Should a Hair Transplant Look Natural in Harsh Light, Wind, and Wet Hair?
A well planned hair transplant should still look natural in normal daily life, including daylight, office light, movement, and quick styling. But no hair transplant should be promised as if it will recreate teenage density in every harsh condition. Wet hair, direct overhead light, wind, and close phone photos can all make the scalp look more visible.
The important distinction is whether the result only looks lighter in harsh conditions, or whether it looks thin, artificial, lined up, or poorly planned in ordinary conditions too. A mature transplant should not need perfect lighting to look acceptable, but it also should not be judged only by the most unforgiving photo you can create.
Many patients test their result in ways they never used to test their native hair. They wet the hair, stand under a bathroom light, pull the hair apart, take close photos, then compare that image with polished clinic results. That comparison can create anxiety even when the transplant is developing normally.
Transplanted hair can look different when the light changes
Strong light exposes the spacing between hairs. This happens with native hair too, but a transplanted area has already lost original density, so the contrast can feel more obvious.
When light comes from above or behind, the scalp reflects more clearly. When the hair is wet, strands group together and leave wider spaces. When wind moves hair against its usual direction, it can reveal areas that normally look fuller when styled.
That alone does not mean the transplant is weak. Hair is not a solid sheet. Coverage depends on hair shaft thickness, curl, color contrast, recipient area size, and how the grafts were distributed. Those details explain why some hair transplant results look thin even when the graft count sounds reasonable. The color part of that review is covered in blonde and red hair transplant planning, because light and copper tones can change what looks full under unforgiving light.
Before surgery, I look at these details carefully. A patient with thick, slightly wavy hair and low scalp contrast can often create more visual coverage than a patient with fine, straight, dark hair on light skin, even with a similar graft number.
Hair length and styling affect scalp visibility
Hair length and styling can change the result more than patients expect. Very short hair gives less overlap. Wet hair separates into groups. Flat hair exposes more scalp than textured hair. A sharp part line can make one area look weaker than it looks in daily movement.
A result should not be judged from one bathroom light photo. The same scalp can look different with a different haircut, hair direction, styling habit, light source, and distance from the camera. Comb through videos can help only when the hair is shown fairly, not only under the most flattering or most punishing condition.
Styling can make a good result look fuller, but it should not be the only thing holding the result together. If the transplant looks natural only when every hair is arranged perfectly, the original plan may have been too weak, too broad, or too dependent on a favorable photo.
Scalp visibility in bright light does not always mean failure
No. Some scalp visibility in bright light, wet hair, or close inspection does not by itself mean failure. I look at whether the hair frames the face naturally in normal daily situations.
A fair review uses several conditions. Look at the hair dry and wet, styled and unstyled, indoors and outdoors, close up and from normal conversational distance. One harsh photo should not decide the entire result.
The concern becomes stronger when the hair looks transparent in ordinary light, when the hairline looks hard or lined up, when thick grafts are visible at the front, or when the result fails to frame the face after full maturation.
Timing matters as well. At month 4, month 5, or month 6, the hair may still be immature, uneven, or wiry. A six month density check is useful, but it is still not the same as judging a mature result.
Real life durability depends on planning details
The result that holds up best in real life is not the one with the most aggressive promise. It is the one with the best planning.
Planning starts with candidacy, donor strength, hair caliber, scalp contrast, future hair loss, and the size of the recipient area. The donor area is a limited resource, so it should not be spent only to create one impressive photograph.
Hairline design also matters. A low, straight front that seems dense in one angle can look unnatural when the hair moves. A softer transition, correct direction, and irregular distribution usually age better in real conditions.
Direction and angle are not small technical details. If grafts are placed in the wrong direction, the hair may not layer properly. If the frontal zone lacks softness, the eye can notice the transplant even when density is acceptable.
At the front, I want softer grafts with one hair, irregular spacing, and a gradual transition. Behind the first line, stronger grafts can create more body, but they still need natural direction and careful distribution.
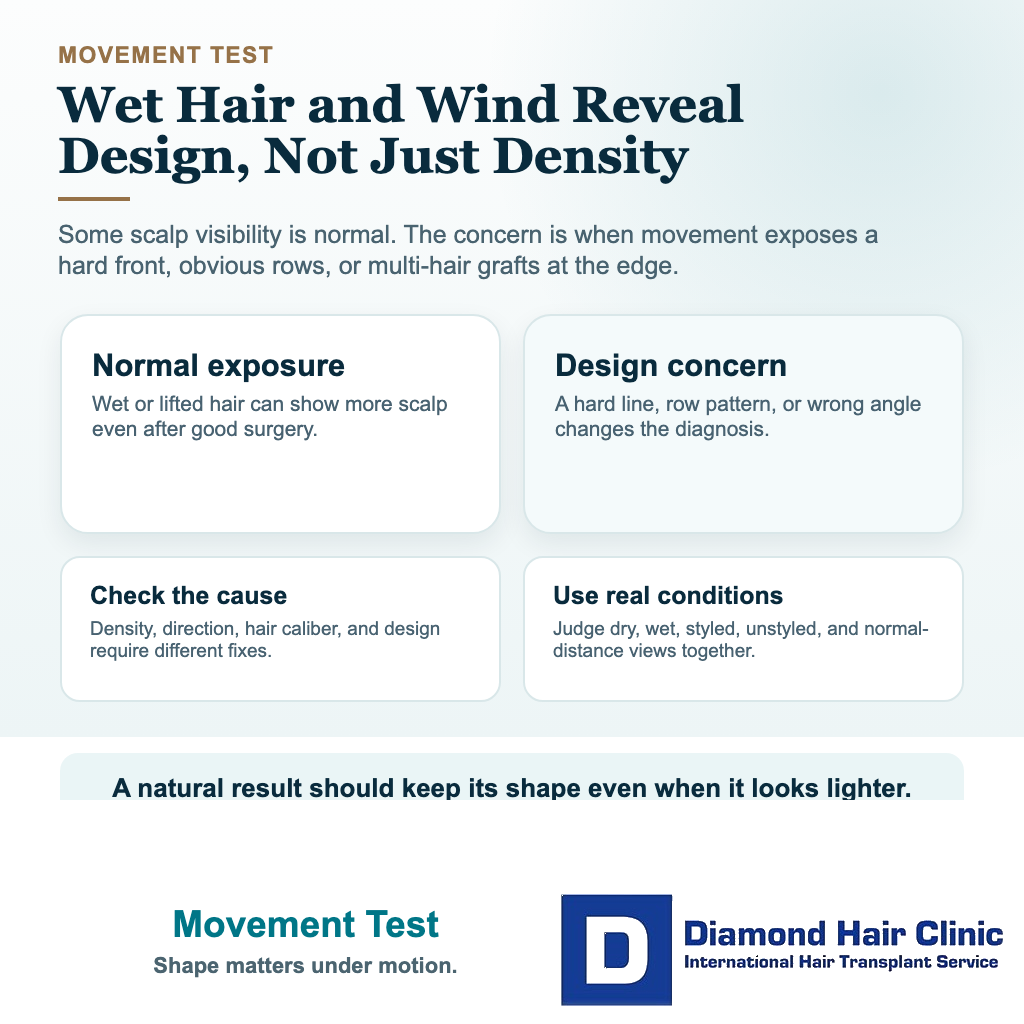
Wind or wet hair can expose a weak plan
Yes, wind and wet hair can expose weaknesses that styled photos hide. Dry hair styled forward can create an impression of density. Wet hair clumps. Wind lifts the hair and removes some control. In those moments, poor distribution, weak angles, low density, or unnatural hairline work can become easier to see.
There is still nuance. A transplant can look slightly lighter when wet and still be a good result. Wet hair always shows more scalp because the strands stick together.
The red flag is a result that loses its natural shape completely when the hair moves. If the hairline suddenly looks like a hard line, if obvious rows appear, or if the front shows thick grafts, the issue is not only wet hair. The issue is design and execution.
At Diamond Hair Clinic, Dr. Mehmet Demircioglu creates the recipient area incisions himself with a sapphire blade. The tool supports precision, but the judgment behind angle, direction, density distribution, and donor use is what protects naturalness.

Hair fibers may still be useful after a hair transplant
Some patients stop using fibers after a mature hair transplant. Some still use a small amount for special situations, especially under strong light or when they want extra cosmetic fullness. Both situations can be normal.
Daily dependence is different from occasional cosmetic help. A small amount of fiber for a photograph, event, or harsh lighting does not prove failure. Needing fibers every day because the transplanted area looks weak in normal light deserves a closer review.
If the patient had advanced hair loss, fine hair, strong scalp contrast, or limited donor supply, a little fiber may improve the cosmetic impression. That can mean the surgery created the best responsible foundation possible while the patient still wants extra styling support.
If the patient cannot leave the house without fibers because the transplanted area looks poor in ordinary conditions, then I want to examine growth, distribution, native hair loss, hairline design, and the promises made before surgery. The decision is different from simply asking when hair fibers can be used after a hair transplant.
Clinic photos can create the wrong expectation
Clinic photos can educate, but they can also mislead when they show only the most flattering version of the result. Dry hair, careful styling, soft light, and a controlled camera angle can make density look stronger than it appears in daily life.
Good documentation shows more than a polished frontal view. Different angles, donor area visibility, harsh light, movement, and result photo context help patients understand what the result really does.
High graft numbers can also create the wrong expectation. A clinic may use a large number to make the result sound dense everywhere, but the donor area has limits. A large number without donor planning can still create a thin or unnatural result.
The difference between a surgeon-led clinic and a high volume model becomes clear here. A result that remains natural for years is more valuable than a dramatic photograph that spends donor reserve too quickly.
Expected thinness and red flags need separation
Thinness can be an expected limitation when the donor area is limited, the balding area is wide, the hair shafts are fine, or the result is being judged wet or under very bright light. The transplant may still be successful if it improves facial framing, looks natural, and preserves future options.
Thinness is more concerning when the mature result looks weak in normal light, when the density is patchy without a clear reason, when the hairline looks artificial, or when the donor area has been overused without producing a strong recipient result.
Be skeptical of a clinic promising full original density across a large balding area in one session. That kind of promise often ignores biology. It may also hide too many grafts used without a safe plan.
Do not judge the result only by how many grafts were moved. Judge how intelligently the donor was used, how natural the front looks, how stable the plan is, and how the hair behaves in real life.
Use the 10 real life result check slides below to separate harsh light, wet hair, wind, hair length, normal distance, fibers, clinic photo bias, repeated red flags, waiting before another surgery, and what evidence to send for review. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.