



Hairline or Crown First in Hair Transplant Planning
If both areas need work and donor hair is limited, I often prioritize the hairline and frontal middle scalp before the crown. The front frames the face and gives the strongest visible return for each graft in many patients. The crown can still matter deeply, but it often needs careful timing, medical stabilization, and sometimes a second session after 12 to 18 months when the first result can be judged properly. A 3,000 graft plan must have a clear priority before surgery begins. For patients between early recession and advanced loss, Norwood 4 or 5 hair transplant planning shows how that priority fits the full graft budget.
The crown should not be ignored. If the front is already stable, donor supply is strong, and the crown is small and clearly defined, crown work can move higher in the plan. The mistake comes from allowing the crown to consume donor grafts before the facial frame and future options have been protected. The same donor protection logic matters during a hair transplant in your 30s.
In consultation, I do not ask only where you are bothered today. I ask where the donor hair will create the most natural and stable improvement over time. The crown may be the emotional priority, while the front may still be the surgical priority. I discuss that difference directly.
Front often deserves protection before the crown
The frontal area is the part of the scalp most people see first. It frames the face, changes the shape of the forehead, and affects how a person looks in conversation, photographs, and normal social life. A natural frontal result can make the whole face look more balanced even if the crown is still thinner.
The hairline should not be treated as a simple line to be lowered. It is a surgical design decision that must respect age, facial proportions, temple shape, hair direction, donor limits, and future loss. A patient who wants the front treated first still needs to understand natural hairline design in hair transplant before approving any plan. The same restraint applies to Norwood 3 front corner planning before deciding how much donor hair needs to stay in reserve for the crown.
The crown is different. It is usually judged from above, behind, or in overhead photos, and the crown whorl changes how light exposes the scalp. It can bother the patient very deeply, but it does not frame the face in the same way. That difference matters.
The frontal third often gives more cosmetic value for the grafts used. If I spend too many grafts in the crown too early, I may weaken the ability to create a strong front later. That is not a small mistake. It can affect the result for life.
That same tradeoff can appear after the first operation too, when the front looks acceptable but the top still needs a second transplant plan for a thin top.
Crown planning that begins with a number only needs to slow down. The front, middle scalp, crown, and donor reserve have to be planned as one lifetime graft plan. The crown itself needs its own careful logic, which is why crown hair transplant planning cannot be treated as a simple extra step.
You may say the crown bothers you more because you see it in photos from behind. That feeling is real. But the most emotional photograph cannot be the only guide. The whole future pattern of hair loss has to be considered. A family history review before hair transplant helps decide whether grafts belong at the front, crown, or in reserve.
The crown can wait in many patients. A wasted donor area cannot be easily replaced. That is the principle to understand before accepting an aggressive front to crown package.
If the donor is excellent, the hair is thick, the crown is small, and the frontal area is already stable or already treated, the discussion changes. But when donor supply is limited, the front usually deserves first priority.
Priority compass
Four checks before choosing hairline or crown first
The best first zone is not always the area that bothers the patient most. A useful plan compares face framing, crown demand, donor reserve, and whether staging protects future options.
Face frame
Which zone changes the face most?
A weak front can affect the face more than a crown gap that is mostly seen from above.
Even splitting can leave both zones weak. Priority planning asks which zone gives the clearest value with the donor supply available.
Use this as a planning frame, not a diagnosis or approval for surgery. The final plan still depends on donor reserve, recipient area anatomy, hair type, medical history, and future hair loss risk.
Even graft division is rarely the right plan
Often, no. Even distribution sounds fair, but surgery is not accounting. The hairline, middle scalp, crown, and donor area do not all give the same visual return for each graft.
If 3,000 grafts are automatically divided into equal parts, the plan needs a closer look. The front may receive too little density to frame the face properly, while the crown may still look thin because the area is curved, exposed to light, and larger than it appears.
This is not really a question of dividing grafts evenly. The decision depends on where each graft gives the most natural improvement while still preserving donor reserve.
Sometimes this means a strong frontal plan and no crown work in the first surgery. Sometimes it means a strong front with gentle crown softening. Sometimes it means treating the crown later, after the first result and the future hair loss pattern are easier to judge.
A balanced plan is not the same as an equal split. A balanced plan protects the most visible areas, respects the donor, and avoids spreading grafts so widely that every area looks unfinished.
Crown treatment in the first session
The crown can sometimes be treated in the first session when the crown loss is limited, donor supply is strong, the hair characteristics are favorable, and the frontal goal is not too demanding. Then, a balanced plan may include some crown work without sacrificing the front.

Crown treatment in the first session makes the most sense when the patient has realistic expectations. The patient needs to understand that crown density usually looks softer than the frontal hairline. They also need to understand that the crown whorl changes hair direction and makes the area visually demanding.
A small crown with good surrounding hair is a different problem from a broad crown in advanced hair loss. A small crown may improve nicely with moderate graft use. A broad crown can absorb many grafts and still look thin under bright light.
The answer changes from patient to patient. Hair caliber, curl, scalp color, contrast, donor density, crown diameter, existing miniaturized hair, and future loss risk all change the decision.
The exact graft number is therefore a result of analysis, not a decoration on a proposal. If the surgeon cannot explain why the number fits the surface area, donor reserve, and density goal, the number is not ready to be trusted. Patients comparing different estimates need to understand how a surgeon calculates graft number.
In a combined session, the priority needs to be clear. Sometimes the goal is a stronger hairline with only light crown softening. Sometimes the crown waits. The weak plan is one where grafts are spread so widely that every area looks slightly treated but none looks strong.
A combined plan is not wrong by definition. A careless combined plan is the problem. If the grafts are diluted across too much surface area, the patient may finish with neither a strong front nor a satisfying crown.
Modest crown density often protects the donor better than spending grafts aggressively and leaving the donor area weaker than the result deserves.
The crown can feel like the main concern
If the crown bothers you more than the hairline, I still need to ask why. Sometimes the crown is truly the main cosmetic problem. Sometimes it only feels that way because photos from above make the area look worse than it appears in normal life.
The crown is often unfairly judged. Bathroom lighting, wet hair, a short haircut, high scalp contrast, and the natural whorl can make it look empty even when there is still meaningful hair. I try not to operate on an illusion created by light and angle.
If the front is strong and the crown is the only weak area, then crown treatment can make sense. But if the front is unstable, the hairline is receding, and donor supply is limited, the plan needs to become more conservative. The front may not bother you today, but it may become the larger problem later.
A crown heavy plan can also age badly if future thinning opens the middle scalp or frontal area around it. The crown may grow, but the overall pattern can still look unbalanced because the grafts were spent in the wrong order.
Age matters here. A younger patient with crown thinning may still have a pattern that is not fully declared. If the crown is transplanted too aggressively before the future front is understood, the patient may lose strategic flexibility.
I check whether medical treatment could improve the crown. The crown can sometimes respond better to medication than a fully bald frontal hairline. I do not read that as medicine replacing surgery in every case, but it can change timing and graft need.
If your crown bothers you most, I do not dismiss it. I simply do not let that emotion overrule the larger plan. A strong surgical plan solves the right problem in the right order.
Your preference matters, but it has to be guided by donor reality, not sold back to you as if every wish can be delivered safely.
Donor strength changes the decision
Donor supply is the limiting factor. Every graft spent in the crown is a graft that cannot be spent in the front, the middle scalp, a repair, or a future session. Donor strength changes everything.
Someone with thick hair, good donor density, low scalp contrast, and a stable pattern has more flexibility. Someone with fine hair, broad loss, high contrast, and donor miniaturization has less. These two situations should not receive the same plan.
Treat donor hair as a limited reserve, not as a number that makes a proposal look generous. Once grafts are removed, they do not return to that donor zone. If the extraction is careless, the donor can become visibly thin, patchy, or depleted.
The donor area in hair transplant has to be understood before accepting a plan that tries to cover everything. The donor is not a warehouse. It is living tissue with a cosmetic future of its own.
When the donor is limited, I often protect the result by building a strong frontal frame and keeping the crown modest. This may sound less exciting, but it protects the patient from a diluted result and a damaged donor.
When the donor is strong, we may have more room to discuss crown improvement. Even then, I do not treat the crown as an unlimited target. The crown can always ask for more grafts. The surgeon has to know when to stop.
You may think you are choosing only between front and crown. In reality, you are choosing between quick coverage and future flexibility.
Use the 10 priority slides below to see how donor reserve, face framing, crown size, native hair stability, and staging change the plan. Swipe the carousel, use the arrows for one step at a time, or choose a number below the image to jump to that point.





Crown grafts can disappoint for visual reasons
Crown grafts can disappoint because good growth does not always mean strong visual coverage. The crown is curved, exposed to overhead light, and shaped by a whorl pattern. Hairs change direction, separate easily, and show more scalp than patients expect.
In the front, hair can be layered forward and supported by facial framing. In the crown, the hair radiates in different directions. That means the same number of grafts may create less visible impact in the crown than in the frontal area.
Wet hair makes the crown look even more open. Strong bathroom light can be brutal. Phone photos from above can exaggerate thinning. You may think the transplant failed when the real issue is that the crown has less optical forgiveness.
Graft number alone is not enough. A clinic may say a certain number will fix the crown, but the real result depends on surface area, shaft thickness, color contrast, curl, direction, and existing hair.
This broader visual issue is one reason why some hair transplant results look thin. The same lesson applies strongly to the crown.
When patients expect crown density to look like a full untouched scalp, disappointment becomes likely. When they understand that the goal is improvement, softening, and better coverage under normal conditions, the discussion becomes more realistic.
Crown graft numbers cannot be used to create fantasy. The surgeon has to explain what the crown can do and what it cannot.
Staged planning instead of one large session
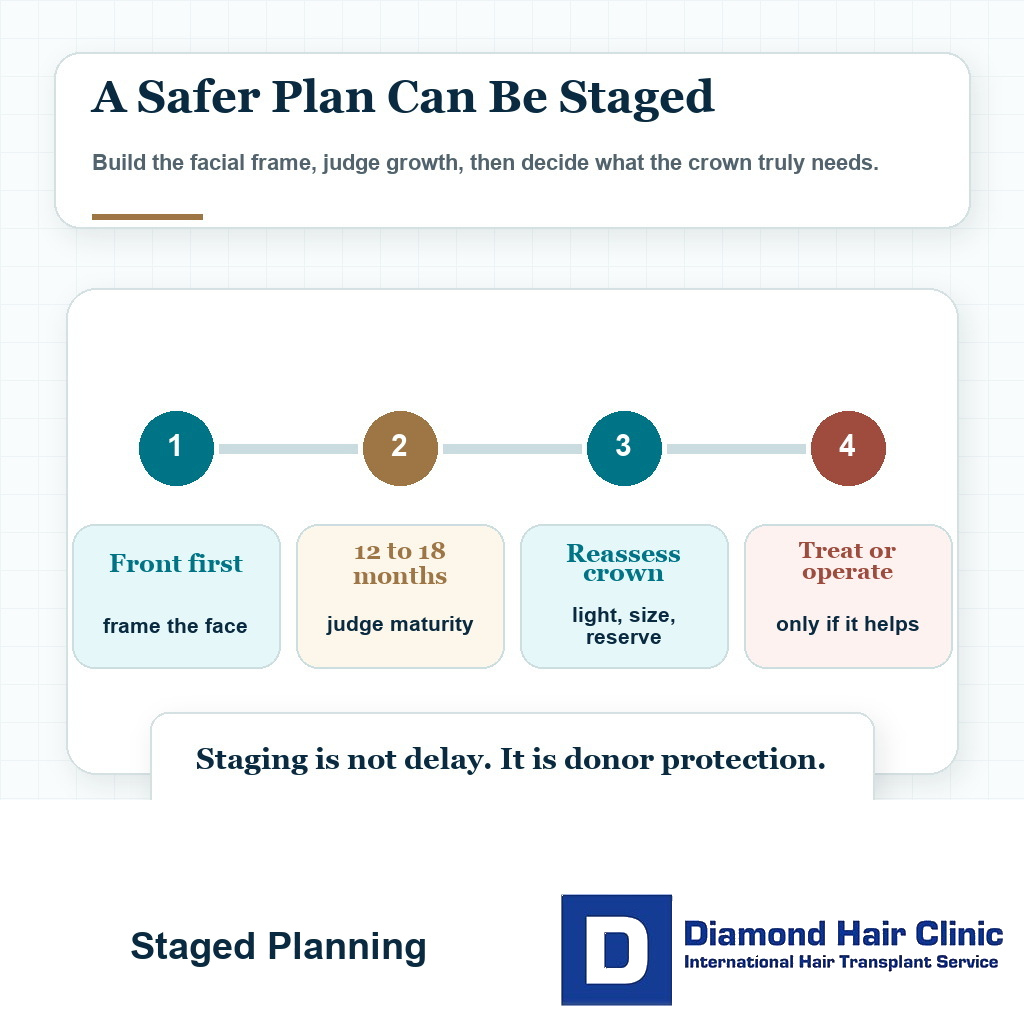
A staged plan is better when the patient has broad loss, uncertain future progression, limited donor supply, or competing priorities between front and crown. It is also better when the first session needs to prove how the hair grows, how the patient heals, and how the design looks in real life.
In advanced patterns, the surface area can be much larger than the patient realizes. A plan that sounds complete may still leave thin coverage if grafts are spread too widely. That is the wider problem in advanced baldness in one hair transplant session.
For some patients, building the frontal frame first and reassessing the crown after the result matures is safer. That usually means waiting 12 to 18 months before making the next major surgical decision. The purpose is not delay for its own sake. The purpose is judging the first result properly.
A second session can be a very good decision when the first operation created a stable foundation and the donor area remains healthy. It can also be a mistake if the first plan used too many grafts too widely and left no clear reserve.
Whether a second hair transplant is worth it depends on whether it is part of a thoughtful plan, not a rescue attempt after poor graft allocation.
The staged approach can be emotionally difficult because most people want everything corrected at once. But surgery is more than what can be done in one day. The real test is what will still look natural and flexible in 5, 10, or 15 years.
A one session plan may sound convenient. But if it spreads the grafts too thinly, weakens the donor, or gives the crown too much priority, the convenience disappears later.
Slower planning is sometimes the more protective choice. It may be frustrating in the consultation, but it can prevent a much more difficult donor problem later.
Medication can change the crown decision
Medication can change the crown decision in specific cases. The crown often contains miniaturized hair that may still respond to medical treatment. If that hair can be stabilized or improved, the surgical plan may become smaller, safer, or better timed.

Medication is not a miracle. It does not rebuild every crown. It does not replace surgery in a bald smooth area. But when there is still weak native hair, it can be a serious part of the plan.
I often consider whether the crown needs a medical trial before donor grafts are committed. If the patient is young, the crown still has hair, and the donor is not unlimited, this discussion becomes central to the plan.
This is the same logic behind discussing medication before hair transplant, because surgery cannot be used to ignore a biological process that is still active.
Medication can also help protect surrounding native hair after a transplant. If the transplanted hair survives but the native hair behind or around it continues to miniaturize, the cosmetic result can weaken over time.
For crown planning, this matters a lot. The crown can expand. A small treated area today can become surrounded by future thinning if the disease process is not controlled.
Crown medication and crown surgery cannot be treated as opposing slogans. Diagnosis comes first, stabilization is considered when useful, and surgery follows when the plan is clear.
A promise to cover everything needs caution
If a clinic promises to cover everything in one session, slow down and look at the cost of that promise. Donor safety, density, naturalness, and future options can all be weakened when the plan tries to solve every area at once.
Large graft numbers can sound reassuring. Someone hears 5,000 or 6,000 grafts and thinks the clinic is being generous. But a high number is not always a good plan. It may simply mean the clinic is willing to spend more donor hair without explaining the consequences.
Clinic marketing can become dangerous here. The patient wants certainty, and the clinic gives them a big number. But the number does not tell them whether the grafts will be distributed well, whether the donor will remain natural, or whether the crown is being given too much priority.
If you receive very different graft estimates from different clinics, you need to understand why hair transplant graft numbers differ before choosing the highest one. The highest number may be correct in some cases, but it must never win by emotion alone.
A plan needs special scrutiny when it tries to lower the hairline, fill the temples, reinforce the middle scalp, and cover a broad crown without a serious donor discussion. That may look impressive on the quote. It may not look impressive years later.
A clinic that respects your future needs to be able to say no. It needs to be able to leave the crown for later. It needs to be able to explain why a smaller plan may be wiser.
Do not treat careful planning as a disappointment. If the plan protects the donor and leaves the crown for later, that may be the reason the result still has options years from now.
How I review the priority after the first result?
The first operation should already contain the review point. If I build the front first and leave crown work for later, I explain which photos, timing, donor healing, frontal density, crown progression, and medication response will matter before a second decision is made.
At 12 to 18 months, the question is not only whether the patient still notices the crown. I also look at how the frontal frame matured, whether native hair stayed stable, whether donor reserve still looks healthy, and whether crown work would now add enough visible value for the grafts it spends.
For that reason, choosing between the front and crown is not a single day preference. It is a plan with a first target, protected reserve, and a future review. A patient who needs that kind of staged thinking should also understand how follow-up after surgery keeps the next decision connected to the original plan.
Choosing the right priority for your scalp
The decision begins with diagnosis, not desire. I need to know your age, hair loss pattern, donor strength, hair caliber, crown size, frontal recession, medication history, family pattern, expectations, and whether the result you want can be created without exhausting the donor.
If the front is weak and the crown is also thinning, the frontal frame usually comes first unless there is a strong reason not to. If the front is already acceptable and the crown is the main remaining concern, crown work may move higher in priority. If both are severe and the donor is limited, compromise is unavoidable.
First understand whether you are a good candidate for hair transplant. A patient can want surgery very badly and still need a more conservative plan than they expected.
The consultation cannot become a list of promises. It needs to clarify which area gives the best visual return, what needs to remain in reserve, whether the crown can wait, whether medication may reduce the crown need, and how future hair loss could affect the plan.
Daily life matters too. If the front affects every conversation and every photograph, that is a different priority than a crown that mainly bothers you in overhead photos. If the crown is the true emotional burden and the front is stable, that also deserves respect.
Do not judge the plan by the largest number, the fastest date, or the most complete sounding promise. Judge it by whether it protects the donor and creates a natural result that can age well.
For many patients, hairline and frontal middle scalp first is the safer priority, with the crown planned later if donor supply and timing allow. The crown can matter deeply. I simply do not let it spend the grafts needed for the face and the future.