Ongoing Hair Loss on Medication Changes Timing
If you are still losing hair while using finasteride, dutasteride, minoxidil, or another treatment, a hair transplant may still be possible. I do not plan it like a routine stable case. First I separate active progression from a temporary medication shed. I also need to know whether side effects, tolerance limits, uncertain diagnosis, or donor reserve change the plan. If the limiting issue is side effects rather than weak response, review finasteride side effects and transplant planning before graft numbers are fixed.
If the treatment list includes natural DHT supplements, I include saw palmetto around FUE planning in the stability review, but I do not treat it as proof that the pattern is controlled.
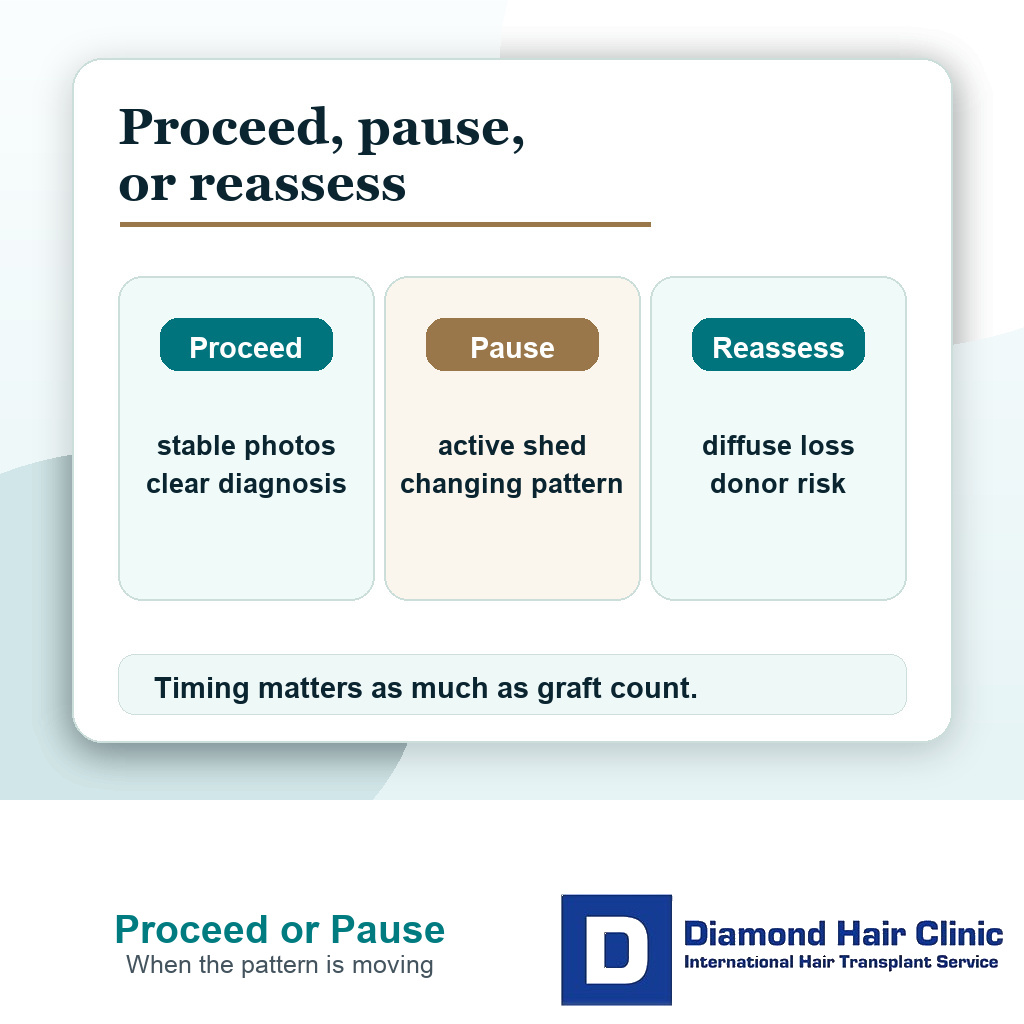
Do not use surgery to chase an unstable pattern. If the donor area is strong, the goal is conservative, and the diagnosis is clear, surgery may still be reasonable. If the pattern is changing quickly, the crown is opening, or the donor area is limited, waiting or adjusting treatment with the prescribing doctor may protect you from a result that looks good briefly and then becomes difficult to maintain.
Stable enough means a pattern I can plan around
Stable enough does not mean zero hairs in the shower. Everyone sheds hair. It also does not mean that medication has restored everything. For surgery, I am looking for a pattern that I can plan around with reasonable confidence.
That means the hairline, mid scalp, crown, and donor area have been compared over time, not judged from one mirror photo. I check whether the loss is still moving quickly, whether miniaturized hair sits behind the planned transplant zone, and whether the donor area itself looks safe. A real assessment gives more protection than a quick graft estimate from photos.
If the goal is only a small, age appropriate frontal refinement, a little uncertainty may be acceptable. If the plan needs dense frontal work, crown coverage, and a large graft number, uncertainty becomes much more dangerous. That is where lifetime graft planning starts to matter. In a Norwood 3 hair transplant plan, that uncertainty changes how low the corners should be rebuilt.
Medication response can be hard to judge
Medication response is rarely as clean as you want it to be. Finasteride or dutasteride may slow the loss without making the hair look thicker. Minoxidil can trigger a shed before improvement. You may improve in the crown but keep thinning in the hairline, or feel worse because daily photos are taken under different light. Stabilization can still be useful even when it does not create the thicker look you hoped for.
I separate three questions. Has the medication reduced the speed of loss? Has it created any visible thickening? Has it made the surgical target more predictable? Those are related, but they are not the same question. The same separation helps after surgery when native hair looks thinner after FUE and medication history may change the interpretation. That same distinction is central to spironolactone hair transplant planning in women, where response and predictability matter more than the prescription label alone. The same medication timeline can also explain why transplanted hair looks thinner years later, especially when treatment was started, stopped, or changed.
One bad week or one emotional photo is not enough to read medication response. The purpose of medication before a hair transplant is to make the surgical map clearer, not more confusing. If you started or changed treatment recently, the timing can be hard to read. A minoxidil shed before transplant planning is the clearest example, but any treatment change can make the scalp look worse before it becomes clear. Changing several treatments every few weeks can make this even harder, because you no longer know which change caused the shed or improvement. Medication stability is measured over months, not a bad week. A medication timeline with start dates, dose changes, missed periods, side effects, product switches, and the reason for each change is more useful than saying only that the treatment “did not work.”
If one of those changes is an online spray, compounded topical, or research chemical style product, bring the same detail described in online hair loss topicals before FUE before I decide whether the hair loss is truly unstable. For tablets or capsules, the same logic applies to online hair loss pills before FUE, because the dose, pharmacy, refill dates, and photos matter before I call the medication response weak.
Ongoing shedding can delay surgery
Ongoing shedding becomes risky when it hides the real border between permanent loss, temporary shed, and weak native hair that may disappear later. If I design a dense hairline while the hair behind it is actively thinning, the transplant can look isolated after the native hair changes.
The risk is higher when shedding is paired with visible miniaturization, family history of advanced hair loss, early age, crown involvement, or diffuse thinning across the top. In those cases, surgery may still be possible, but a hair transplant while hair loss is still active has to be conservative enough to survive future change.
A transplant moves hair. It does not stop the disease process. That distinction is central. The transplanted grafts may grow well, while native hair around them keeps thinning. If your native hair is still active, you need to understand continued hair loss after hair transplant before graft numbers are fixed.

Before surgery, I separate treatment response from surgical planning. A temporary shed, active progression, and weak donor reserve are different problems.
Surgery can still be reasonable in a moving pattern
Surgery can still be reasonable when the diagnosis is clear, the donor area is strong, the requested zone is limited, and the plan leaves enough donor reserve for future hair loss. I am more comfortable when you understand that the first operation should not use every possible graft just because the current photos are upsetting.
A man of 38 with slow frontal recession, strong donor density, realistic goals, and stable medical history is a different case from someone who is 22 with diffuse thinning, crown loss, and rapid change despite aggressive treatment. Both may feel equally distressed, but the surgical risk is not equal.
If medication cannot be used because of side effects or medical advice, the question changes. A person considering a hair transplant without finasteride needs a plan built around that limit. Here the focus is different because you are using or have tried treatment, but your pattern still has not become easy to trust.
Donor reserve matters more when the pattern is moving
When the pattern is moving, donor reserve becomes the safety margin. If too many grafts are used early, later thinning can expose the limits of the first plan. A low, dense, youthful hairline may look attractive in early photos, but it can become a burden if the mid scalp and crown continue to open.
I treat donor hair as a limited budget, not an unlimited cosmetic supply. This is especially true when medication has not clearly stabilized the pattern. You may need a second or third plan later, and that future plan is only possible if the first operation did not spend the donor area too aggressively.
Do not judge the plan only by how many grafts can be extracted today. I also need to know how many grafts should remain unused so the result can still look natural in five, ten, or twenty years.
Transplanted hair and native hair carry different risks
You may wonder whether the grafts will survive if medication is not working perfectly. In most androgenetic hair loss cases, transplanted hairs are taken from the safer donor zone because they are more resistant to the same thinning process. But if the donor area itself shows diffuse or retrograde miniaturization, that assumption becomes weaker. Medication does not turn a weak donor area into a safe one.
The native hair around the grafts is a separate question. It may be thinner, more dependent on medication, and more likely to miniaturize after the transplant than the donor grafts themselves. The plan needs a transition zone, not a hard border of transplanted density, so a future gap is less likely if native hair continues to weaken.
The surgical drawing must account for what may disappear later. If there is weak native hair behind the new hairline, I avoid creating a sharp island of transplanted density with an empty gap behind it. If the crown is still changing, I may leave it for later rather than spending too much donor hair on an area that can enlarge.
Native shock loss can also confuse the picture after surgery. If weak nearby hairs shed after surgery, I separate that from medication failure because native hair shock loss after hair transplant can involve hairs that were already miniaturized and may not fully recover.

A hair transplant plan should separate transplanted graft survival from native hair that may keep thinning over time.
Details that matter before choosing graft numbers
Before agreeing to a graft number, I review the diagnosis, donor density, hair caliber, contrast between hair and scalp, age, family pattern, medication history, and the exact zones being treated. Medication history should include what you used, how consistently you used it, why you stopped or changed it, and whether side effects or medical advice limited the plan. Baseline photos from before the medication and comparable photos after a stable period are also useful, because a graft number without that context is not a medical plan.
When you are still losing hair on medication, I am cautious with very large first sessions. The larger the first operation, the more certain I need to be about donor safety and the future pattern. If the clinic gives a high number quickly but does not explain the future loss plan, the decision should slow down.
A second opinion before hair transplant surgery can be useful at this point. Different graft estimates are common, but the explanation behind the number matters more than the number itself.
Age and family history change the decision
Age does not decide everything, but it changes the margin for error. A younger person has more years for native hair to keep thinning. If strong family history suggests advanced loss, a hairline that looks safe today may become too aggressive later.
With younger patients, I need stronger proof of diagnosis, medical stability, and donor reserve before using many grafts. A mature patient with slow change and a stable donor area may have a more predictable surgical window.
Age is part of the medication decision. If you may be too young for a hair transplant, I use a different threshold than I would for planning a hair transplant in your 30s with slower change, even when the same treatment is being used.
Diagnosis may need checking again
If medication is not stabilizing the pattern, I do not assume the diagnosis is straightforward male pattern hair loss. Diffuse thinning, rapid shedding, scalp inflammation, nutritional deficiency, thyroid disease, scarring alopecia, or another medical problem can change the answer.
A transplant into the wrong diagnosis can waste donor hair and delay proper treatment. If the donor area looks weak, the scalp is inflamed, the loss is patchy, or the pattern does not behave like typical androgenetic hair loss, a scalp biopsy before a hair transplant may be part of stronger review. Diagnosis comes first, not a faster graft number.
When the diagnosis is uncertain, surgery should wait. Waiting is not failure. It can be the decision that protects the donor area.
A moving hair loss pattern does not always cancel surgery, but it changes the level of proof needed before grafts are used.
Medication needs enough time before surgery
There is no single number that fits every patient, but a few weeks is rarely enough to judge. Finasteride needs several months before its benefit can be assessed, and minoxidil may take months as well. Early shedding can make the first period look worse. For surgery, the question is not only whether the drug has had time to show benefit, but whether the loss pattern has become interpretable enough to design around. Dutasteride and combined regimens also need proper medical supervision and enough time to interpret. Do not stop, double, or add medication just to force clarity before a surgery date. That decision belongs with the prescribing doctor. Medication timing should not be manipulated only to keep a surgery date.
If the planned surgery is small and the diagnosis is clear, the waiting period may be different from someone who wants dense hairline, mid scalp, and crown coverage. The more grafts a plan requires, the more stable information I need before surgery.
In some patients, I use medication to delay hair transplant surgery rather than rushing to operate. Medication does not need to produce a perfect result to be valuable. Sometimes its value is that it tells us whether the future loss pattern is slowing enough to plan responsibly.
Surgery without reliable medication use
If you cannot stay on medication, I do not treat that decision as a failure. Side effects, fertility plans, medical history, anxiety about treatment, and personal tolerance all matter. Tell the surgeon whether the issue is a side effect, a prescribing concern, a pregnancy or fertility plan, poor adherence, cost, or personal choice, because each reason changes the plan differently. Also say when you stopped or reduced treatment and what happened afterward, so the plan does not confuse shedding after withdrawal with the natural speed of hair loss. But the surgical plan must become more conservative, not more aggressive.
Without reliable long term medical stabilization, I need to protect the donor area even more. That may mean a higher hairline, less crown ambition, staged planning, or choosing no surgery for now if the risk is too high. It may also mean accepting that future thinning could require another plan later.
A conservative operation can still be valuable when you understand the limits. Refusing medication by itself is not the issue. The risky part is asking surgery to ignore the long term consequences of that choice while still expecting a dense, low, full coverage transplant.
Waiting versus moving ahead with surgery
Do not decide from one clinic quote, one set of wet hair photos, or one bad week of shedding. I compare photos over time, examine the donor area, review the medication history, check the diagnosis, and decide whether the requested design can age well if native hair keeps changing. The comparison should use similar hair length, lighting, wet or dry condition, styling, and medication status, because inconsistent photos can make stable hair look unstable.
You are a better candidate when the diagnosis is clear, the donor area is strong, the goal is limited, the hairline is age appropriate, and the plan leaves grafts in reserve. You are a weaker candidate when the loss is rapid, diffuse, unexplained, emotionally urgent, or dependent on a high graft number to look acceptable. Those are the same signs I look for when judging good hair transplant candidates.
My surgical threshold is practical, even when the analysis is detailed. If I cannot explain how the result will still make sense when more native hair is lost, I should not pretend the operation is ready. A transplant should give you a plan, not just a temporary answer to panic.
Ongoing loss on medication needs a timing review, so these 3 slides connect shedding with native hair and whether surgery should wait. Swipe sideways, use the arrows, or choose a number below the image.