the patient? Who designs the hairline? Who decides the graft number? Who creates the recipient area incisions? Who stops the plan when the donor area cannot safely support it?
The modern era teaches a less comfortable lesson. Hair transplantation did not simply become better in a straight line. Part of the field became more careful and medically mature. Another part became more scalable, more commercial, and more detached from real surgical responsibility.
Robotic and body hair tools became easy marketing stories
Both robotic hair transplantation and body hair transplantation belong to the modern refinement era of hair restoration. Neither is imaginary, and neither should be dismissed as having no medical role. Robotic systems, including ARTAS robotic hair transplantation, represented real attempts to improve standardization and extraction efficiency, while body hair transplantation expanded donor possibilities for selected difficult patients, especially severe baldness and donor depleted repair cases.

Even so, body hair remains a niche option for carefully selected patients, and robotic systems remain adjunctive tools. Neither should be presented as the defining center of modern hair restoration.
A robotic system can be presented as if the machine itself guarantees superiority, even though the robot does not replace candidate selection, hairline design, donor judgment, or recipient area artistry. Body hair transplantation can be presented as if it solves donor limitations in a simple way, even though body hair differs from scalp hair in caliber, texture, growth cycle, and visual behavior.
Robotic hair transplantation is typically priced higher than standard manual approaches, which makes the robotic label useful as both a technology claim and a pricing tool. Body hair transplantation can also be marketed as an advanced rescue strategy, especially in patients who are frightened about donor depletion and strongly want more grafts.
The key distinction is not whether these methods exist. The concern is the commercial use of a real method as a branding device.
A clinic can make robotic sound like automatic superiority and make body hair sound like unlimited donor expansion, even though neither claim is true in a simple sense. Robotic systems assist part of extraction, but they do not replace the surgeon. Body hair can help in selected difficult cases, but it does not magically become ideal scalp donor hair.
Commercially, they also belong in the story of how hair mill clinics package novelty, charge more, and create a more marketable image of sophistication than the underlying surgical model may actually deserve.
Sapphire FUE belongs inside the broader FUE evolution
Sapphire FUE is not a separate historical chapter in hair transplantation in the same way as FUT and FUE.
It is better understood as a later refinement within the already established FUE era, especially within the longer evolution of recipient area creation.
That historical context matters.
Long before sapphire blades became a recognizable market term, hair transplant surgeons were already trying to refine the way recipient areas were created.
The field had moved through different recipient area tools and methods over time, and this part of surgery was already being adjusted and readjusted in the search for greater precision and control.
In that sense, sapphire did not suddenly create a new universe of hair transplantation. It entered a refinement process already underway.
The extraction side is still FUE.
The term sapphire usually refers to the blade material used for recipient area creation, not to a completely different donor harvesting method. Historically, Sapphire FUE falls within the established FUE timeline, not outside it.
Sapphire FUE appears to have emerged in 2014 and became more widely visible around 2015 to 2016.
That timing is important because it shows where sapphire fits in the bigger story.
By then, FUE was already well established.
The field was no longer mainly trying to prove that FUE could work. It was moving into a later phase, where attention increasingly turned toward refinements, presentation, terminology, and smaller technical distinctions within the modern FUE framework.
Historically, sapphire belongs to a period when hair transplantation had already entered its more modern stage, and the field was evolving through technical refinement rather than a major foundational breakthrough. Sapphire FUE should not be described as a revolution in the history of hair transplantation. It is more accurate to describe it as a term from the middle of the 2010s, after the field’s major structural changes had already taken place.
If FUT and FUE were major historical steps, Sapphire FUE was a later variation within the already mature FUE period. The same logic applies to naturalness. Smaller punches and grafts can help, but a natural result still depends on transition, irregularity, discipline, and respect for how real hair actually grows.
Modern naturalness is a design discipline, not a technique label
In the modern era, the field has gradually learned that a result can be technically successful yet fail aesthetically if it looks too sharp, too patterned, too dense in the wrong places, or too disconnected from the patient’s age and future hair loss.
At first, the field thought of improvement mainly in terms of survival, then in terms of smaller grafts, but true naturalness required something beyond both of those steps. It required understanding that the eye does not read hair only as a number of follicles. The eye reads softness, variation, rhythm, depth, and intentional irregularity.
A natural result does not come from making the frontal line sharp and dense in a geometric way. It comes from understanding softness, stagger, variation, and age-appropriate design, knowing when to be conservative, creating a transition zone that does not scream “transplant,” and resisting the temptation to force density in ways the scalp, donor area, or long-term plan cannot support.
Modern hairline restoration keeps returning to the same point, the frontal edge should transition gradually from finer, softer hairs into stronger density behind it, not look like a stamped border or what many patients describe as a wall of hair.
This is also where the field learned that naturalness is not only micro design, but also macro planning.
A transplant can look reasonable in a close-up photo and still feel wrong on the face if the overall shape, height, recession pattern, and density emphasis do not fit the person.
The modern era taught that naturalness depends not only on single graft placement, but also on larger visual architecture, where the density is concentrated, how the frontal forelock is handled, how the temporal recession is respected, and whether the design will still look natural if the surrounding native hair continues to thin.
Concepts such as central density and the frontal forelock became important precisely because they protect naturalness over time, not only in the first impression. For me, that is when the field moved from being mostly technical to being truly surgical and artistic, because the question was no longer only whether the graft could stay alive.
The more important question became whether the result could look as if it was never transplanted. That is more sophisticated than a simple technology prediction, and the answer is not simply to use single hair grafts. Single hairs matter, especially at the front, but naturalness is created by how they are placed, how the transition is built, how the irregularity is controlled, how the density builds gradually, and how the whole design fits the patient’s age, face, and likely future loss.
Modern guidance on recipient area creation and aesthetic assessment also emphasizes that angle, direction, density, distribution, and the relationship between recipient area and graft behavior remain central to the final appearance.
The modern era also taught another important lesson, a natural result must survive more than a clinic photo.
It should still look natural in daylight, with shorter styling, with wet hair, from different viewing angles, and as the patient ages. It should not depend entirely on one carefully selected before and after photo.
In that sense, real naturalness is durable.
It continues to make visual sense when lighting changes, when the hairstyle changes, and when the surrounding native hair changes. That explains why judgment matters so much.
An overbuilt result may look impressive early, yet age badly.
A well planned result usually looks less aggressive on paper, but more natural over time.
Naturalness is not just a technical method.
I see it as a design philosophy.
It is the point where biology, aesthetics, long-term planning, artistry, and surgical judgment all meet.
And that is one of the most valuable things the modern era has taught hair transplant surgeons.
Can artificial intelligence improve planning without replacing judgment?
Artificial intelligence may become useful in hair restoration, but it should be understood carefully.
AI may help with diagnosis support, donor mapping, density analysis, graft counting, extraction planning, follow-up comparison, and long-term tracking of hair loss progression. It may also improve robotic systems that assist part of extraction.
That does not mean AI can cure baldness by itself or decide whether surgery is right for a specific person. Biology still matters. Clinical trials still matter. Safety still matters.
I already see one small practical example. Some patients use AI tools to estimate how many grafts appear visible in post-operative photos. That can be interesting, but it should not be treated as medical proof. Lighting, angle, scabbing, hair trimming, image quality, and spacing can all mislead the estimate.
The more valuable future use may be trend tracking. Hair loss is not static. Native hair miniaturizes, crown loss expands, and a result that looks acceptable at twelve months may look different several years later if surrounding hair continues to thin.
AI may help surgeons and patients compare those changes more objectively. Still, donor protection, hairline design, candidate selection, and the decision to refuse a weak plan remain human surgical responsibilities.
Could hair cloning change the limits of transplantation?
If one future development could change the basic logic of hair transplantation, it is hair cloning, or more precisely hair follicle regeneration or hair multiplication.
Traditional hair transplantation redistributes existing follicles. It does not create a new permanent donor supply. Donor planning has shaped almost every major improvement in the field for that reason.
Hair cloning tries to address that limitation by multiplying cells that form hair or regenerating new follicular units. If it ever becomes clinically reliable, it could change the mathematics of hair restoration rather than only improving technique.
Patients need realism here. There is still no broadly approved, routine clinical treatment that reliably creates unlimited new hair follicles in everyday practice.
Current work includes dermal papilla cell expansion, induced pluripotent stem cell research, follicle organoids, scaffolds, bioengineering, and other regenerative strategies. That scientific direction is serious, but serious research is not the same as a mature treatment.
The difficulty is not only making cells survive in a laboratory. A follicle is a tiny organ. It has to integrate into scalp tissue, cycle properly, grow in a useful direction, produce cosmetically acceptable hair, remain safe, and be reproducible enough for normal clinical use.
Even if hair cloning works one day, the first useful versions may be more limited than patients imagine. They may help selected density, repair, scarred scalp, or patients with depleted donor supply before they ever become an unlimited solution for every bald area.
Hair cloning is not fake. It is not ready. Both statements can be true at the same time.
Until that changes, hair transplantation remains a way to redistribute existing donor hair. Hair cloning may become a major future direction for the field, but it still belongs to the frontier, not routine daily reality.
What does the full history really teach us?
The deepest lesson is not nostalgia. Hair transplantation improved when the field moved away from crude coverage and toward natural design.
It improved when surgeons took hair loss patterns more seriously, treated the donor area as precious, respected follicular units, and learned that a result must look natural for years, not only grow in the first year.
The long line from Dieffenbach, Hodara, Okuda, Hamilton, Orentreich, Norwood, Ludwig, Limmer, Rassman, Bernstein, Inaba, Woods, Harris, and many others is not only a list of names. It is the story of a field learning that survival, coverage, and novelty are not enough.
If you are choosing surgery now, use that history as a filter. Do not stop at the technique name. Ask who is planning the case, protecting the donor, designing the hairline, creating the recipient area, thinking years ahead, and deciding what should not be done.
Tools will improve. AI may help planning. Hair cloning may one day challenge the donor limitation that defines classic transplantation. But the patient will still need judgment from the surgeon. More technology does not by itself create a more natural result.
The history of hair transplantation still matters because it teaches that the best progress is not the loudest promise. It is the progress that protects the patient from an obvious, wasteful, or poorly planned result.