


Different causes can create the same visible gap
A hair transplant does not treat the scalp as one flat surface. The surgeon places follicular units into a specific recipient area, while the surrounding native hair may be shaved differently, shocked temporarily, miniaturizing slowly, or already thinner than it looked before surgery.
In the first days, the most common cause is visual contrast. The recipient area is trimmed very short so graft placement can be controlled. Nearby native hair may be a different length. Scabs and redness can sharpen the border. Under bright light, a normal transition can look like a white strip.
That is different from a narrow plan that only filled the obvious bald area while ignoring weak hair behind it. If the transition zone was left untreated or unplanned, the patient may later see a strip between growing grafts and native hair.
Diagnosis comes first. Before surgery, the surgeon has to decide whether the patient is a good candidate for a hair transplant and whether the native hair behind the planned recipient area is stable enough to support the design.
An early border is often temporary during recovery
In the first two weeks, a gap often looks more serious than it is. Scabs, swelling, redness, skin color contrast, and different shaving lengths can all sharpen the line between transplanted and native zones.
A reassuring sign is the presence of short native hairs inside the area you call a gap. If the skin looks healthy and small hairs are still visible, the area may simply be passing through an early visual phase.
Shock loss can also create a temporary gap. Native hairs around the recipient area may shed after surgical trauma, inflammation, anesthesia, and incisions. Many of those hairs recover when they were strong before surgery.
Weak miniaturized hairs are less predictable. They may shed and return slowly, return thinner, or sometimes fail to return in a meaningful cosmetic way. Miniaturization is not a detail to discover after surgery. It has to be judged during planning.
During the first weeks, the priority is not to inspect every millimeter all day. Protect the grafts, wash correctly, avoid trauma, and follow hair transplant aftercare. Increasing pain, spreading redness, pus, fever, strong odor, blackening skin, or worsening bleeding needs quick clinic review.
A persistent strip can suggest a planning problem
A persistent strip becomes more concerning when it follows the exact shape of the surgical design and remains visible after the hair has had enough time to mature.
A natural transplant should not look like a patch placed in front of another scalp. The front needs to connect with the mid scalp. The temples need to connect with the frontal hairline. The crown should not be treated as an isolated circle without respect for the hair around it.
A low or strong hairline request still has to be weighed against future safety. Low and flat hairlines become especially risky when the hair behind them is unstable or when donor reserve cannot support the density needed later.
A rushed design can create a density cliff. The transplanted part may be too dense at the front while the native hair behind it is too thin to support that strength. The result may not look bald, but it can look artificial because the eye notices a sudden change.
Too few grafts are not always the problem. Sometimes grafts were used in the wrong priority. A result that blends well comes from understanding how one zone visually supports the next.
Native hair loss can open a new space later
Yes. Transplanted hair is usually taken from the safer donor area and is expected to be more resistant to male pattern hair loss. Native hair on the top of the scalp is different. It may continue to miniaturize after surgery.
That means a technically successful transplant can still develop a gap later. The grafts may survive and the new hairline may grow, while native hair behind it keeps thinning.
This is not always a surgical failure. It can be the biology of progressive hair loss. But it needs to be discussed before surgery, especially in younger patients, diffuse thinning patients, and patients with a family history of advanced baldness.
A very low, very strong hairline can therefore be risky in a young patient. If the mid scalp is unstable, solving today’s insecurity can create tomorrow’s gap.
Medical treatment may matter for some patients. Finasteride, dutasteride, minoxidil after hair transplant, or other options may be discussed depending on diagnosis, health, tolerance, age, and risk profile. I do not force every patient into the same plan, but I do explain that surgery alone does not protect native hair.
A crown hair transplant needs separate planning. The circular growth pattern, changing hair direction, and future thinning around the crown can make gaps more visible if the plan is too aggressive or too isolated.

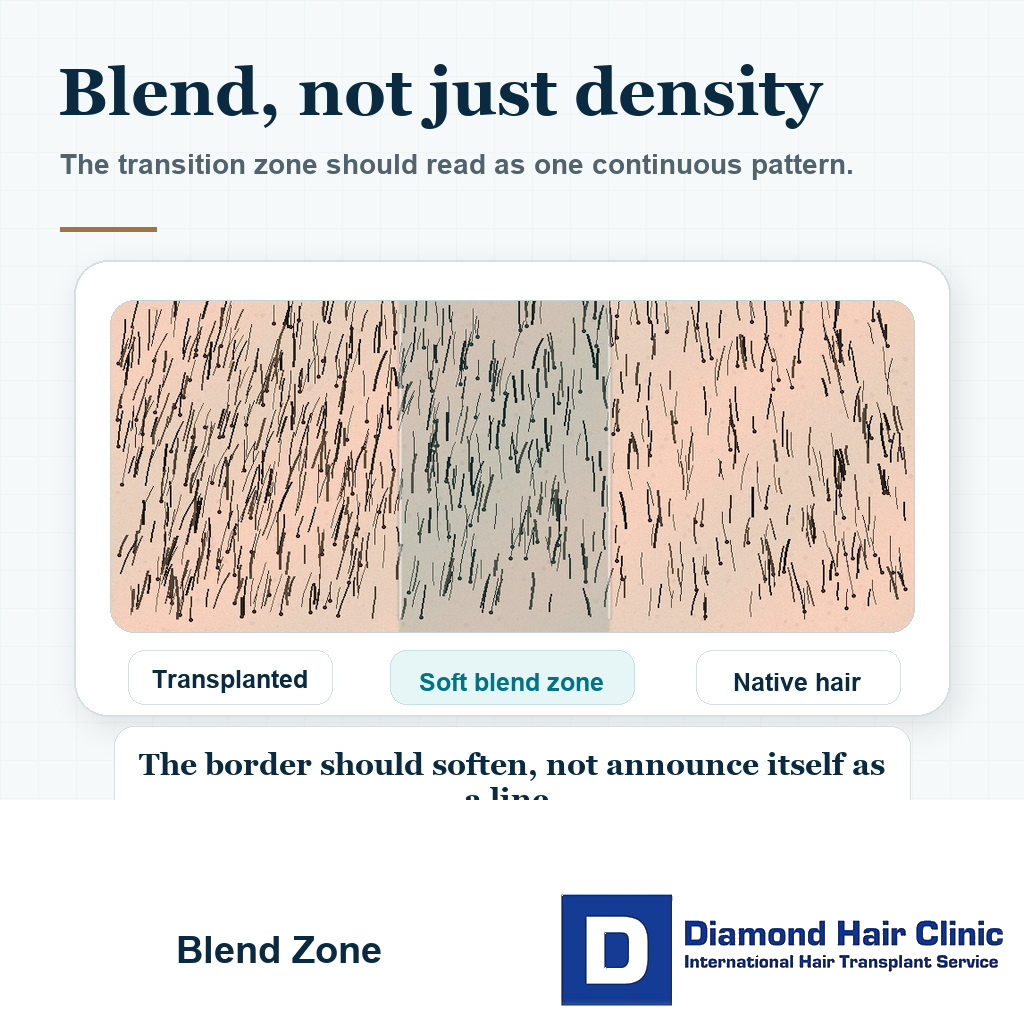
A blend zone needs softness instead of a wall
Many people think every visible gap needs more density. In the transition zone, blending often matters more than raw graft count.
Hair direction, angle, caliber, color contrast, curl, skin tone, and native hair quality all affect how the transition reads. If transplanted hair points one way and native hair behaves another way, the border can look wrong even when the graft count is not low.
A hair transplant cannot be planned through numbers alone. Graft numbers matter, and I explain how I calculate graft numbers, but the number is only one part of the decision.
A soft transition uses careful irregularity, angle control, respect for existing hair direction, and enough judgment to avoid a dense block in front of weak native hair. A smaller number of grafts placed intelligently can look more natural than a larger number placed without a visual plan.
Some transplants look good in one photo and thin in another. Lighting, wet hair, short haircuts, and camera angle can reveal the transition more clearly. Thin looking hair transplant results often come back to distribution and blending, not density alone.
Questions before accepting a hairline or crown design
Before accepting a hair transplant plan, do not ask only how many grafts are needed. Ask what will happen to the native hair behind the transplant if hair loss continues.
Ask whether the current hair loss is stable. Ask whether the design will still make sense if more native hair is lost over the next few years. For the hairline, ask how the front will connect to the temples and mid scalp.
For the crown, ask whether crown coverage is the right priority now or whether the frontal area should be stabilized first. Many people want everything in one session, but donor area limits force priorities.
For diffuse thinning, ask whether transplanting between existing hairs is safe in this specific case. If the recipient area is full of miniaturized hair, shock loss and future thinning need direct discussion before surgery.
Responsibility matters here. A hairline or crown plan should come from someone who understands blending, native hair loss, donor limits, and future thinning. At Diamond Hair Clinic, planning comes before graft numbers. Hairline design in hair transplant is a medical and aesthetic responsibility, not decoration.

Safe timing for repairing a gap
Repair depends on timing, donor reserve, and whether native hair is still actively thinning. Sometimes a gap can be repaired very well. Sometimes it can only be improved. The answer depends on donor capacity, scalp condition, previous graft placement, hair quality, and skin scarring.
If the gap is simply underfilled and the donor area is healthy, a second session may soften the transition. The repair plan should avoid an overloaded block of density and make transplanted and native areas read as one continuous pattern.
If the hairline was placed too low, repair becomes more complex. Adding grafts behind a low hairline may help coverage, but it may also spend donor hair trying to support a design that should have been more careful from the beginning.
If the donor area has already been overused, repair options become narrower. Every graft spent badly reduces future options. Repair surgery also requires patience, because a rushed repair can make a difficult case harder.
At 4 or 5 months, it is usually too early to call the result final. Uneven growth is common. Some areas wake earlier, and some areas grow later. At 12 to 18 months, a persistent gap becomes much more useful to evaluate in person.