Norwood 3 Hairline and Donor Planning
If you are around Norwood 3, a hair transplant can be reasonable, but the Norwood label is not enough to approve surgery. I first need to know whether the recession is stable enough, where the hairline can safely sit, how much of the front actually needs grafts, and how much donor reserve must remain if the mid scalp or crown changes later. If the pattern has moved beyond corner planning, Norwood 4 or 5 hair transplant planning explains how the graft budget changes.
I treat Norwood 3 as a future planning problem, not only a corner problem. If the corners are rebuilt too low or too densely, the result can look attractive at first and become difficult to manage when native hair behind it can continue to thin.
Norwood 3 is only a starting point for planning
Norwood 3 usually means visible recession at the temples or frontal corners. The central forelock may still look strong, the crown may still look quiet, and you may still style the hair well from the front. The decision can feel confusing because you may not look bald, but the corner loss may be real enough for a surgical discussion.
Norwood 3 is not one identical shape. Some men mainly have corner recession. Some have a more frontal type A pattern. Some have early crown involvement, often described as Norwood 3 vertex. That difference changes whether the plan focuses on the corners, the frontal band, crown risk, or a broader future loss strategy. The label describes the pattern. It does not decide by itself that surgery should happen now.
The Norwood stage gives me a starting point, not a full surgical plan. I still need to examine hair caliber, miniaturization behind the hairline, family pattern, age, medication history, donor density, and the way you want to wear your hair. The same Norwood number can need different treatment in someone aged 23 with fast loss and someone aged 38 with a stable pattern.
Serial photos matter here. A single dry, styled photo may hide thinning behind the forelock, while wet hair, harsh light, or a comb through video can reveal miniaturization that changes the design. If the hair behind the planned front line is weakening, the corner design needs more caution than it would in a stable isolated recession.
This is also why I separate a Norwood 3 plan from a Norwood 2 hair transplant decision. Norwood 2 can sometimes be watched longer because the recession may still be a mature hairline. Norwood 3 usually needs a more serious discussion about whether surgery is being used to restore a natural frame or to chase an old teenage hairline.
Graft quotes vary for Norwood 3
It is common to receive different graft estimates from different clinics for Norwood 3. One clinic may quote around 1,800 to 2,200 grafts. Another may quote 3,000 or more. The difference is not always proof that one estimate is wrong, but it is a signal that you need to understand what each clinic is trying to build.
Fine hair, light hair against light skin, a wide forehead, deep corners, or a plan that blends into the forelock may increase the graft number. A lower hairline or stronger temple corner closure also increases the number. A more conservative design may use fewer grafts because it respects the existing central forelock and avoids creating a dense wall at the front.
The number is unsafe when it is separated from the design. A graft count without a hairline drawing, donor assessment, density target, single hair front row plan, and future loss plan is only a sales number. Ask whether the quote covers only the corners or also the frontal band behind them. A slightly slower plan can protect you better than spending too much donor hair in the first procedure.
Norwood 3 planning starts with stability, hairline height, donor reserve, and the treatment plan you can realistically maintain.
Norwood 3 can still be too early for surgery
Norwood 3 can be too early for surgery when the pattern is still moving quickly, you are very young, the family history points toward advanced loss, or the treatment plan has not been tested long enough. In that setting, surgery can create a strong front while the native hair behind it continues to retreat.
Age matters because donor hair is limited and male pattern hair loss often progresses over years. A man aged 22 with Norwood 3 recession may feel desperate because the corners affect the face, dating confidence, and photographs. I understand that pressure. Still, the design has to survive the possibility of Norwood 5 or 6 progression, not only look good at today’s hair length and styling angle.
In a younger patient, too young for hair transplant is not decided by birthday alone. Pattern stability, donor area, medical treatment, and emotional expectations decide whether surgery is mature enough.
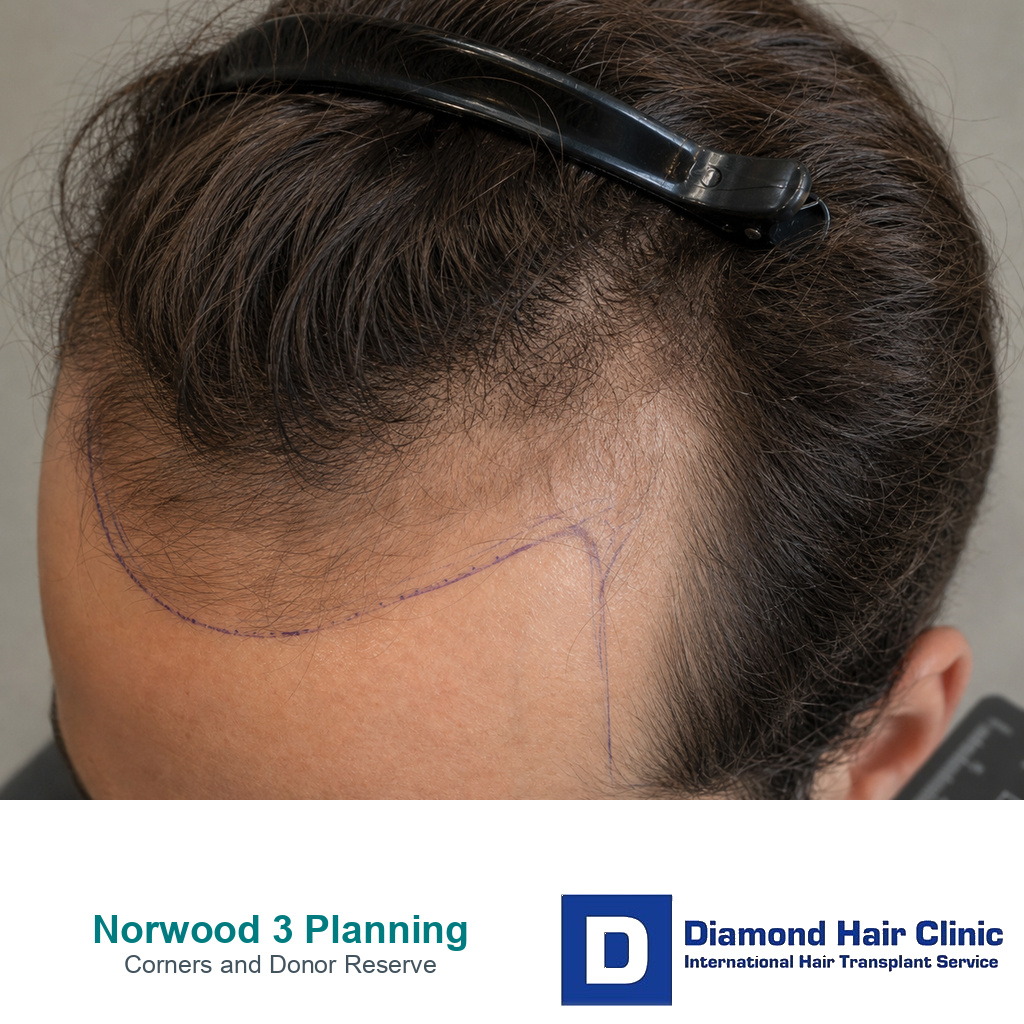
Restoring corners without an artificial look
The corners need to be restored to a mature frame, not to the lowest line you can imagine. A Norwood 3 hairline often needs softness at the front edge, slight irregularity, correct direction, and enough recession left to suit the face as it ages. A perfectly straight, low, dense hairline can look impressive in one photo and artificial in real life.
Temple corner work is especially unforgiving. The hair direction changes, the skin angle changes, and the first rows need finer single hair grafts. If the corners are closed too aggressively, the face can look boxed in. If the corners are ignored completely, you may feel the transplant did not solve the visible problem. The balance is surgical, not cosmetic drawing.
I also separate frontal corner recession from temple point reconstruction. Closing the frontal corners can frame the face. Rebuilding weak temple points is a different decision with different angles, finer hairs, and higher risk of looking unnatural if the donor hair is not suitable. A Norwood 3 plan needs to say which one is being treated.
Hairline design in hair transplant surgery and temple graft count planning both sit inside this decision. The front that ages best is not the lowest front. It is the line that fits your current face, your donor capacity, and the likely future pattern.

Norwood 3 corner design needs to improve the frame without spending future donor reserve too aggressively.
Front corners do not show the whole risk
At Norwood 3, it is easy to look in the mirror and see only the temples. I look at the whole scalp. I check the forelock, mid scalp, crown, donor area, beard option if it may matter later, hair shaft thickness, and signs of diffuse miniaturization. The front corners may be the visible complaint, but they are not always the only area at risk.
If the crown is likely to open later, a very aggressive frontal plan can steal grafts from a future crown or mid scalp strategy. If the forelock is miniaturizing, the transplant must blend into hair that may become weaker. If the donor area is already fine or limited, a dense corner repair can create donor thinning that only becomes obvious after the first short haircut.
The same donor budget issue can return later if the hairline is repaired first and the top then needs a second transplant review for thin coverage.
In a Norwood 3 case, lifetime graft planning matters from the first design. Donor hair is not an unlimited budget. Once grafts are moved, the decision cannot be undone without another repair problem.
Medication tolerance and family history can change the plan
Medication does not replace surgery when the corners are already empty, but it can change the timing and the design. If finasteride, dutasteride, or minoxidil helps stabilize native hair, the transplant can often focus more confidently on the missing corners. If you cannot tolerate medication or do not want it, the surgical plan must assume more future native thinning.
I do not design a Norwood 3 hairline as if treatment will freeze hair loss forever. I ask what you have actually used, what side effects occurred, whether the response has been stable, and whether the plan still works if medication is reduced or stopped. Active shedding or weak response changes the surgical threshold, which is why still losing hair on medication before a transplant deserves a separate look.
Family history also matters. If your father, uncles, or brothers moved from early temple recession to Norwood 5, 6, or 7, I treat your front corners with more caution. A careful review of family hair loss history matters here because a nice Norwood 3 result should not trap you into an unnatural island if your pattern later becomes stronger.
Realistic graft range for Norwood 3
There is no universal graft number for Norwood 3. A small corner softening may sit around 1,500 grafts in the right case. A broader frontal reconstruction that blends into the forelock may move closer to 3,000 grafts. Many plans sit between those examples. Fine hair often needs more grafts for the same visual coverage than coarse hair, and a lower design needs more grafts than a mature design.
I treat those numbers as examples, not promises. The real estimate depends on measured surface area, hair caliber, desired density, existing native hair, and donor safety. I avoid promising a fixed number before seeing the scalp in detail because false precision can lead to poor planning.
A serious estimate needs to connect the drawn area to the density target. The front edge may need finer single hair grafts, while the area behind it may need different follicular units and a different density. Existing native hair can reduce the empty surface area, but it can also make placement more delicate if those hairs are miniaturizing.
The proposed number has to match the surgical goal. If a clinic quotes a high number, ask where those grafts will go, how many will be reserved for the first rows, how density changes behind the first rows, and how donor reserve will be protected. If a clinic quotes a low number, ask whether the result will look unfinished. A mature Norwood 3 plan explains both the visible frame and the donor cost you cannot see in the mirror.

Different graft quotes can all sound plausible until the design, hair caliber, donor reserve, and staged plan are reviewed together.