



Hair Transplant Tools Cannot Replace Surgeon Judgment
Tools and techniques matter in hair transplant surgery, but they do not matter more than diagnosis, donor planning, hairline design, recipient area control, graft handling, and surgeon judgment. A modern tool can help a good plan. It cannot make a weak plan safe.
This is where many patients become confused. One clinic promotes Sapphire FUE, another promotes DHI versus FUE, another promotes robotic extraction, implanter pens, punch size, blade type, or a premium package. These names sound objective. The history of hair transplantation shows the same pattern, where a label can become famous before patients understand what it actually changes. The useful distinction is whether the tool changes a specific surgical step, and whether the right person is making the decisions around it.
The distinction matters because hair transplantation is not one mechanical step. Extraction, graft sorting, recipient area incision, implantation, density planning, hairline design, and donor preservation all have to fit the same patient. If those decisions are poor, the tool name becomes decoration.
The tool should serve the plan. I decide the plan from the donor area, the recipient area, hair caliber, hair loss pattern, age, medical situation, expectations, and future risk. Only after that does the technique choice have meaning.
No tool can guarantee a better result
No tool can guarantee a better result by itself. A technique name may describe a useful part of surgery, but it does not prove that the patient is a good candidate, that the donor area is safe, or that the hairline will look natural years later.
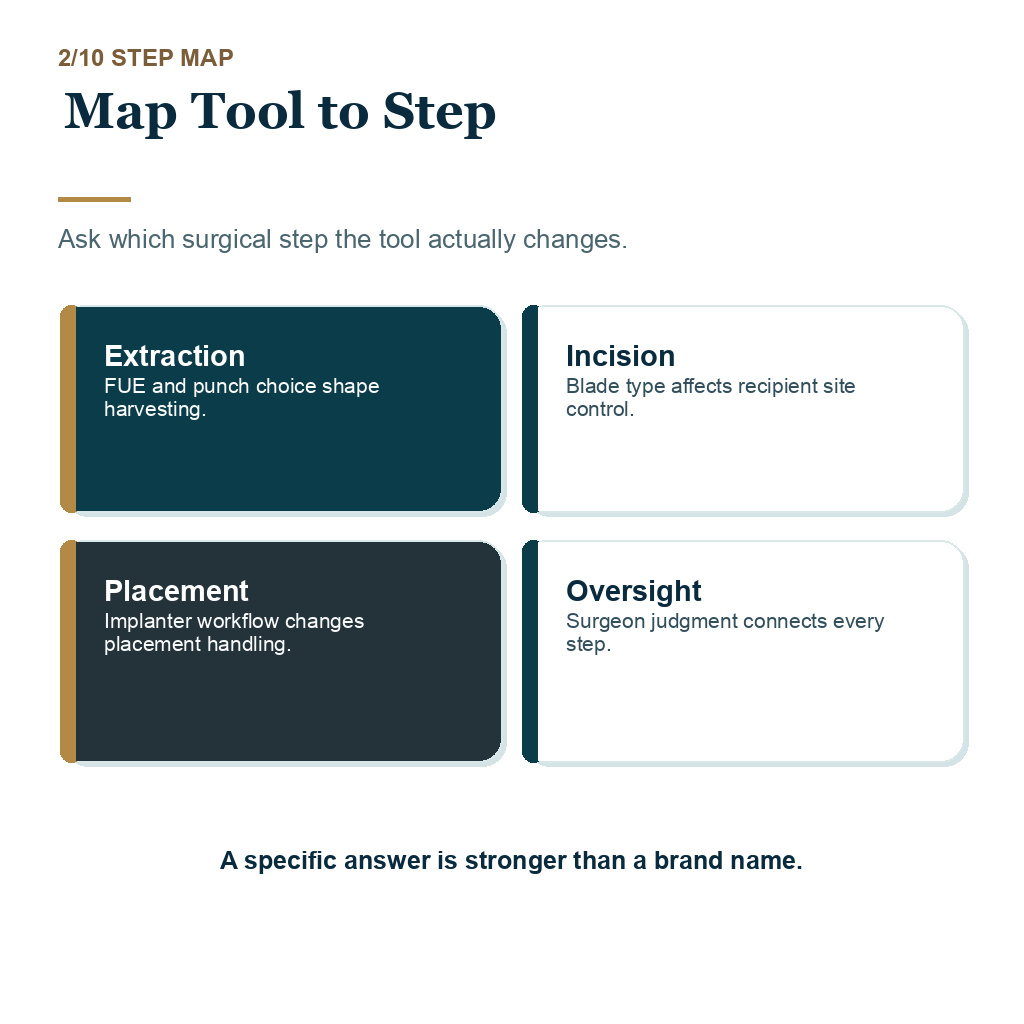
FUE hair transplant is a harvesting approach. Sapphire blades mainly affect how recipient area incisions are made. DHI usually describes implantation with an implanter pen. Robotic systems may assist selected extraction or site creation steps. These can all be useful in the right case, but none of them replaces the surgeon’s judgment.
The mistake is treating the method as the result. A refined instrument used with rushed donor planning, wrong direction, poor graft selection, or a low artificial hairline can still produce a disappointing transplant.
Patient details come before the technique name
The first conversation should be about the patient, not the equipment. I want to understand donor density, hair caliber, miniaturization, skin and hair contrast, curl, scalp quality, age, family history, crown demand, medical background, and whether the goal can be achieved without spending too much donor reserve.
The donor area sets the extraction limit. Graft number planning decides whether the session size matches the surface area. Hairline design decides whether the result belongs on the face as the patient gets older. A clinic that begins with a method before explaining these details is starting in the wrong order.
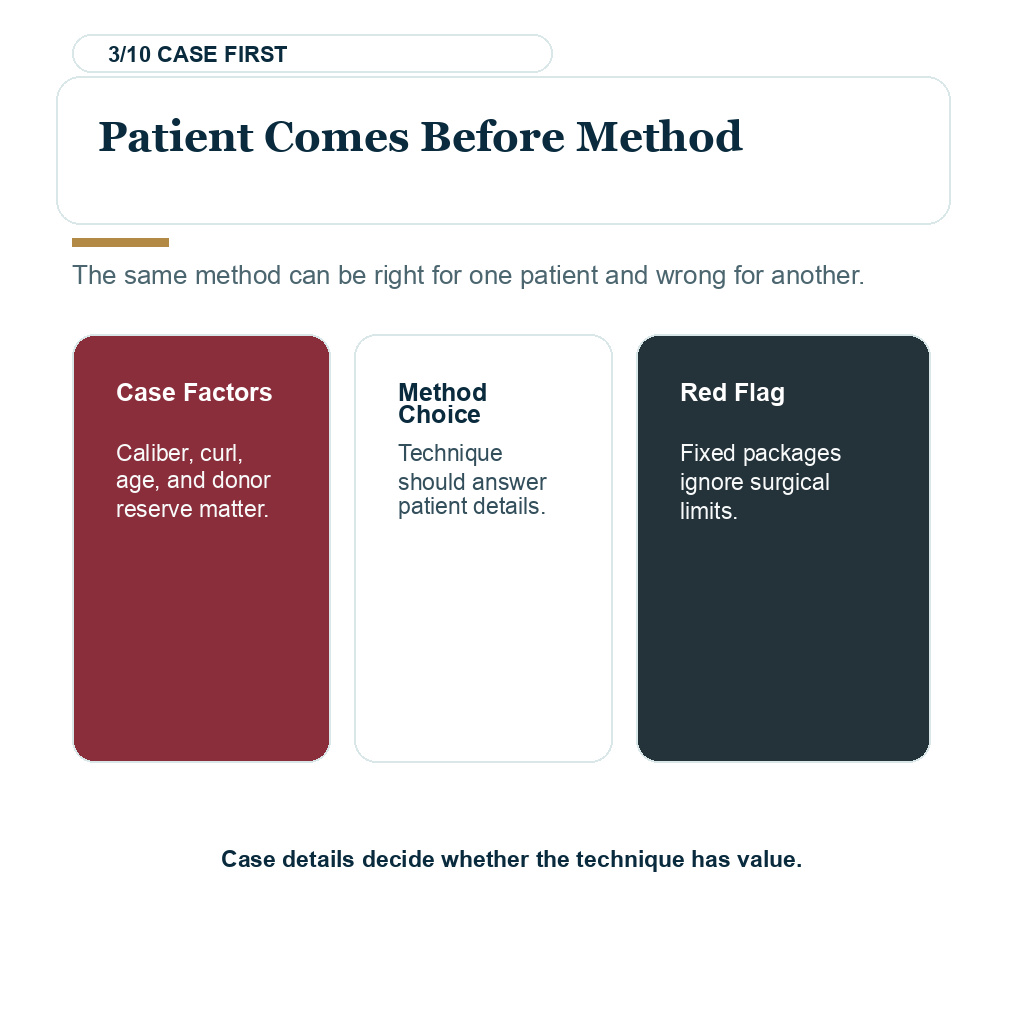
This is also why two patients cannot choose a technique from a menu in the same way. A small frontal refinement, diffuse thinning, Afro textured hair, scar tissue, a weak donor area, and advanced crown loss can all require different handling even if the advertised technique name is the same.
Better questions than which technique is best
A better question is, “Why does this method fit my case?” The answer should connect the technique to your donor area, recipient area, hairline design, hair caliber, planned density, and future hair loss pattern. If the explanation stays at the level of branding, it is not enough.
Ask who examined the donor, who calculated the graft number, who designs the hairline, who creates the recipient area incisions, who supervises extraction, and who protects the grafts while they are outside the body. These questions are more important than whether the clinic uses a fashionable word.
There is a practical price question too. If one clinic offers a basic result with one method and a better result with a more expensive method, ask exactly what medical difference is being claimed. A higher package should not be used to sell the same surgical responsibility under a more impressive label.
Tools genuinely matter during graft handling and placement
Tools matter when they change tissue handling in a real way. Punch choice, extraction depth, incision size, blade sharpness, graft hydration, implantation flow, placement timing, and team coordination can all affect trauma, consistency, and graft survival conditions.
This does not make the tool unimportant. It makes the tool specific. A sapphire blade may help the surgeon create controlled recipient area incisions. An implanter pen may help selected placement workflows. A robotic system may assist selected FUE extraction steps. A smaller or larger punch may change donor scarring risk depending on the hair and skin.
But the tool does not decide donor limits, long-term hair loss planning, hairline height, temple behavior, density priority, or whether surgery should be delayed. That is the practical distinction patients need to keep in mind.
A useful tool improves a defined surgical step. It should not be used to avoid explaining the whole operation.

Surgical decisions still depend on the surgeon
The cosmetic result is shaped before the tool touches the scalp. The surgeon has to decide where the hairline should sit, how soft the first rows should be, which grafts belong in the front, how the angles should follow natural direction, and how much density the skin and donor can support.
Natural hairline design is not created by a blade name. It comes from proportion, age judgment, irregularity, graft selection, direction, and moderation. The same is true for crown planning, temple work, and donor preservation.
The harder question is who performs each surgical step. If the surgeon is not involved in the decisions that frame the face and protect the donor, a modern tool can give false comfort.
Poor planning can create visible thinning in the donor area, a low artificial hairline, weak coverage after an oversized session, or a day one layout that looks impressive but does not age well. The device did not decide those outcomes. The planning did.
Technique marketing becomes a warning sign when it replaces diagnosis
Be cautious when the clinic sells the tool louder than it explains the plan. A clinic that cannot discuss donor limits, surgeon responsibility, graft handling, hairline design, recipient area control, realistic density, and follow-up is not made safer by a modern device.
Turkey is a good example of this confusion. Turkey itself is not the issue, and a technique label is not the solution. The risk comes from poor clinic structure, delegated judgment, rushed volume, and sales promises that hide uncertainty. Those are the situations where hair mill red flags still matter, even when a clinic advertises advanced equipment.
If the clinic avoids clear answers about who plans and performs the key steps, the technique label should not reassure you. The label may be true and still not tell you whether the surgery is being handled responsibly.
Use the 10 tool judgment filter slides below to separate technique labels, surgical step mapping, patient factors, responsibility questions, donor limits, graft handling, hairline design, marketing warning signs, photo context, and the final clinic choice order. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.


Result photos should be compared under fair conditions
Before and after photos are useful only when they are interpreted with context. Baseline hair, lighting, hair length, donor strength, graft count, hair caliber, skin contrast, and follow-up timing all change what the result means.
A tool name under a photo does not tell the full surgical story. A patient with strong donor hair and limited frontal recession is not comparable to a patient with broad thinning, fine hair, unstable loss, or a weak donor reserve. The same method can look excellent in one case and be the wrong choice in another.
When comparing results, I care more about why the plan matched the patient than which label was used. Photos show outcomes. They do not explain the decision making behind them unless the clinic also shows the case context.
Choosing between FUE, Sapphire FUE, DHI, or robotic FUE
Start by removing the technique name from the sentence. If the plan still makes medical sense without the label, the technique can be judged fairly. If the plan becomes vague once the label is removed, you have not been given enough information.
For some patients, manual FUE with careful surgeon control is the best fit. For others, Sapphire FUE may support refined recipient area work. DHI may be useful in selected placement workflows. Robotic hair transplant systems may assist certain technical steps, but they still need surgeon-led case selection and oversight.
At Diamond Hair Clinic, I do not choose a method as a menu item. I choose it after examining the donor area, recipient area, graft number, hairline goal, expectations, and long-term plan. If you are comparing clinics, choosing a hair transplant clinic in Turkey should begin with surgeon responsibility, donor protection, realistic density discussion, and a process that can say no when the request is unsafe.
My practical view is this. Tools can improve surgery when they are used for the right reason. They become dangerous when they are used to replace the conversation about diagnosis, donor limits, hairline design, graft handling, and responsibility. Surgeon judgment turns tools into treatment.