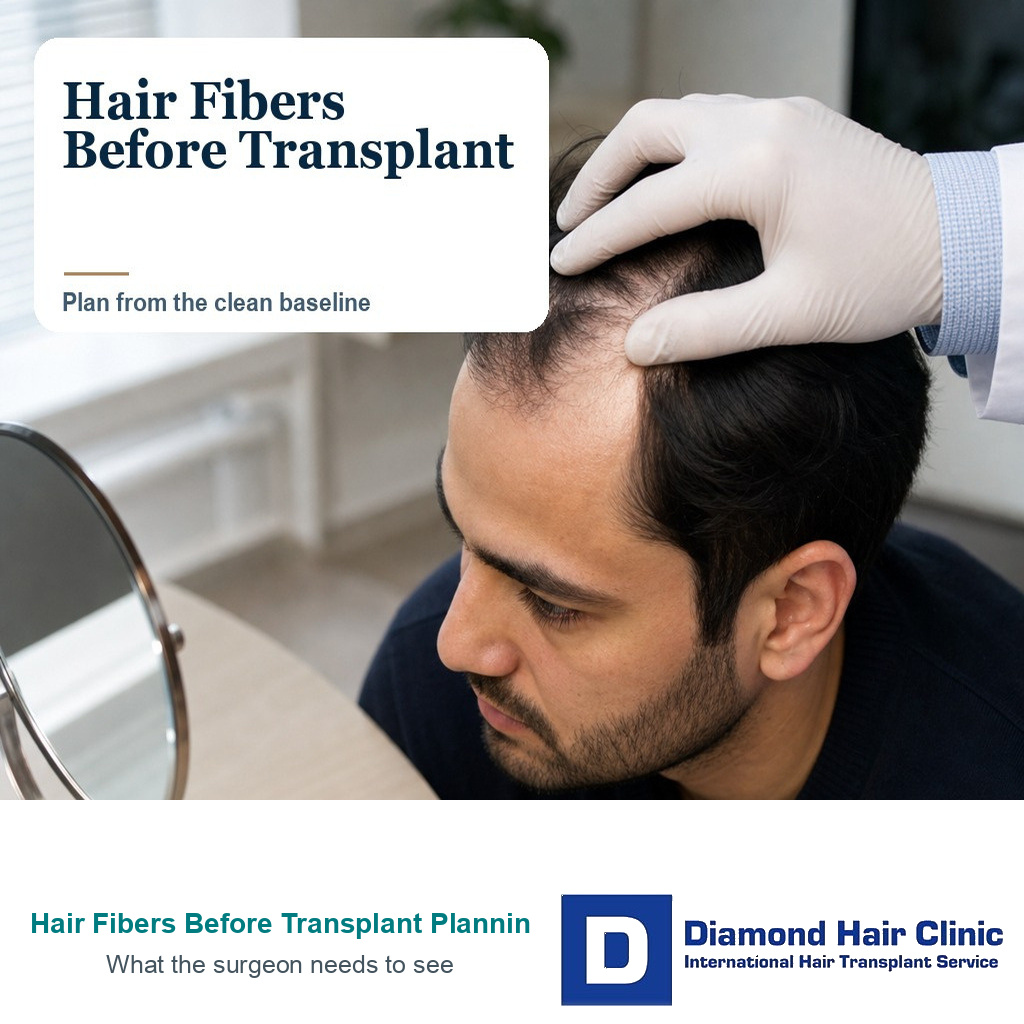
Hair Fibers Need a Clear Plan Before Surgery
If you use hair fibers or scalp concealer before a hair transplant, remove them for your consultation photos, scalp examination, surgical planning, and surgery day. Fibers can help you feel more comfortable socially, but they are not a reliable baseline for surgery. Clinically, they can hide the real amount of thinning, make the donor plan look easier than it is, and make the cosmetic darkness from fibers feel like a realistic transplant target.
Fiber use is not the problem. People use fibers to work, travel, date, or appear in public without feeling exposed. For surgical planning, I still need clean, dry hair without product, and sometimes wet or parted photos, not a cosmetic effect that disappears after washing. This includes root sprays, tinted powders, dry shampoo, thick styling paste, and dark scalp concealers, not only classic hair fibers. A similar rule applies to hair dye before hair transplant because color should not leave residue or irritation that confuses the scalp check.
Hair fibers can change the consultation
Hair fibers work by adding color and texture around existing hair shafts. That can reduce the contrast between hair and scalp very quickly. For daily life, this may be useful. For surgical planning, it can become misleading because the clinic needs to see what is actually present.
There is a practical difference between using fibers socially and using fibers as evidence for surgery. Two photo sets can both be useful, but they must not be mixed. A styled photo can show how you normally present yourself. A clean photo, taken before a very short haircut before surgery when possible, shows what I must plan around. If those two pictures tell very different stories, the clean picture has to control the medical decision.
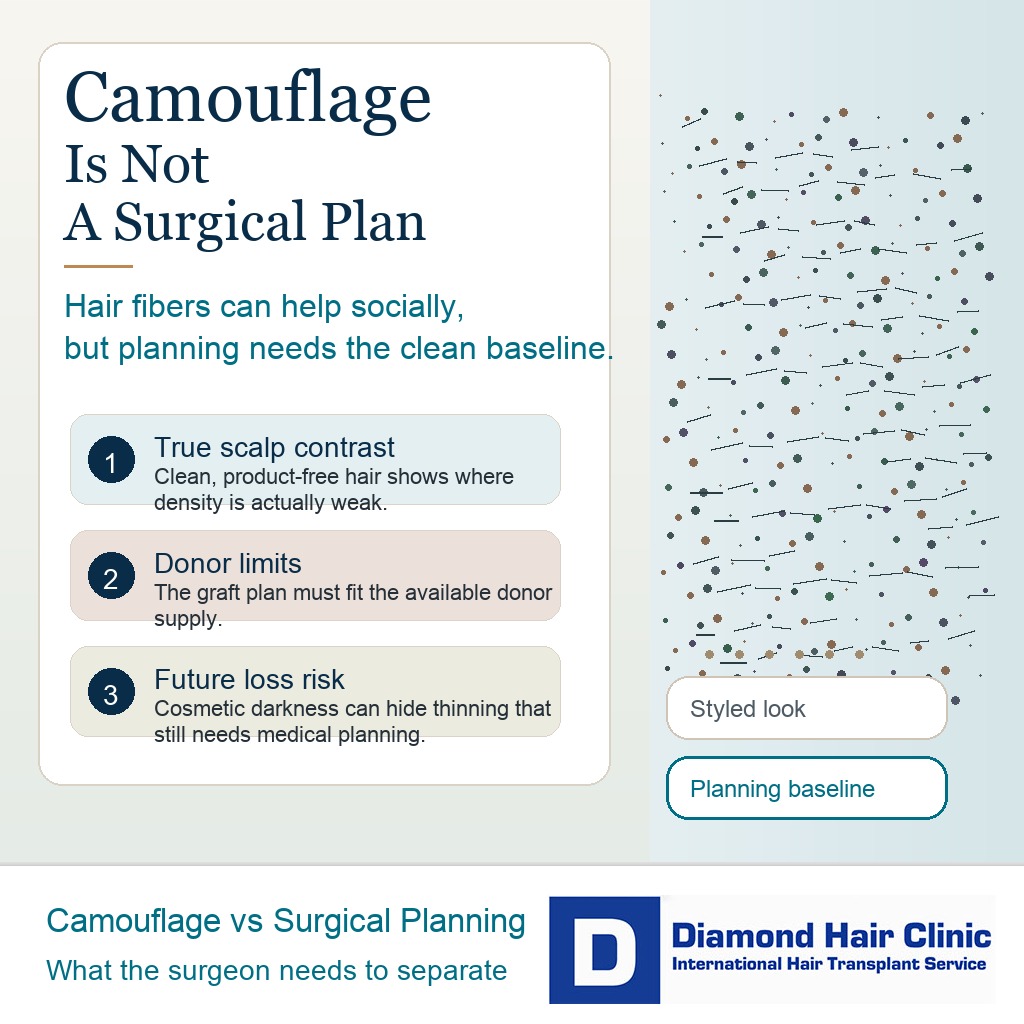
Cosmetic darkness can hide scalp contrast, but surgery has to work within donor limits and future hair loss risk.
If the front looks denser with fibers, the plan may underestimate how much native hair is weak. If the crown looks darker with concealer, the area may seem to need only a small touch. If the middle scalp is covered well in normal lighting, diffuse thinning may be missed unless the hair is parted and photographed clearly.
A hair transplant is planned around real hair caliber, real scalp visibility, donor capacity, and future hair loss. Fibers can improve the appearance for a few hours, but they do not change the number of stable hairs available for the long term.
The surgeon needs clean scalp and hair evidence
The surgeon needs to see the scalp the way it behaves without cosmetic support. That means the true hairline shape, the caliber of the existing hairs, the density behind the hairline, the crown pattern, the donor area, and any redness, scaling, irritation, or inflammation on the scalp.
That distinction can change the plan. A frontal forelock that seems strong with fibers may actually be fragile miniaturized hair. Hair that looks thin in photos may still have strong caliber that can create better visual coverage after careful planning. The difference cannot be judged from a darkened surface alone.
For remote assessment, hair transplant planning photos should show the hair dry, wet or slightly damp when requested, parted in several directions, and taken under direct light. If fibers are part of daily life, send one styled set only as a clearly labeled social or styling reference. The medical planning set must be clean, and it should control the surgical decision if the two sets differ.
Clean views without product give the surgeon a more reliable baseline than cosmetic density.
Fibers can make density expectations unrealistic
Fibers can create a dark, matte surface that makes the scalp less visible than real hair alone can achieve. A transplant adds living follicles, but it does not paint the scalp. If you compare surgery to a heavy fiber result, the plan can become too optimistic.
This is especially relevant for patients who judge their hair in harsh bathroom light, wet hair, wind, or close phone photos. Hair transplant results in harsh light and wet hair can look different from mirror or social photos. Fibers can push that contrast even further because they darken the background and hide the spaces between hairs.
The surgical plan should aim for natural coverage, age appropriate framing, and donor preservation. It should not chase a cosmetic shadow that only exists while powder is sitting on the hair shafts and scalp.
Stop fibers before medical planning photos
For medical planning photos, yes. Wash the product out and send at least one clean set after the hair is fully dry. If residue still darkens the scalp, repeat the wash and explain that product may still be present. The clinic should also know how often you use fibers, where you apply them, and whether you need them only in the crown, the frontal third, the middle scalp, or almost everywhere.
The most useful photo set does not need to look flattering. It needs to show the scalp clearly. Take photos from the front, both temples, top, crown, donor area, and side profile. Part the hair where the thinning is strongest. If you normally style the hair forward, also show the hair lifted. A short comb through video in direct light can be useful because it shows whether density changes when the hair moves. If you have long hair, separate the strands enough to show the scalp below.
A styled photo can still be useful, but label it clearly as styled with fibers. It should not sit beside clean photos as if both sets show the same medical baseline. It is better to see the problem clearly at the beginning than discover on surgery day that the clean scalp tells a different story.
Send a clean set if earlier photos used fibers
If you already sent consultation photos while wearing fibers, do not treat that as a serious mistake. Send the clinic a note and provide a second clean set before the surgical plan is finalized. The important issue is whether the hairline, middle scalp, crown, and donor area were judged from a cosmetic effect rather than the real scalp.
The clean set should show the same angles as the original photos so the difference is visible. If the clinic changes the graft estimate, hairline design, or timing after seeing the clean scalp, that is useful information. Revised planning after clean photos is usually safer than pretending the fibers were not there.
Dependence on fibers changes privacy planning
It can feel hard to leave the house without fibers. Over time, camouflage can start to control haircuts, rain exposure, gym sessions, trips, hotel stays, and social events because every situation becomes a question of whether the scalp might be seen. That pressure is real.

Surgery may help you move away from daily camouflage, but it should not be sold as a complete escape from every styling concern. A transplant result still has limits under wet hair, strong light, short hair, and progressive native hair loss. If you currently need a thick layer of fibers to feel normal, the consultation must separate what surgery can realistically improve from what the cosmetic darkness has made you expect.
If privacy during recovery is a major concern, read about keeping a hair transplant secret because the early visible phase after surgery is different from the daily concealment that fibers provide.
Fibers can hide diffuse or unstable thinning
They can. Diffuse thinning is often harder to plan than a clear receding hairline because the surgeon must decide whether the native hairs are strong enough to work around. If fibers hide visible scalp across a wide area, the case may look like a local density problem when the real issue is active thinning.
A clean examination matters especially in diffuse thinning and hair transplant surgery. The surgeon must ask whether the diagnosis is stable, whether medical treatment is needed first, whether the donor area is truly strong, and whether placing grafts between weak native hairs creates a poor balance between risk and benefit.
If the pattern is still moving quickly, surgery can place islands of transplanted hair into a landscape that keeps changing. Delay surgery if the diagnosis is unclear or if the native hair is still losing ground too aggressively.
Hairline and crown planning need clean baselines
Fibers can make the hairline look softer and fuller than it is. They can also make the crown look smaller than it really is. Both can pull the plan toward the wrong priority.
For the hairline, the surgeon needs to see where single hair grafts will be needed, where native hairs are still useful, and how low the design can safely sit as you age. A darkened frontal area can make a lower or denser line feel reasonable even when the donor supply cannot support it long term. The principles of hairline design in hair transplant surgery must be based on anatomy, age, facial frame, donor supply, and future loss, not on how the area looks after cosmetic powder.
For the crown, fibers can create a rounded dark zone that looks easy to fill. In reality, crown work can consume many grafts and still look lighter under strong light because the whorl opens in several directions. If you are considering a crown hair transplant, the crown is often a donor budget decision, not only a cosmetic target.
Surgery day planning starts with hair without product
Before surgery day, the final plan should be reviewed with the hair clean. The hairline design, recipient area, donor area, graft priorities, and any areas that will be left for future planning should be clear. Ask when to stop fibers, root sprays, concealer, dyes, or heavy styling products before arrival, because residue can stay on the scalp, pillow, or hair shafts longer than expected. If fibers have been part of your daily routine, tell the clinic instead of pretending you never use them.
The clinic may ask you to wash your hair before surgery and avoid styling products. Follow the exact instructions from the surgical team. Arriving with residue on the scalp can make the examination harder, interfere with clear marking, and may create unnecessary cleaning or timing problems before the procedure begins.
If fibers, sprays, dyes, or scalp products have caused itching, redness, scaling, soreness, or small irritated patches, mention that before surgery. Share the product type, where you apply it, how long the reaction has been present, and whether scratching or washing makes it worse. Washing the product out may remove the cosmetic layer, but it does not answer by itself whether the scalp is settled enough for surgery.
Most importantly, do not let embarrassment hide information from your surgeon. If you depend on fibers because the middle scalp is visible through the hair, say so. If the crown looks acceptable only with concealer, say so. If you are using fibers to cover weak donor areas or older scars, say so. Hidden information can lead to a weaker plan.
These 8 hair fiber planning slides separate the clean baseline, photos without product, product types, donor visibility, wet or parted photos, stop timing, waiting after surgery, and what to tell the clinic. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.