


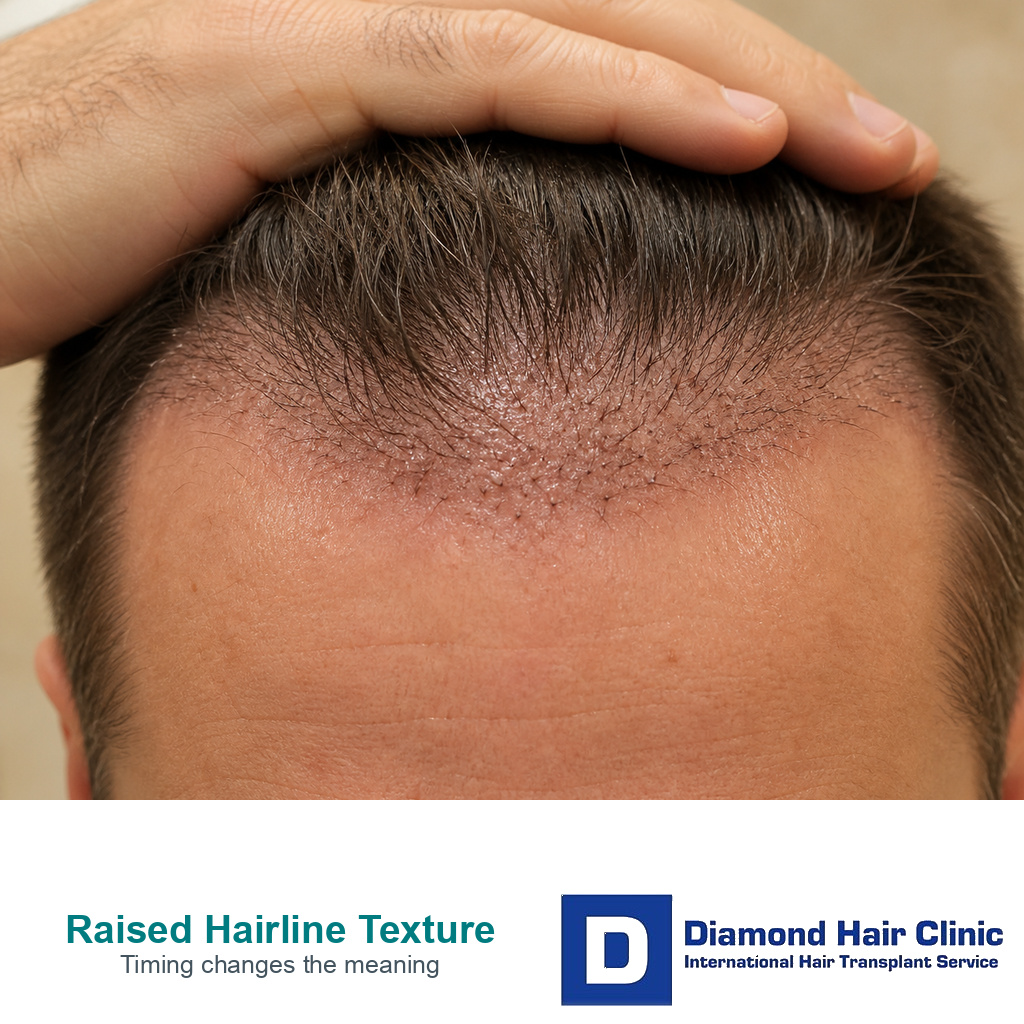
Raised Hairline Texture and When to Ask for Review
A bumpy or raised hairline after FUE can be part of early healing, especially in the first weeks when crusting, swelling, tiny scabs, and shedding make the recipient area look uneven. The concern changes when the surface forms fixed rows, pits, ridges, or cobblestone texture, or when bumps come with heat, worsening pain, discharge, fever, a new dusky skin change that looks damaged, or an open wound.
A case like this should not be judged from one dramatic close view. I look at timing, symptoms, pattern, and whether the skin is settling or becoming more fixed. Until the clinic reviews it, protect the grafts, avoid rubbing or squeezing, and document the area before trying home fixes.
Bumpy recipient area in the first weeks
Some uneven texture is common in the first days and weeks. The recipient area has thousands of tiny channel openings, so it can look raised from swelling, crusting, dried serum, tiny scabs, and the normal inflammatory phase of healing. The transplanted hair can also shed before the skin looks smooth, so the surface suddenly becomes easier to inspect.
You may see small orange colored spots on the first day, small crusts around grafts, or a rough surface when the scabs begin to loosen. I do not treat that as graft failure by itself. If the area is gradually settling, the color is improving, pain is not increasing, and the review photos are reassuring, I usually watch early texture rather than treat it aggressively.
The mistake I try to prevent is comparing the scalp with a smooth forehead too early. The recipient area is healing tissue, not untouched skin. Early swelling and crusting can make the hairline look higher, thicker, row shaped, or uneven before the surface settles.
Timing of bumps after surgery
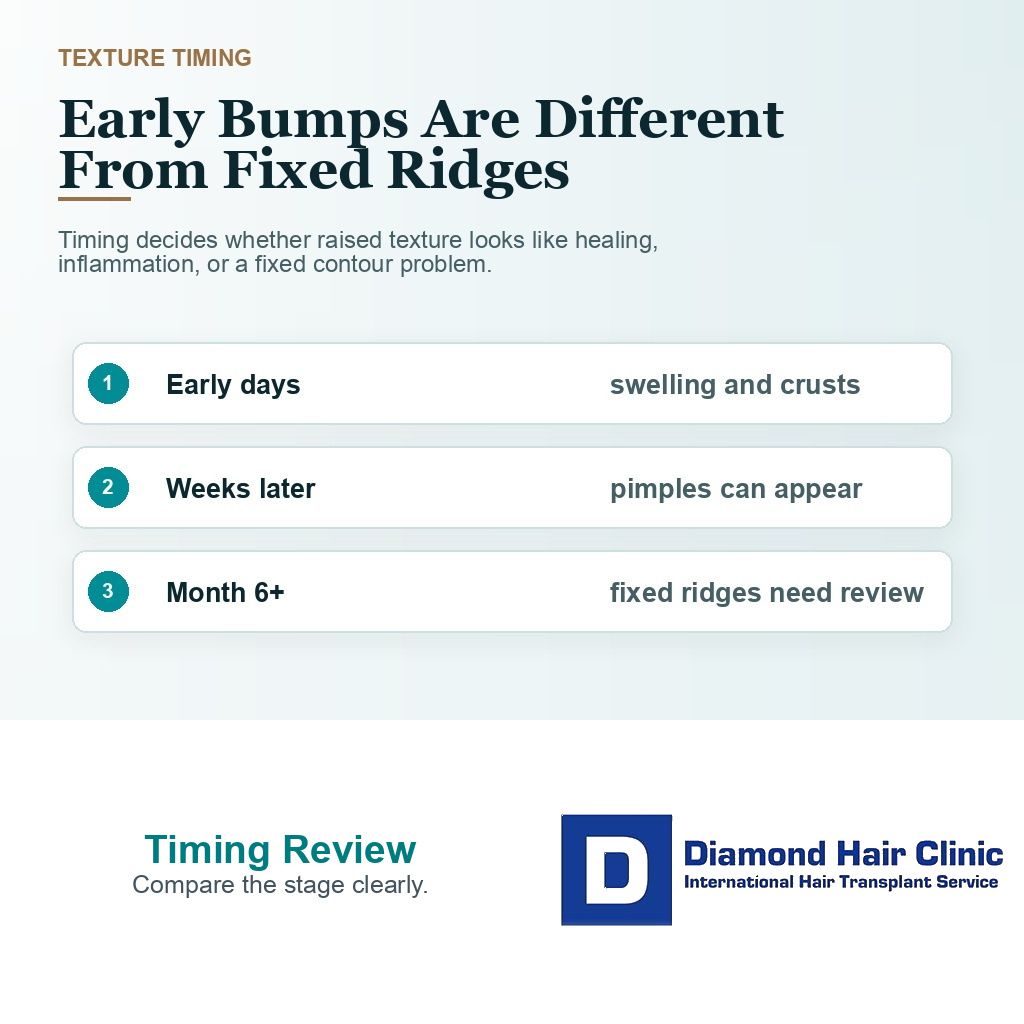
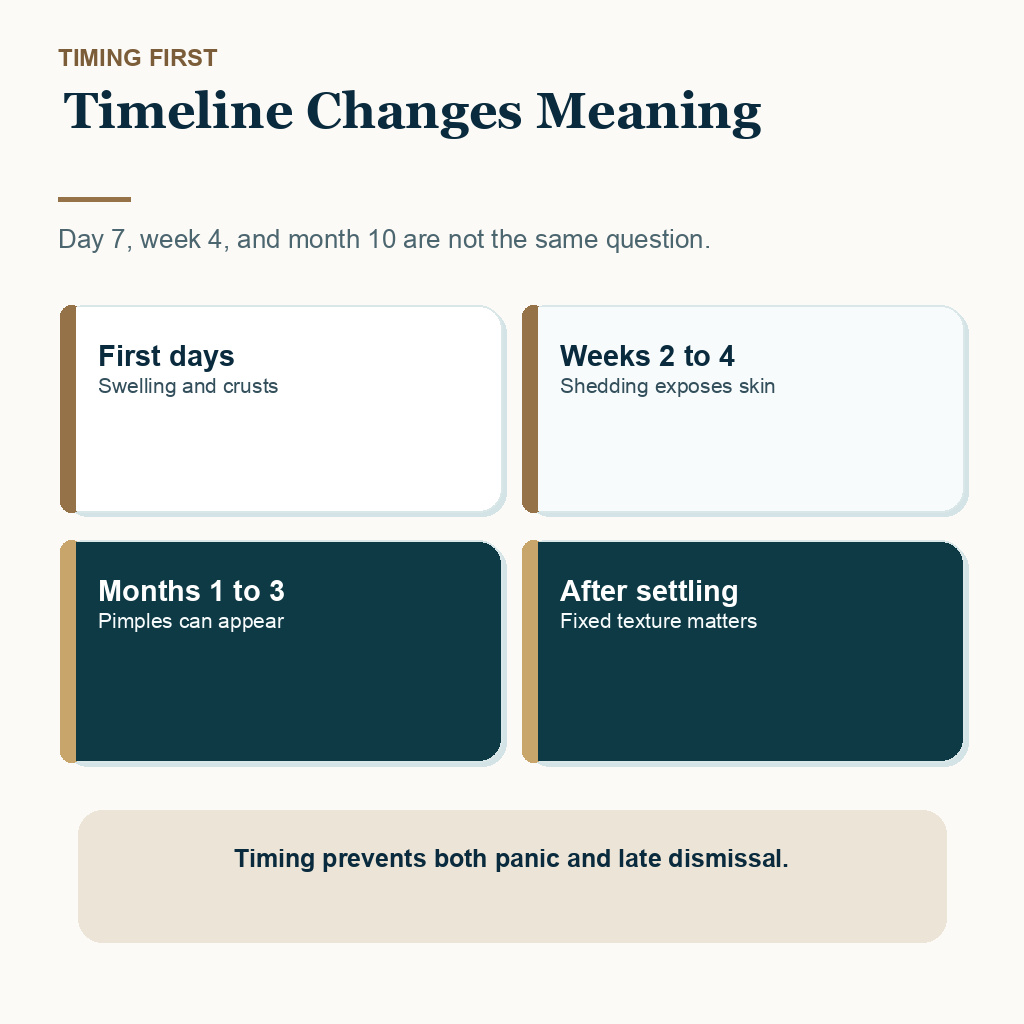
Timing changes the meaning. In the first few days, raised dots often reflect swelling, graft sites, crusting, and dried fluid. Around the second to fourth week, shedding can expose texture that was hidden by implanted hair. Around one to three months, pimples, ingrown hairs, and folliculitis can appear as new hairs begin to move under the skin.
When texture remains firm, row shaped, raised, or indented after inflammation has settled, I review it differently. A fixed ridge at the hairline, small pits around graft exits, or a cobblestone surface months later may point toward scar texture, graft placement depth, old plug work, dense packing, or healing biology. If the visible problem is also unwanted hair position, bad hairline graft removal choices should be considered separately from skin texture treatment.
A bump at day 7 and a fixed ridge at month 10 are not the same problem. Soft swelling that changes from day to day is different from a firm line or pit pattern that remains after redness settles. The first may be part of healing. The second deserves physical review, good photos, and sometimes delayed repair planning after growth and inflammation have matured.
These 10 raised texture slides separate timing, early healing texture, follicle centered bumps, fixed ridges or pits, warning symptoms, photo evidence, and repair timing. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.






Swelling and early healing texture
Bumps are more likely to be healing texture when they are small, diffuse, similar across the treated area, and improving slowly. Mild tenderness, tightness, and uneven crusting can fit the early recovery period when the symptoms are settling rather than escalating.
The healing timeline matters too. If the scabs are coming off, redness is fading, the skin is less tender, and new irritation is not spreading, monitoring may be enough. Good follow up helps you avoid reacting too early while still catching the moment when review becomes necessary.
If your main worry is graft security, I separate that from surface texture. Hair transplant graft security covers when grafts are harder to dislodge. A graft can be secure while the surrounding skin still looks rough, irritated, or swollen.
Pitting, ridging, and cobblestoning concerns
Pitting means small depressed marks or tiny holes in the recipient area. Ridging means a raised line or shelf shaped area, often near the hairline. Cobblestoning means a bumpy, irregular surface where grafts or healing tissue sit unevenly. These words are sometimes used loosely online, so diagnosis from photos alone can be unreliable.
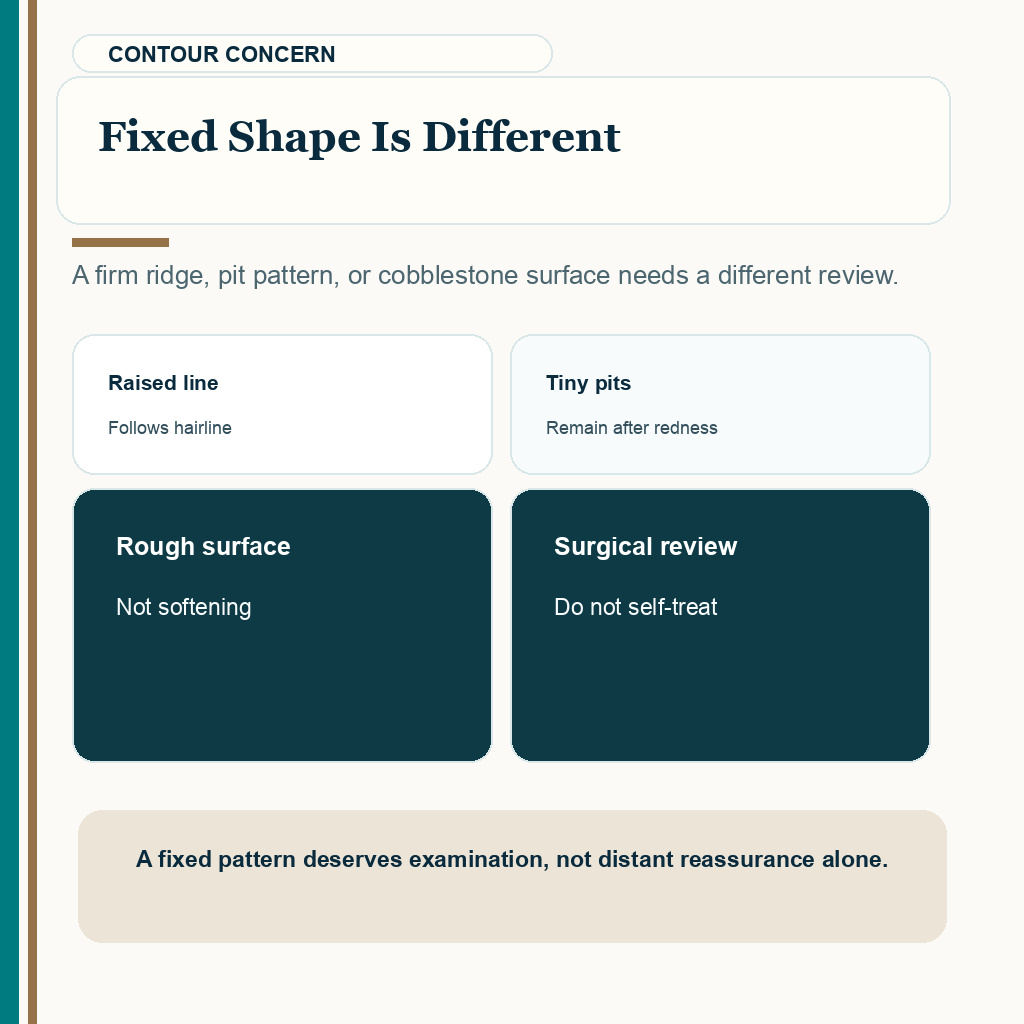
My concern rises when the texture looks organized rather than random. Parallel raised rows, a firm ridge following the hairline, pits that remain after redness has settled, or a rough surface that does not soften with time should not be brushed aside as ordinary scabbing. I need to know when it appeared, whether it is changing, and whether it matches where grafts were placed.
These problems can come from several mechanisms. Grafts sitting too high, channels created at the wrong depth, too much tissue compression, piggybacked grafts, older plug work, aggressive density, or scar response in the skin can all change surface contour. The same scalp can have normal healing in one area, folliculitis in another, and a more fixed contour problem at the hairline.
When I see persistent raised or indented texture, I treat it as a surgical quality concern, not just a cosmetic worry. It needs review by someone who can examine the skin, not a verdict based only on cropped images. Texture that feels soft and changes with swelling is not the same as a firm scar shelf, and that difference is difficult to prove from one photo alone.
Folliculitis and ingrown hairs can make the surface bumpy
Folliculitis, ingrown hairs, small cysts, and pimples can make the recipient area feel bumpy during recovery. These bumps usually have a focal point around a follicle. They may look red or white, feel tender or itchy, and come and go. That is different from fixed pitting or ridging, although both can look alarming in photographs.
When the spots look more like inflammation, I first judge the redness, scabs, and pimples after hair transplant pattern. If infection is part of the picture, I treat folliculitis and hair transplant surgery as an infection control question, not as cosmetic guessing.
Do not squeeze these bumps in the recipient area. Squeezing can irritate the skin, introduce bacteria, and create more inflammation. Do not add leftover antibiotics, steroid creams, acne products, or strong antiseptics without instruction, because they can change the surface and make diagnosis harder. What I need first is clear photography, a note about pain, heat, discharge, itching, and timing, and clinic instruction on washing or medication before you try to fix the bump at home.
Warning signs for faster clinic review
Some texture changes are not only about appearance. I want prompt clinic review if raised areas come with spreading redness, increasing heat, worsening pain, yellow or green discharge, bleeding that restarts, fever, a foul smell, a new dusky, black, gray, wet, or damaged skin area, an open wound, or swelling that is getting worse instead of settling.
By dark change, I mean a new change in the operated skin that looks damaged, not naturally darker skin tone or ordinary redness after surgery. Infection and recipient area necrosis are uncommon, but they are not problems to manage by waiting for casual reassurance from a distance. If you feel unwell, dizzy, feverish, or very weak, think beyond the grafts and protect general medical safety. If the clinic cannot review urgent symptoms quickly, local medical assessment comes before waiting for the next message reply.
Worsening pain, heat, drainage, fever, or skin that looks damaged moves the issue from texture anxiety to medical review. In that setting, waiting for the surface to “smooth out” can be the wrong response.

Avoid rubbing, massage, and squeezing
Do not try to force a bumpy hairline flat by rubbing, scraping, squeezing, needling, or aggressive massage. Early grafts and healing skin need careful handling. Later scar texture also does not become safer because you apply more pressure.
Sometimes gentle scalp management or clinic directed massage is reasonable later, but I decide that from the healing stage and the surgeon’s instructions. During scalp massage after hair transplant, pressure and timing matter. Early rubbing can irritate the recipient area, disturb scabs, and make a review harder because the skin becomes more inflamed.
If the surface is truly scarred, home force is not a repair plan. It may create more trauma. I separate swelling, folliculitis, pitting, ridging, cobblestoning, and hair angle problems only after the skin has had enough time to mature, unless infection or damaged skin needs faster medical attention.
Dense packing and high graft numbers can affect skin texture
The recipient area has a blood supply and a healing capacity. I am not against dense packing when the skin, graft size, channel angle, and surgical handling allow it. The risk starts when a clinic treats the scalp like empty space to fill with as many grafts as possible.
High density means more incisions in a small area. If channels are too close, too deep, too shallow, or poorly angled, the skin can heal with visible irregularity. Large sessions also create more swelling, more tissue handling, and more opportunity for uneven healing when the plan is not conservative enough.
When I plan grafts, I cannot separate number from surface quality. Chasing too many grafts in one area can create surface risk when the tissue cannot accept the density. Copying 45 grafts per cm2 or avoiding transparent graft count verification can also hide that risk from you. More grafts only help when the tissue can accept them and the donor plan remains responsible.
A natural hairline is not only about hair direction. The skin surface also has to heal naturally. A dense result that leaves visible ridging or pitting can still trouble you, especially under harsh light, with short hair, or after shedding exposes the surface.
Sending photos for clinic review
Use photos that help us judge change over time. Use soft daylight or consistent indoor light. Include one close view, one middle distance photo, and one photo from the side. If the texture is raised, a side angle can show contour better than a straight overhead photo. A short video with light from the side can also help when the question is surface height rather than color.
A dramatic zoomed image with flash is not enough. Flash can exaggerate pores, scabs, shadows, and tiny height differences. Also send the surgery date, the day or month after surgery, whether the bumps are painful or itchy, whether there is discharge, whether the area feels hot, what products were used, and whether the texture is improving, stable, or worsening.
If you are far away or the review is remote, hair transplant follow up access needs clear communication and escalation when symptoms cannot wait.

Options if texture remains after full healing
Repair depends on what the texture actually is. Small inflammatory bumps may need medical treatment. Ingrown hairs or cysts may need controlled release or treatment by a clinician. Fixed pitting, ridging, cobblestoning, old plug work, or poor hair direction may need a repair plan, but that plan is usually delayed until the tissue has matured. First, I separate active inflammation from scar response, graft placement, hair direction, or a mixture of more than one issue.
Some repair options may include removing or redistributing problematic grafts, careful additional grafting, laser or resurfacing options in selected cases, scar revision, or camouflage with a different styling plan. Each option has limits. The donor area may already be reduced, the skin may scar again, and a second procedure can make the situation worse if the diagnosis is wrong. If you have a history of thick raised scars or keloids, revision needs extra caution because new injury can trigger new scar behavior.
A repair plan may involve pluggy hairline repair, wrong hair direction after hair transplant, or bad hair transplant repair, but I do not treat those as the same diagnosis. Texture, graft angle, plug size, donor reserve, and hairline position all need separate judgment.
Judging texture without reacting too early
I start with the timeline. A rough surface in the first weeks often deserves observation and clinic follow up. A painful, hot, draining, damaged, or worsening surface deserves faster review. A fixed ridge, pit pattern, or cobblestone texture months later deserves a proper surgical assessment rather than reassurance from distance alone.
Do not touch, squeeze, scrape, or try to treat a new bumpy recipient area yourself. Share clear photos, describe the symptoms, and let the clinic separate healing, inflammation, folliculitis, and a contour problem that may need later review.
The best protection is planning before surgery. A conservative hairline, careful channel depth, controlled density, direct surgeon involvement, and clear follow up do more to prevent texture problems than any repair promise made after the skin has already healed poorly.