Minoxidil Shed and Hair Transplant Timing
If the shed is active and surgery can safely wait, I avoid rushing surgery during an active minoxidil shed.
Shedding around the middle months after surgery needs the same careful timing logic, so I connect the medication timeline with the month 6 to 8 shedding pattern instead of judging the transplant from one shower.
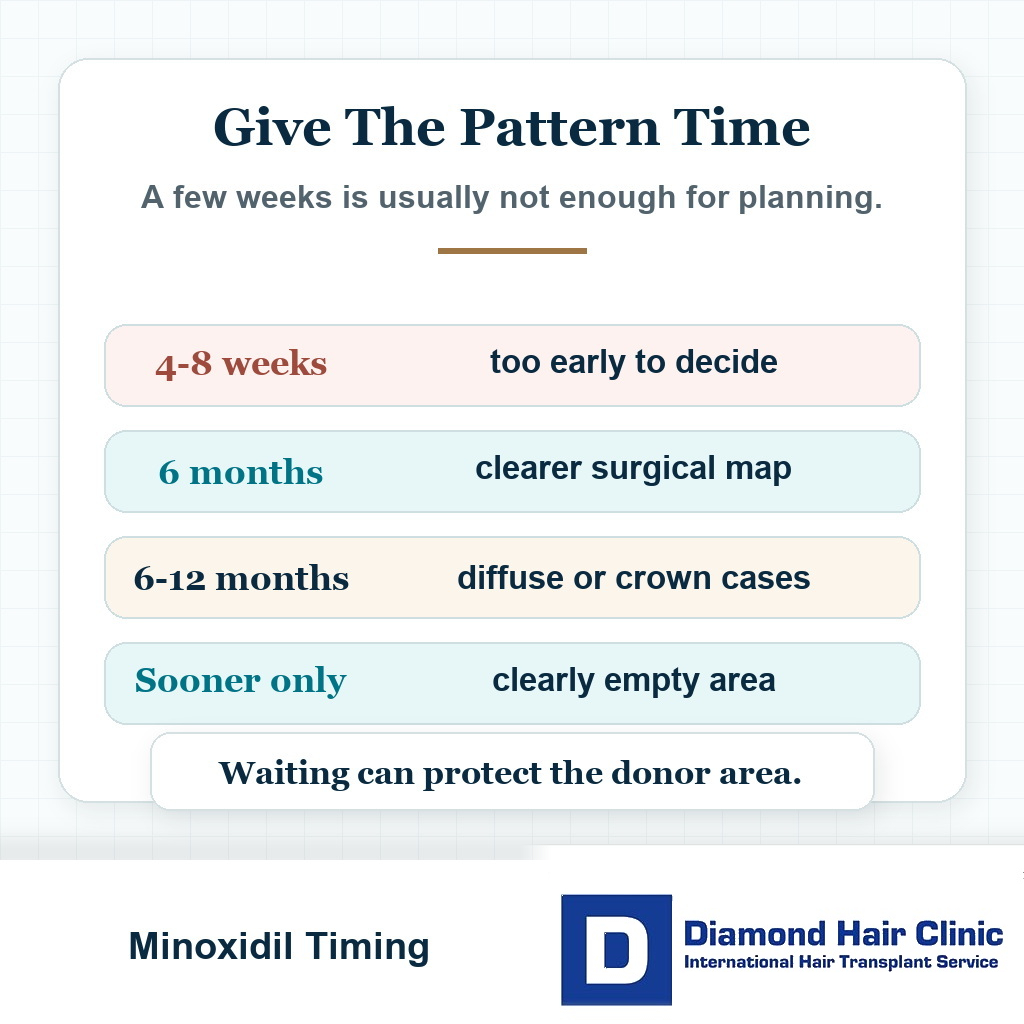
If you started or changed minoxidil within the last 1 to 3 months and the shedding is active, at least 6 months of observation is often safer. In diffuse thinning, crown thinning, or unstable hair loss, 6 to 12 months may give a more reliable surgical map. Surgery may still be reasonable sooner only when the area is already clearly empty, the donor area is strong, and the shed does not change the surgical plan.
This answer can feel frustrating. If you are already losing hair, waiting while more hair falls in the shower can feel like doing nothing. But surgery during a changing hair pattern can force the surgeon to make decisions with incomplete information.
Normal daily shedding is different from a sudden heavy shed after starting, stopping, or changing minoxidil. I am mainly cautious when the visible pattern is still moving, not when a stable pattern includes ordinary daily hair fall.
The question is not whether minoxidil is good or bad. In the right case, it can be useful. The same judgment applies later when deciding whether minoxidil after a hair transplant is part of maintenance or just another source of anxiety. The detail that matters is whether the hair you are seeing today is stable enough to plan surgery responsibly.
The broader question of medication before a hair transplant is not separate from this decision. Whether to pause minoxidil before surgery is part of the same timing discussion. If these decisions are handled casually, you may end up with more confusion, not more clarity.
This comes down to the pattern we are really seeing. Are we seeing the real hair loss pattern, or are we seeing a temporary medication reaction that is still unfolding? When that distinction is unclear, I handle still losing hair on medication before a hair transplant as a planning problem, not only a medication question.
When this is not clear, waiting is often not a delay. It is part of safer planning.
Shed timing sorter
Is shedding changing the surgical map?
Use this before choosing a date during an active minoxidil shed.
Wait for the pattern to settle before a large design decision. Consistent photos and a review point matter more than one frightening shower.
The useful split is recent medication change, pattern stability, donor limits, planned area, and pressure to choose a date.
Minoxidil shedding makes the surgical map less reliable
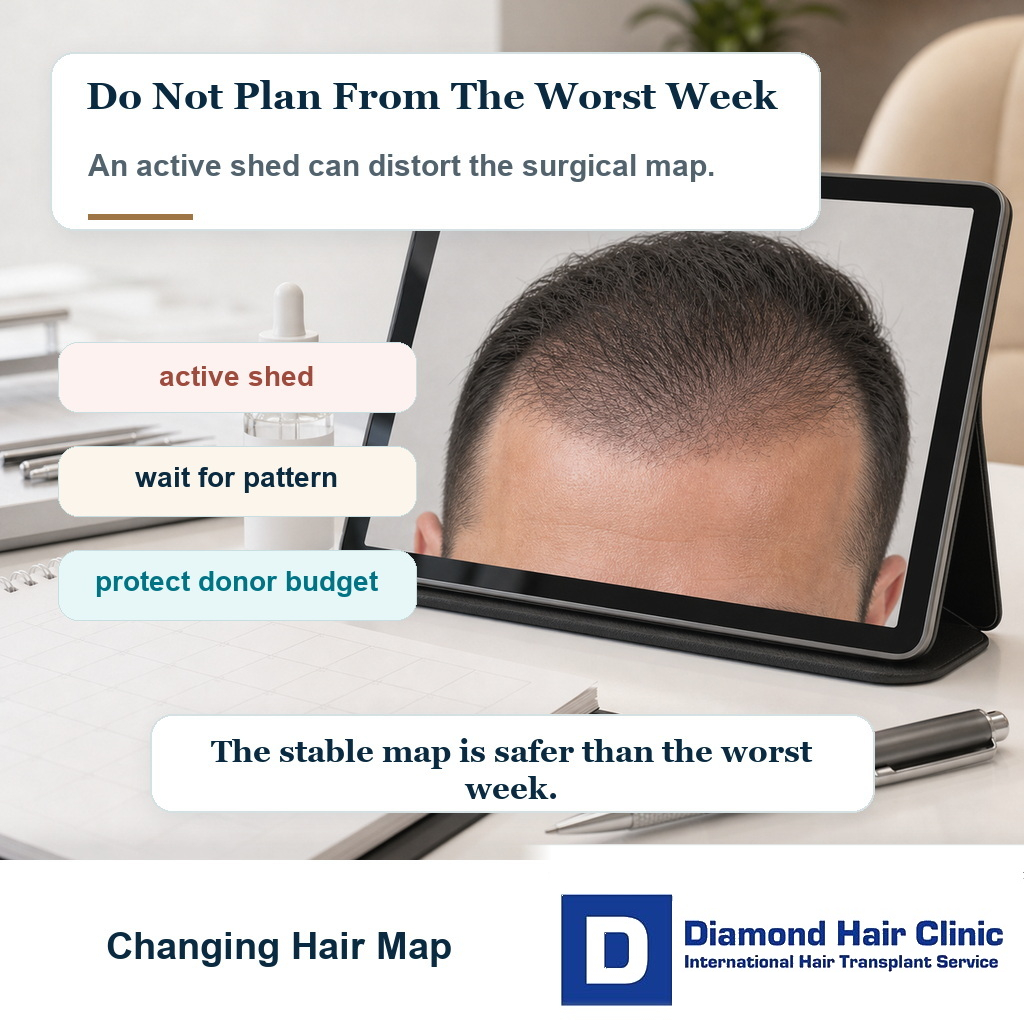
A minoxidil shed can make planning harder because it changes the visible map of the scalp. The surgeon needs to know which areas are truly empty, which areas still contain recoverable native hair, and which hairs are weak enough that they may not survive long term.
When shedding is active, the scalp may look worse than it will look later. If surgery is planned during that moment, the graft number may be estimated too aggressively, or grafts may be placed in areas that might have improved with time.
It matters because donor grafts are limited. A graft used today cannot be used again later. If the plan is built on a temporary shed rather than the real stable pattern, the donor area may be spent less intelligently.
The next issue is blending. Hair transplant surgery is not only about filling empty space. The real work is creating a natural relationship between transplanted hair and existing native hair.
If the native hair is temporarily missing because of a medication shed, the surgeon may see less native hair than usual. If that hair later returns, the area may become too crowded or uneven. If it does not return, you may need a different density plan.
Both possibilities matter. I do not plan surgery while the picture is moving too quickly unless there is a clear reason not to wait.
In surgical planning, uncertainty is not harmless. The more uncertainty there is before surgery, the more carefully the surgeon must protect donor supply, recipient area safety, and future options.
A rushed decision often asks only whether the operation can be done. A careful surgeon asks whether now is the right time to operate.
Observation time after starting or changing minoxidil
If you have just started minoxidil or changed the dose or form, 4 to 8 weeks is usually too early to read the final hair pattern. That is usually too soon for a reliable surgical decision. If the worry appears long after surgery, the review becomes closer to a transplanted hair thinning years later cause check, not only a minoxidil shed question.
For many people, 6 months gives a much more useful view. In diffuse thinning, crown thinning, or a very unstable pattern, 6 to 12 months can give better information.
The waiting period is not identical for every patient. The surgeon needs enough time to know whether the shedding is settling, whether miniaturized hairs are improving, and whether the hair loss pattern is becoming more stable.
The first weeks can be misleading. You may feel that medication is making the situation worse. In some cases, that worsening is temporary. In other cases, the hair loss was already progressing and the timing simply overlaps with the medication change.
Panic photos alone cannot decide surgery. The timeline, medication history, consistent photos, and a proper assessment of the donor and recipient areas all matter.
If you started oral minoxidil one month ago and are shedding heavily, committing to a large surgery immediately is usually premature. One month is not enough to understand the direction of the response.
If you have been stable for many months, the conversation is different. Stability does not mean zero hair fall. It means the pattern is predictable enough that the surgical plan is not being built on a temporary storm.
A properly timed operation is safer than an emotionally convenient date. A discount, a travel window, or an available surgical slot cannot decide the biology of the scalp.
Oral and topical minoxidil create different planning issues
Oral minoxidil and topical minoxidil create different planning issues. Topical minoxidil is applied to the scalp, so it can affect the skin surface with residue, dryness, irritation, flakes, or sensitivity. Oral minoxidil acts systemically, so the scalp surface issue is different. If pets share the home, that residue question needs a minoxidil pet safety plan before timing decisions are finalized.
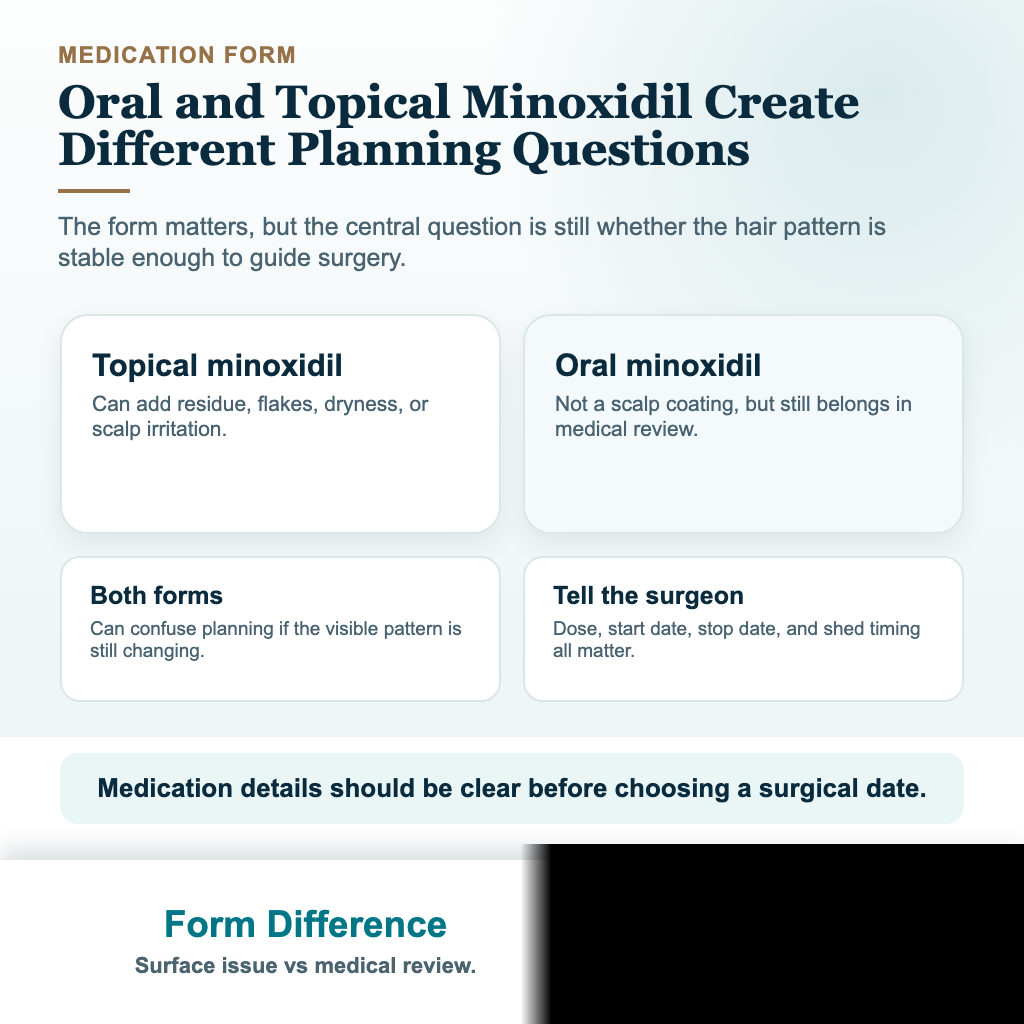
But from a planning point of view, both can create confusion if the hair is actively changing. This is not only about where the medication is applied. The detail that matters is whether the hair pattern is stable enough to guide surgery.
Some people switch from topical to oral minoxidil because topical use is messy or irritating. That reason can be understandable, but changing treatment shortly before surgery can create a new period of uncertainty.
If you switch medication and then book surgery soon afterward, the surgeon may be evaluating a scalp that is not in its steady state. That can affect graft count, density planning, and where the recipient area needs to begin and end.
Oral minoxidil also requires medical supervision. It is not simply a stronger version of a cosmetic lotion. Your general health, blood pressure, heart history, swelling tendency, dizziness, palpitations, and side effect risk need consideration by a qualified doctor.
Oral minoxidil must not be started casually because someone feels desperate before surgery. It also must not be stopped suddenly because shedding becomes frightening. Medication changes need to be deliberate, not emotional.
The best timing is decided before the surgical plan is finalized. If medication is part of the strategy, you and the surgeon need to know what you are waiting to see.
A practical plan needs a review point, a photo comparison, and a decision moment. Otherwise you are only taking medication and hoping the uncertainty disappears.
Surgery can still be reasonable in selected stable areas
Surgery can still be reasonable sooner when the transplant area is clearly bald or almost bald, the native hair pattern is not being distorted by active shedding, and the donor area is strong enough for the proposed plan.
For example, a mature frontal recession with very little native hair remaining in the planned recipient area may be easier to judge than diffuse thinning across the whole top. In that case, a medication shed may not change the surgical map as much.
Age also matters. A patient aged 45 with stable frontal recession is not the same as a patient aged 24 with rapid thinning and a family history of advanced baldness.
Candidacy comes before impatience. The wider question of being a good candidate for a hair transplant matters because not everyone who wants surgery is ready for the same plan.
A shorter wait may also be reasonable when you have already been on a stable medical plan for a meaningful period and only made a minor adjustment. But if the change has triggered heavy shedding, the plan needs more caution.
The size of the planned operation matters too. A small, conservative procedure may be less risky than a large operation that tries to redesign the hairline, fill the middle scalp, and chase the crown while the biology is still moving.
When surgery is done sooner, the plan needs to stay conservative. That means no aggressive hairline, no careless dense packing into weak native hair, and no promise that medication will solve every uncertainty afterward.
The answer is not always to wait one full year. The decision depends on what information is missing, how important that missing information is, and whether surgery can be planned responsibly without it.
Risks of operating while the pattern is changing
The first problem is wrong graft distribution. If the scalp looks thinner than it truly will after the shed settles, the surgeon may place grafts where they are not the best long term priority.
The second problem is underestimating future loss. If you are still actively miniaturizing behind the planned hairline, the transplant may look acceptable at first and then a gap between transplanted and native hair can appear later.
The third problem is confusing medication shedding with surgical shock loss. After surgery, you may shed more hair and panic. It becomes harder to know what came from medication, what came from surgery, and what came from the underlying hair loss process.
This overlaps with native hair shock loss after a hair transplant. When multiple causes of shedding overlap, you can lose all sense of timing.
The fourth problem is emotional. If you were already anxious during a medication shed, you may become much more anxious after surgery. The ugly phase can feel unbearable because the hair already felt unstable before the operation.
A hair transplant requires patience even in the best conditions. If surgery begins in the middle of panic, the months after surgery can feel much harder.
Another risk is repair surgery. If the first operation is planned around unstable hair, a second operation may be needed not because the grafts failed, but because the first plan did not respect the future pattern.
Repair work is always more difficult than proper first planning. It may involve scar tissue, limited donor supply, unnatural density transitions, and a more complicated emotional relationship with the result.
Timing is part of surgery. It is not separate from surgery. A good operation at the wrong moment can still become a disappointing plan.
Judging whether medication is helping the plan
Judge medication by pattern, timing, and clinical usefulness. If shedding starts shortly after a medication change and then gradually settles, that may be part of a treatment response. If thinning continues month after month with no sign of stabilization, that is different.
Photos matter, but they must be taken properly. The same lighting, same hair length, same angle, and same dryness level make the comparison more reliable. Wet hair, harsh light, and different camera distances can make the scalp look like a different person.
The key question is whether medication changes the surgical need. If the frontal area remains clearly empty, surgery may still be needed. If the middle scalp improves enough that fewer grafts are needed, waiting may have protected the donor area.
Minoxidil mainly supports growth and hair cycling. It does not replace treatment aimed at DHT in many men with male pattern hair loss. The discussion sometimes overlaps with hair transplant without finasteride.
Finasteride is not mandatory for every patient. The surgeon still needs to understand what is controlling the underlying hair loss, what is only improving hair appearance, and what remains unstable.
A medication response can be helpful even if it does not remove the need for surgery. If it clarifies the true size of the recipient area, improves weak native hair, or makes the crown less urgent, it has already helped the plan.
On the other hand, medication can confuse the plan if it is started too close to surgery and creates active shedding without enough review time. The surgeon then has to decide whether today’s thinness is permanent or temporary.
That is not a small detail. It changes graft number, density strategy, and whether to treat now or observe longer.
Stopping minoxidil before the operation
This depends on the form of minoxidil and the surgeon’s protocol. Do not make this decision alone the night before surgery.
Topical minoxidil is often paused around the operation because the scalp needs to be clean, settled, and free of irritation. The timing question of whether to stop minoxidil before a hair transplant needs to be handled before the operation, not guessed at the last moment.
The question is different with oral minoxidil because it is not placed on the scalp surface. Oral medication still needs medical review. Discuss it with the doctor who prescribed it and the surgeon who will operate.
Stopping medication suddenly can create more shedding and more confusion. Continuing medication without telling the surgeon is also not intelligent. The surgeon needs to know what you are taking, when you started, when the shedding began, and whether the dose or form changed recently.
If surgery is already scheduled and you are shedding heavily, discuss the timing directly instead of pretending the shed does not matter. Sometimes the operation can proceed. Sometimes postponement is the better medical decision.
What concerns me is secrecy. Some people hide medication changes because they are afraid the surgeon will cancel the date. That is a mistake. A surgeon cannot protect what he does not know.
If a clinic does not ask about medication, recent shedding, or hair loss stability before taking payment, that is not reassuring. It suggests the clinic is selling a procedure more than planning a surgery.
A surgeon led clinic needs to be willing to pause, reassess, and change the plan when the biology of the scalp changes.
Use these slides to compare medication timing, stable zones, disclosure, shedding related to stopping, and review before booking.


Shed after stopping minoxidil also matters
A shed after stopping minoxidil can be just as important as a shed after starting it. If hair was being supported by minoxidil and you stop, some of that hair may weaken or shed. That can make the scalp look worse and can change how the surgical plan is judged.
Stopping minoxidil simply to expose every weak area before surgery sounds logical on paper, but in real life it can create months of instability and emotional panic. It can also make the surgeon plan around a temporary reaction rather than a settled pattern.
Stopping because of irritation, side effects, pregnancy planning, blood pressure concerns, or another medical reason should be reviewed properly. When the only reason is impatience before surgery, I slow the decision down rather than create a new shedding problem.
The key question is whether the hair loss pattern after stopping has stabilized. If shedding is still active, the map is still changing. If the pattern has settled and you do not plan to restart, the surgical design can be discussed more.
Do not create a medication shed just to make a transplant decision faster. A clearer plan comes from stability, not from forcing the scalp into a crisis.
Diffuse and crown thinning need more caution
Diffuse thinning makes this decision more delicate. In diffuse thinning, the recipient area may still contain many native hairs, but many of them may be miniaturized or unstable.
If you have diffuse thinning and hair transplant concerns while actively shedding from medication, the decision becomes more cautious. The surgeon may not be looking at the true stable density of the native hair.
Transplanting between existing hairs can be done, but it requires careful judgment. If the native hair is unstable, the surgery may cause more shock, and the final appearance may not match your expectation.
The crown also needs patience. A crown hair transplant consumes grafts quickly, and the visual reward can be slower and less dramatic than the front. If medication may improve crown coverage, waiting can sometimes change the plan significantly.
This is especially true when the crown is not completely bald. If there are many weak miniaturized hairs, medication response can help the surgeon decide whether the crown needs grafts now, fewer grafts later, or no surgery yet.
You may feel you cannot wait because the crown bothers you every day. That feeling is understandable. But the crown is also one of the areas where impatience can spend donor supply quickly.
The frontal hairline is more visible socially, so people often push for a fast decision there. The crown is emotionally frustrating because it shows in photos and under light. Both areas need planning, but they do not always deserve the same urgency.
If the hair is actively shedding, assess the crown, middle scalp, and frontal zone together and separately. That pattern helps decide whether the weak point is medication timing, ongoing androgenetic loss, or both.
Surgeon questions before choosing a date
Before choosing a date during or soon after a minoxidil shed, the visible pattern must be stable enough for surgical planning. The main issue is whether we are seeing true empty space, temporary shedding, or a pattern that may still change with time.
If the medication response improves, the planned recipient area may shrink. If the shedding continues, the graft number or hairline design may need to change. Waiting a few months can sometimes give a clearer map and protect the donor area from being used too early.
Your medication timeline should be clear before payment or travel. If you recently started oral minoxidil, changed from topical to oral, stopped treatment, restarted treatment, or had heavy shedding, bring that timeline into the consultation before the surgery date is chosen.
This broader caution is part of what needs to be clear before you book a hair transplant. Booking is not just choosing a date. It is accepting a plan.
A responsible plan needs to explain what happens if medication improves the hair, what happens if it does not, and what happens if the native hair continues to thin after surgery. If the clinic only says to do it now without discussing those possibilities, the answer may be convenient for the clinic rather than protective for you.
Practical plan while shedding is active
When shedding is active after starting or changing minoxidil, I pause the booking decision and document the next few months. Consistent photos, medically supervised medication use, and time make the pattern clearer than a rushed surgery date.
If the surgery is not urgent, at least 6 months after the medication change is often safer before making a major surgical commitment. For some people, 6 to 12 months gives a better view of whether the hair is stabilizing, improving, or still progressing.
When a surgical date is already booked, speak to the surgeon directly. Do not let fear of losing the slot make the decision for you. A careful surgeon would rather adjust the timing than operate on a scalp that is giving unclear information.
If your recipient area is clearly empty, your donor area is strong, and the shed does not change the plan, surgery may still be reasonable. But that needs to be a clinical judgment, not your guess under stress.
The central principle is simple. Do not let a temporary medication shed create a permanent surgical decision.
A hair transplant can be a very good solution when the timing, donor management, and design are correct. But it is still surgery. It needs planning from the most reliable version of your hair loss pattern, not from the most frightening week of shedding.
Patience here is not delay for its own sake. It protects the donor area, preserves future options, and helps avoid a result that solves today’s panic but creates tomorrow’s problem.
The recommendation is plain. If the hair pattern is actively changing, let it settle unless there is a clear surgical reason not to wait. A more stable pattern gives a better plan, and a better plan often gives you a more natural result.