


2000 Grafts for Hair Transplant Coverage
2,000 grafts can be enough for a hair transplant when the goal is a focused hairline, temple, or frontal area improvement. That amount is usually not enough for full hairline, mid scalp, and crown coverage together. The number only becomes meaningful when it is tied to a real plan. The area, donor strength, hair quality, density goal, and future hair loss risk have to make sense together.
Two thousand grafts do not create a result by themselves. They are a limited amount of donor tissue. Used in the right area, they can build a strong frontal frame. Spread across too much scalp, they can grow and still look thin. That is the practical distinction to understand before comparing quotes.
In consultation, I first define what the surgery needs to achieve. It may be rebuilding a hairline, softening temple recession, adding frontal density, touching a small crown, or trying to cover everything from front to back. For a natural frontal frame in a suitable patient, 2,000 grafts may be very reasonable. For complete coverage from front to crown, that is not a realistic 2,000 graft goal.
2000 graft target compass
Four checks before trusting a 2000 graft plan
A 2000 graft offer is only useful when the target is clear. The same number can mean focused front work, weak broad coverage, or a plan that needs staging.
Area size
How large is the target area?
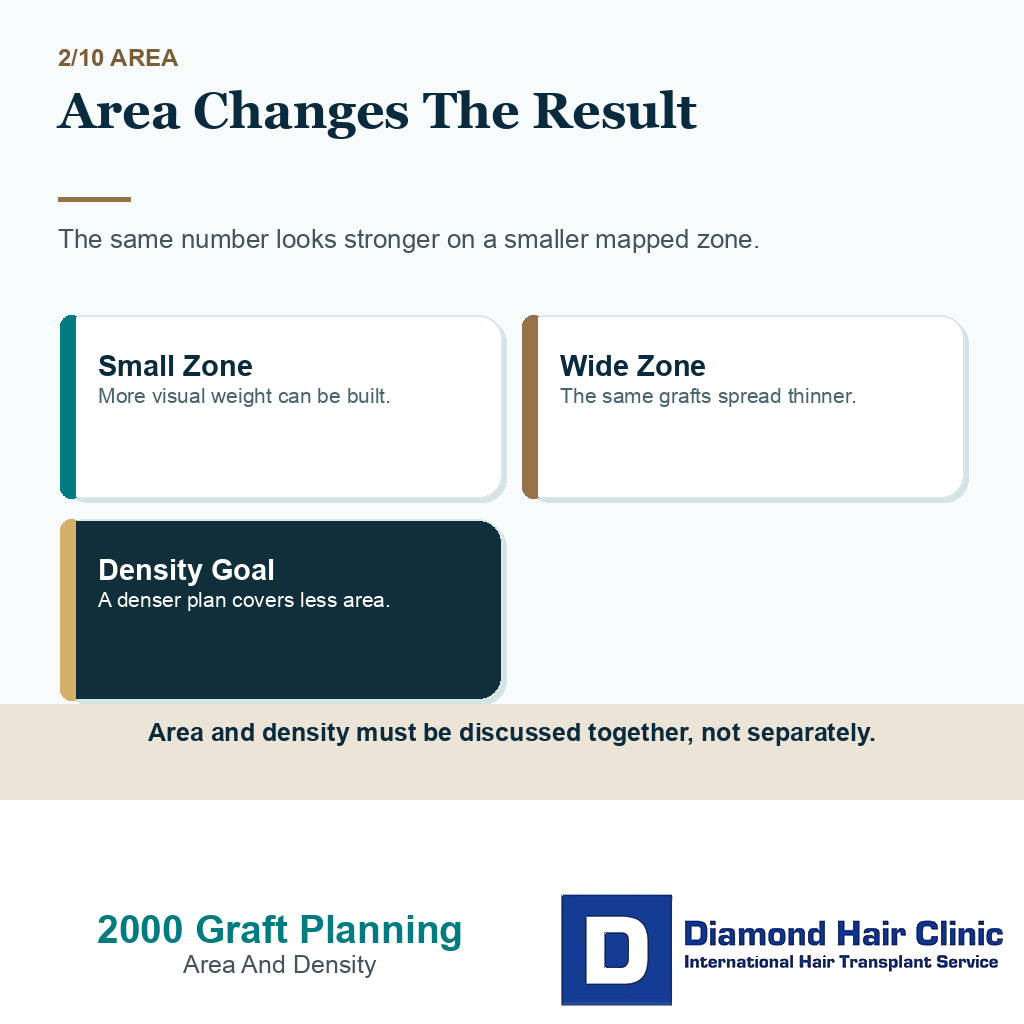
The same graft number behaves differently on a small frontal zone and a broad thinning pattern.
Sometimes, but only for a defined goal. The target area, hair quality, and density expectation decide the answer.
Use this as a planning frame, not a diagnosis or approval for surgery. The final plan still depends on donor reserve, recipient area anatomy, hair type, medical history, and future hair loss risk.
Realistic coverage depends on area and density
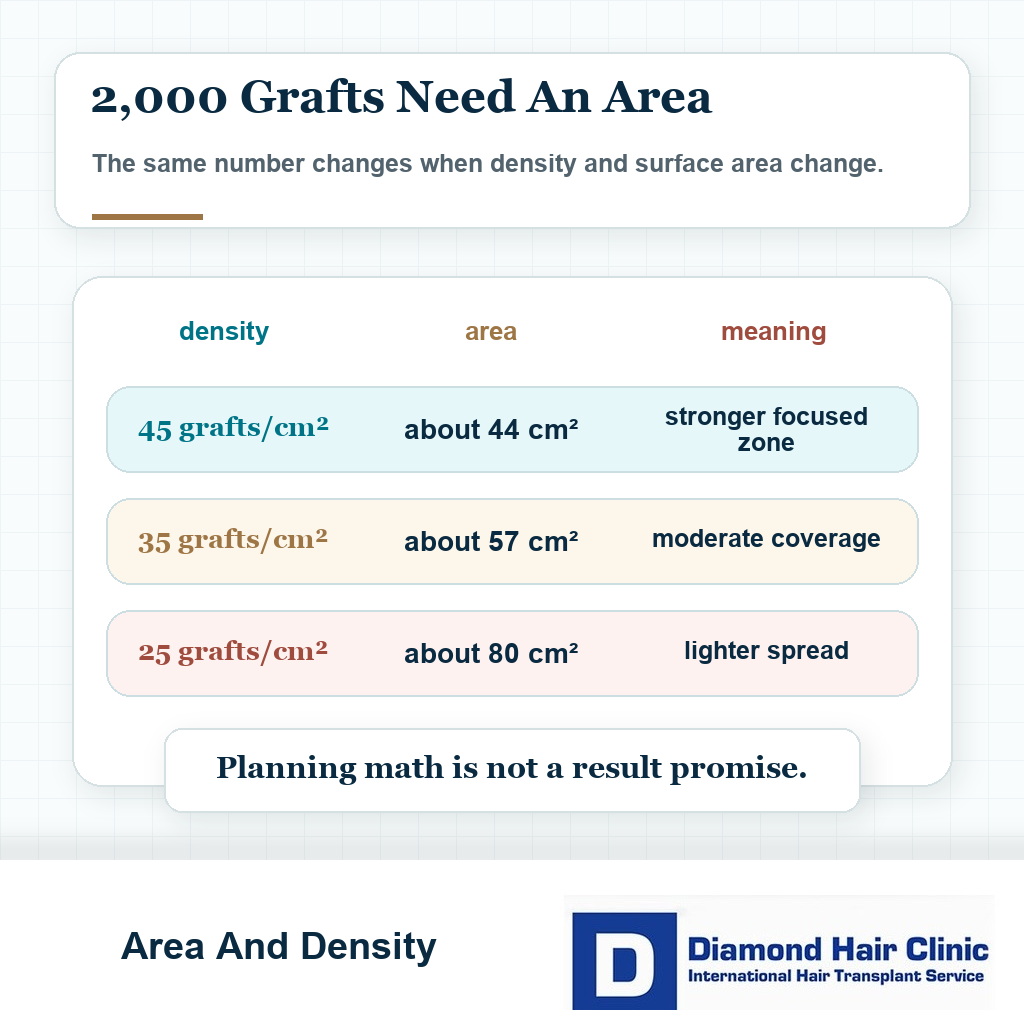
The practical way to understand 2,000 grafts is to connect the number to area. If 2,000 grafts are placed at about 35 grafts per square centimeter, they cover about 57 square centimeters. If they are placed at about 45 grafts per square centimeter, they cover about 44 square centimeters. If they are spread at about 25 grafts per square centimeter, they cover about 80 square centimeters, but the density will look lighter.
These figures are useful for planning, but they are not a promise. A stronger density across 44 square centimeters and a lighter density across 80 square centimeters will not look the same. Hair shaft thickness, graft quality, the number of hairs inside each graft, skin contrast, angle, curl, and native hair all change the visible result.
I use density differently from zone to zone. The first hairline edge needs softer single grafts and careful irregularity. The area behind it may need stronger visual weight. The crown needs a different strategy because light reflects differently and the hair turns in a spiral pattern.
If the area is too large, ambition does not create more grafts. It only asks the same grafts to do a job they cannot do well. You may still see growth, but the result can feel thin because the plan was stretched too far.
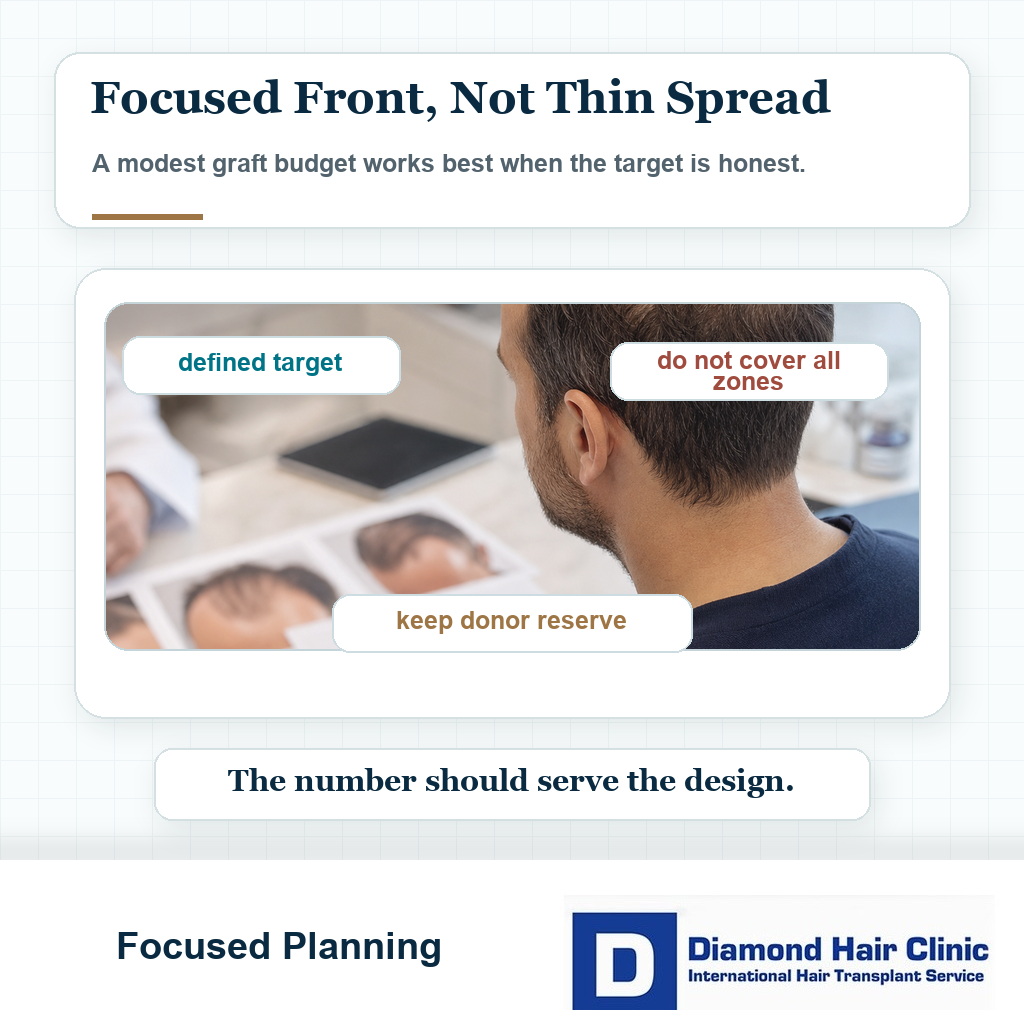
For 2,000 grafts to be enough, the target must stay focused. The number can be excellent when it is used for a clear priority and disappointing when it is used as a package answer for too much scalp.
Treating the front can be enough in selected patients
Treating the front can be enough when the hair loss is limited, the donor area is strong, expectations are realistic, and the goal is clearly defined. A common example is someone with mild to moderate temple recession who needs the frontal frame rebuilt without chasing every weak area on the scalp.
It can also be enough when there is useful native hair behind the hairline. In that case, the grafts do not need to create every bit of coverage from zero. They need to restore the front in a way that blends with what is already present.
Hair quality matters. Thick, wavy, darker hair can create stronger visual coverage from the same graft count than fine, straight, light hair. Scalp color, hair color, hair shaft thickness, and styling length all change the result.
A narrow recession with strong hair characteristics may improve meaningfully from a focused procedure. Broad recession, weak donor density, fine hair, and crown thinning need a very different conversation.
The number has to be connected to the plan. The broader method behind how a surgeon calculates graft number is simple in principle. The same number can be excellent, weak, or risky depending on how it is used.
A well planned smaller procedure can be better than a larger operation that spends grafts without a clear visual strategy. A smaller 1,000 graft plan can be the better plan when it protects the donor area and creates the right visual effect.
The plan falls short when the area is too large
The plan starts to fall short when you want strong coverage across the hairline, mid scalp, and crown in one session. The surface area is simply too large to create dense coverage everywhere with a limited graft budget.
I see this misunderstanding often. Someone hears a graft number and imagines a full head of hair returning. But a graft has to be placed somewhere. If the area is too wide, the same number becomes spread out, and the final result may look thin.
2,000 grafts are not a bad number. The mistake is asking them to behave like 4,000 grafts. That is when a quote can sound precise while the visual plan is still weak.
The plan may also be too small if the hairline is being lowered aggressively. A low hairline consumes many grafts because it creates a larger recipient area. The lower the line, the more grafts are needed just to build the front.
It may be too small in advanced baldness. If someone has lost a large frontal area and also has crown thinning, surgery can create improvement, but not the full correction the patient is imagining.
It may also be too small if the donor hair is fine. Fine hair gives less coverage per graft, so fine hair transplant planning has to be judged differently from thick hair planning.
The concern goes beyond a thin looking result. You may spend donor grafts without solving the main cosmetic problem. Once grafts are used, that donor reserve is smaller.
A graft number without a clear treated area should make you pause. If there is diffuse weakness across the top, the number may sound precise but the target may be vague. Surgery works best when the surgeon knows exactly which zones are being improved and which zones are being protected for later.
Another weak point is expecting the same result at every length and in every light. Careful frontal work may look very helpful when the hair is styled well, but it may not erase scalp visibility under harsh light or when the hair is wet. That expectation should be explained before surgery, not after.
These 10 slides show what 2000 grafts can and cannot cover when donor reserve is limited. Swipe across the image, use an arrow, or pick a number below the carousel.

Hairline rebuilding depends on design and donor control
The hairline can be rebuilt well in the right case. This is often where a modest graft budget makes the most sense. The hairline frames the face, and careful frontal work can create a strong cosmetic improvement without using every available donor graft.
The key word is focused. If the grafts are used to rebuild temples, soften recession, and restore the frontal outline, the result can be natural and satisfying. If the same grafts are asked to lower the hairline dramatically and fill a broad area behind it, the plan may become too thin.
A natural hairline depends on more than density. Height, shape, irregularity, graft selection, direction, and facial balance decide whether the line looks natural. A dense but badly designed hairline is not a good result.
Natural hairline design in hair transplant is where each graft has to earn its place. The surgeon must know where the grafts give the most value.
If you are young, the hairline needs even more caution. A very low hairline can look exciting at first, but it may age badly if the native hair behind it continues to thin. The first surgery should not trap you into needing several difficult corrections later.
With a focused graft budget, a mature and well placed hairline is often wiser than a dramatic low line. The purpose is not to draw the youngest possible hairline. It is to create one that still makes sense in the future.
Crown coverage needs especially careful planning
A smaller session can improve a small or moderate crown, but it rarely creates dense crown coverage if the crown area is large. The crown is one of the most demanding areas of the scalp for grafts because hair direction changes, light reflects strongly, and the whirl pattern can expose scalp even when grafts grow.
The crown is easy to underestimate. It can look like a simple round thinning area, but in practical terms it can consume a large number of grafts while giving a softer visual change than the frontal hairline.
A small crown touch can soften contrast. That is different from trying to rebuild a broad crown densely. If the crown is broad and the front is also weak, using the whole session only in the crown may not be the best first priority.
Crown hair transplant planning has to be conservative and direct because the crown should not be judged like a simple empty circle.
Often, the frontal frame gives more visible value than the crown. The crown can matter, but the donor supply must be used where it changes appearance most responsibly.
If both the hairline and crown are weak, a staged plan may be safer. A first session may restore the frontal frame, while the crown is reassessed later. The decision around hairline or crown first in a hair transplant becomes especially important when the graft budget is limited.
It can be disappointing to hear that the crown needs to wait. The crown can carry a lot of emotion because it appears in photographs and under overhead light, but emotion cannot decide the donor order for us.
If 2,000 grafts are placed into a large crown, you may see new hair and still feel uncovered. If the same grafts restore the frontal frame in the right case, the visible improvement may be much stronger. This is the kind of judgment that must happen before the graft count is accepted.
Different estimates often describe different plans
Clinics give different estimates because they may not be planning the same result. One clinic may be planning only the hairline. Another may be including the frontal area and mid scalp. Another may be promising crown coverage as well.
The number is what people hear first, so the lower quote can feel too cautious and the higher quote can feel more generous. I do not assess it that way. I ask what each number is meant to do.
Different clinics also evaluate donor safety differently. Some plans are conservative because they protect future options. Others are aggressive because a bigger number sounds more attractive when someone is comparing offers.
Number shopping can be dangerous. The more exciting quote may still be the weaker plan if nobody explains the treated area, density plan, graft distribution, and donor risk.
This is the real reason hair transplant graft numbers differ. The estimate is not meaningful unless the clinic explains the design behind it.
If one clinic says 2,000 and another says 4,000, do not ask only which is correct. Ask what each clinic is planning, what will be left untreated, and what the donor area will look like afterward. A middle estimate can also be reasonable in some cases, so read 3,000 grafts for a hair transplant as a plan, not just a larger number.
Hair quality changes how coverage looks
Hair quality can change the whole visual result. The same graft count in thick, coarse, wavy hair can create more visible coverage than it would in fine, straight hair. The number is the same, but the optical effect is different.

Hair color and scalp color also matter. Dark hair on light scalp shows more contrast. Light hair on light scalp can look fuller with the same density because the contrast is lower.
Curl and wave can help coverage because the hairs occupy more visual space. Straight fine hair may separate more easily and show scalp more easily, especially under bright light or when wet.
Fine hair can still benefit from a smaller procedure. The point is that the plan must be more precise, and the expectation must be more realistic.
I check graft composition. A graft may contain one hair, two hairs, or more. Two people with the same graft count may not receive the same number of hairs. That is one reason the graft number alone cannot predict the final look.
You may see a quote. I need to see the biology behind it. Hair thickness, graft quality, donor density, and the recipient area all decide what the surgery can accomplish.
Hair direction matters as well. If the grafts are placed at the wrong angle, even a reasonable number can look artificial or less dense. Good density is not just a matter of how many grafts are present. Natural direction and layering decide how well they lie together.
Technical execution and artistic planning have to be judged together. A procedure of this size can look strong when the grafts are used intelligently. The same number can look weak when the plan ignores hair characteristics or when the grafts are distributed without priority.
Donor protection should be visible in the plan
You judge it by asking what will be removed, where it will be removed from, and what will remain for the future. Once a follicular unit is removed, that exact unit does not grow back in the donor area.
A smaller number is not simply safe, and a larger number is not simply unsafe. The safety depends on donor density, extraction pattern, hair shaft thickness, scalp contrast, age, future loss, and whether you may need another session later.
The donor area in hair transplant must be evaluated before any number is approved. Someone with strong donor density may handle a focused session easily. Someone with weak donor density may need a much more cautious approach.
The number also needs to protect future correction. If the first surgery uses grafts without clear priorities, you may later need more coverage but have fewer safe grafts available over your lifetime.
Good donor management is more than avoiding visible overharvesting. The real goal is preserving options. A plan can look acceptable today and still be weak if it ignores what you may need in five or ten years.
A smaller session still needs the same seriousness and precision as a larger one. It needs the same seriousness and precision as a larger one.
A smaller session can still harm the donor area when the extraction plan is careless. If grafts are taken from the wrong zone, taken too close together, or taken from a donor area that is already weak, the long term cost can still be real.
Donor protection depends on more than the number removed. Pattern, spacing, safe zone judgment, and whether the remaining hair can still camouflage the extraction all matter. This is especially important for patients who prefer shorter haircuts.
A bigger number still needs donor justification
A bigger number may be correct if the treated area is larger and the donor area can safely support it. But a bigger number can also be a marketing tool if it is offered without diagnosis, donor measurement, and a clear design.
It is natural to feel safer with the bigger number because it sounds like more value. But in hair transplant planning, more is not always better.
Too many grafts in one area can increase tissue trauma, waste donor supply, or create an unnatural design if the plan is not balanced.
A larger number can also hide a poor strategy. If a clinic says 5,000 grafts but cannot explain the hairline, crown priority, donor safety, and future plan, do not let the number impress you.
A smaller number can also be wrong. If you clearly need broader coverage and the clinic recommends a limited plan only to keep the price lower or the operation simpler, the result may disappoint you.
The right number is the number that fits your case. It is not the biggest number and not always the smallest number. It is the number that belongs to a responsible plan.
Reading a 2,000 graft quote carefully
Start with the treated area. Hairline only is very different from frontal area plus mid scalp. Crown included is a different plan again.
Then look at the density promise. Do not accept vague promises like full coverage if the area is broad. You need to know what may still look thin, what will be left for later, and what the result should look like in normal lighting.
It is also important to understand why the estimate was chosen. That means the donor area was examined, miniaturization was considered, future loss was discussed, and medication was reviewed when native hair is still weakening.
A proper consultation also needs to decide whether you are a good candidate for hair transplant. You can want a smaller operation and still not be ready for surgery if the diagnosis, donor area, or expectations are poor.
The plan also needs to leave room for a second procedure if one may be needed. A focused first surgery can be wise, especially if it protects the donor reserve. But you need to know whether the surgeon sees the case as one stage or part of a longer plan.
Surgeon led planning matters here. The person designing the plan must understand donor management, hairline design, recipient area strategy, and future progression. Otherwise, the graft number becomes a package size instead of a surgical decision.
Ask what would make the surgeon change the plan on the day of surgery. Sometimes the donor looks different after trimming. Sometimes graft quality, density, or miniaturization changes the safest approach. A real surgical plan has room for judgment.
When the answer is that the number is fixed no matter what is found, be careful. Hair transplantation is not a transaction for a promised quantity alone. It is a medical and aesthetic decision made on living tissue.

Judging the result after surgery
After surgery, do not judge a focused result too early. For the frontal area, 12 months is often a fairer point for judging the mature cosmetic result. For the crown, maturation can take up to 18 months.

At four or five months, a result can look thin even when growth is still developing. At six or seven months, some improvement may appear, but the final texture, thickness, and coverage are not mature yet.
Still, timing does not solve every problem. If the grafts were spread across too large an area, the result may remain thinner than you expected even after growth matures. That is not a growth problem. It is a planning problem.
If the first session was focused and direct, a second session may later make sense. Whether a second hair transplant is worth it depends on visible need, donor reserve, and whether another procedure improves the plan without weakening the future.
Judge the result against the plan that was actually made. A focused operation can be enough when the donor is respected and you understand what the grafts can realistically achieve. It is not enough when it is used to promise full coverage across a problem that needs a larger or staged plan.
If you are deciding between a conservative quote and a higher quote, do not choose by number alone. Choose by diagnosis, design, donor safety, and clear explanation. That is what protects the result.
That is the result I am trying to protect for you. Not the number that sounded most impressive in a message, but the plan that still looks natural after growth has matured and still leaves the donor area healthy for the future.