


Native Hair Shock Loss Needs Recovery Context
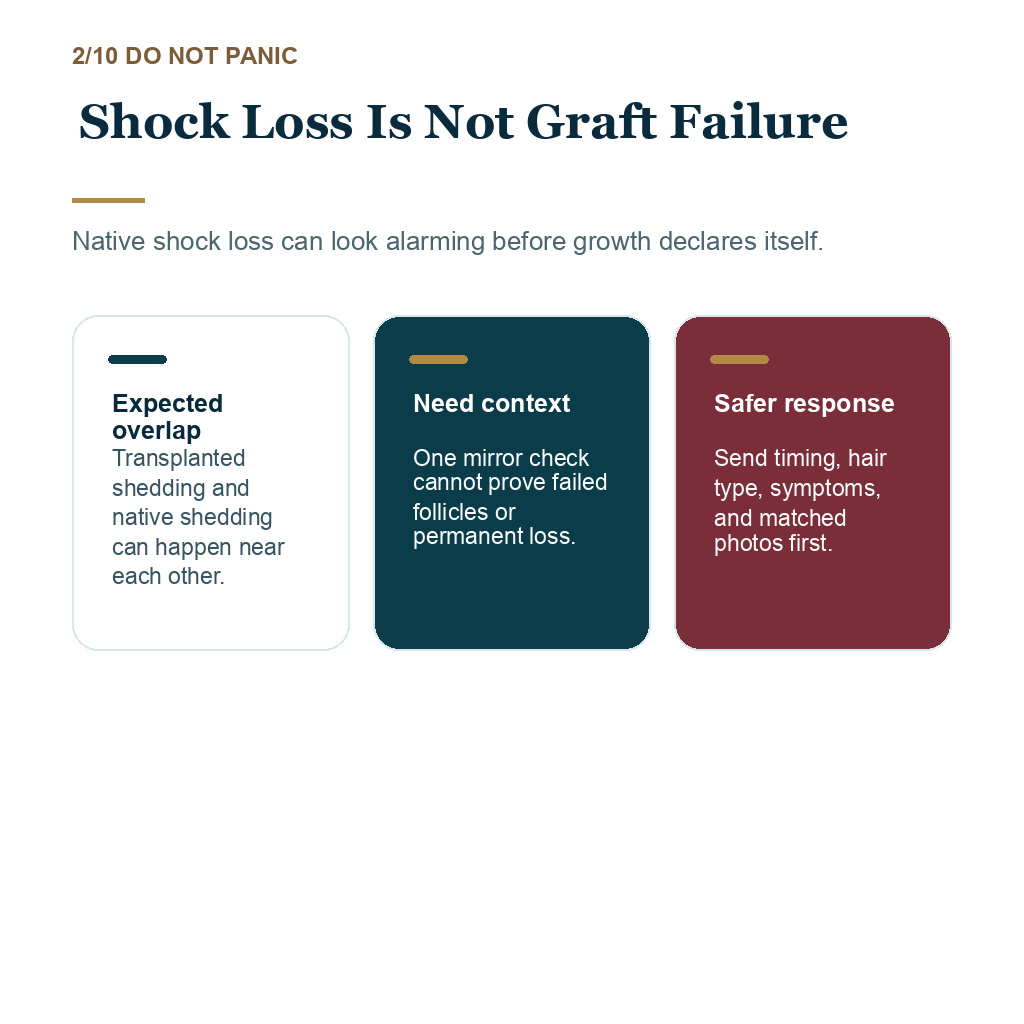
Temporary thinning around the recipient area can be frightening, especially when existing hairs were still present between the grafts. It can mean existing hairs near the transplanted area have been pushed into shedding by surgery, swelling, inflammation, or work between fragile miniaturized hairs. It does not by itself mean the grafts failed, and it should not be judged from one frightened mirror check.
The important step is to separate transplanted shaft shedding, native hair shock loss, and ongoing pattern hair loss. Short newly moved shafts, longer original hairs, diffuse shedding, scalp symptoms, medication changes, and matched photos can point to different explanations. Then I can decide whether the right response is controlled waiting, medication review, closer follow-up, or medical examination.
If the hairs you are losing are longer original hairs rather than short transplanted shafts, that detail matters. It does not prove permanent loss, but it tells me the concern may involve native hair or diffuse shedding rather than the transplanted grafts themselves.
If you are worried now, do not scrape, pull, or test the grafts. Send matched photos, the surgery date, medication changes, and any scalp symptoms so the shedding pattern can be judged properly.
Shedding interpretation map
Match the shedding pattern before judging failure
The first question is what type of hair is falling, where it is happening, and whether the timing fits transplanted shaft shedding, native shock loss, diffuse shedding, or a scalp problem.
Transplanted shaft check
Short shafts shedding does not prove graft failure
Short newly moved shafts falling during early recovery, often after scabs loosen and the scalp looks suddenly emptier.
Use the timeline and matched photos instead of judging from one mirror check.
Do not scrape, pull, or test the area to prove whether follicles are alive.
The shaft can shed while the follicle remains under the skin. Timing and appearance matter.
Native shock loss is different from transplanted shedding
After FUE, transplanted shafts often shed during the early recovery period. Those hairs are usually short, newly moved shafts. The follicles remain under the skin and enter a quieter phase before new growth starts. That pattern can make the recipient area look empty even when the grafts are alive.
Native shock loss is different. It affects hairs that were already growing in the recipient or nearby scalp before surgery. You may feel, “I had more hair before the transplant, and now the original hair around the grafts looks thinner.” That fear is understandable, especially when the implanted zone was placed into an area that still had some existing density.
The distinction is important because the advice changes. Transplanted shedding is expected. Native shock loss is a stress response in existing hair. Direct injury to existing follicles is a different concern, and I would not diagnose that from shed hairs alone. Ongoing androgenetic loss is the disease continuing in the background. These can overlap, which is why a quick answer from a single photo is often misleading.
Some native hairs are more vulnerable
The native hairs most likely to shed are usually the hairs that were already miniaturized. They may have looked useful in normal lighting, but under magnification they were thin, short, or unstable. Surgery, local swelling, work in the recipient area, anesthesia, and inflammation can push those hairs into shedding sooner than expected.
For that reason, I do not judge only the number of grafts a person wants. I look at what will happen to the hair that remains between those grafts. Dense packing into a zone with weak native hair can make the early weeks look worse before they look better. The visual result at one or two months can be emotionally difficult, even when the surgical plan was reasonable.
Some shocked native hairs return. Some hairs that were already near the end of their miniaturization path do not return with the same strength. The quality of the native hair before surgery decides much of the risk. Assessment before surgery is not a formality. It shapes the entire recovery conversation.
Timing can fit shock loss
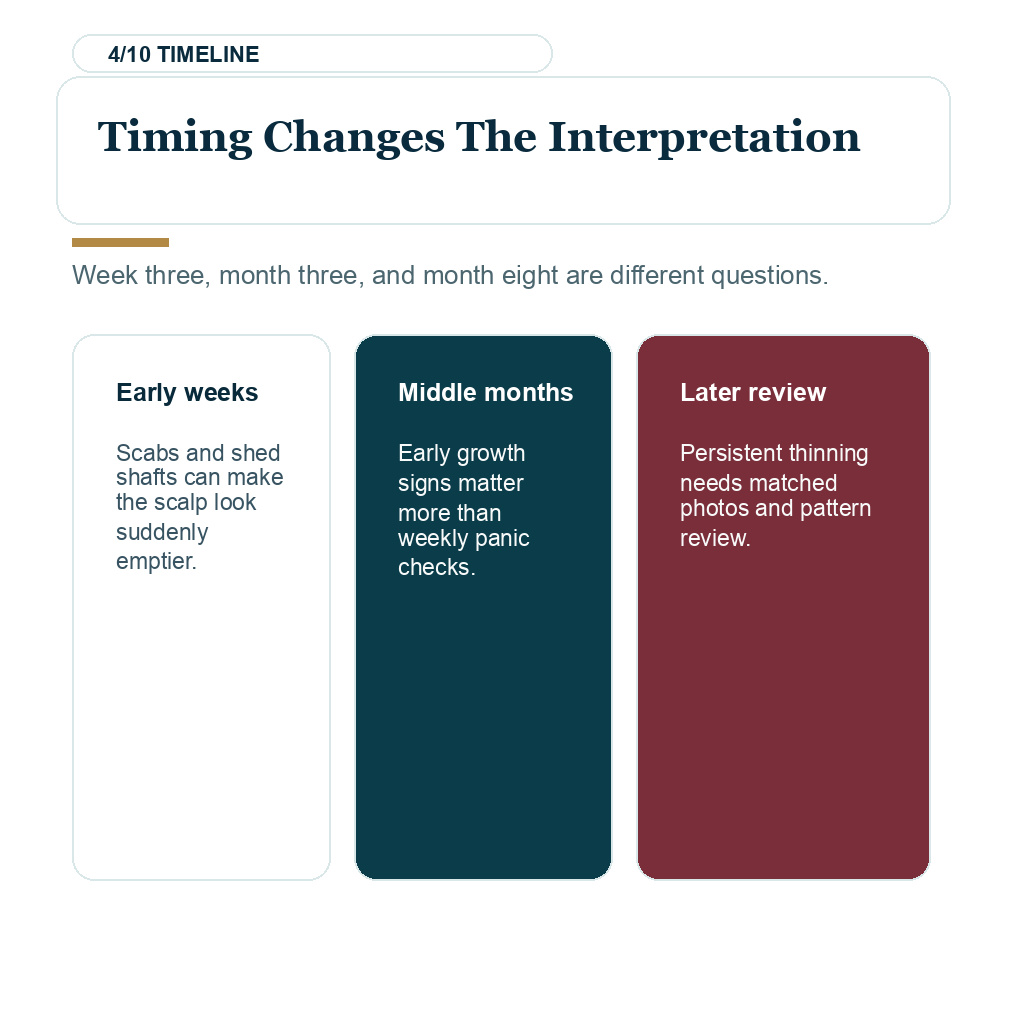
Shock loss usually becomes noticeable after the early healing period, not on the first day. The first several weeks can look worse because transplanted shafts shed, scabs are gone, and the scalp suddenly looks bare. Native shock loss can add to that impression when longer existing hairs start to fall around the transplanted area.
General telogen shedding after physical or emotional stress can appear later as well. A broader discussion of telogen effluvium around hair transplant timing is useful when the shedding is diffuse rather than limited to the implanted zone. The timing matters because the same complaint at week three, month three, and month eight can have different meanings.
By month four or five, I expect to see early signs of new growth rather than final density. If you compare every week, recovery can feel stalled even when the timeline is still normal. Pages about low density at four months after hair transplant and the month five growth check are better for judging early growth, while this article focuses on the native hair that seemed to disappear around surgery.
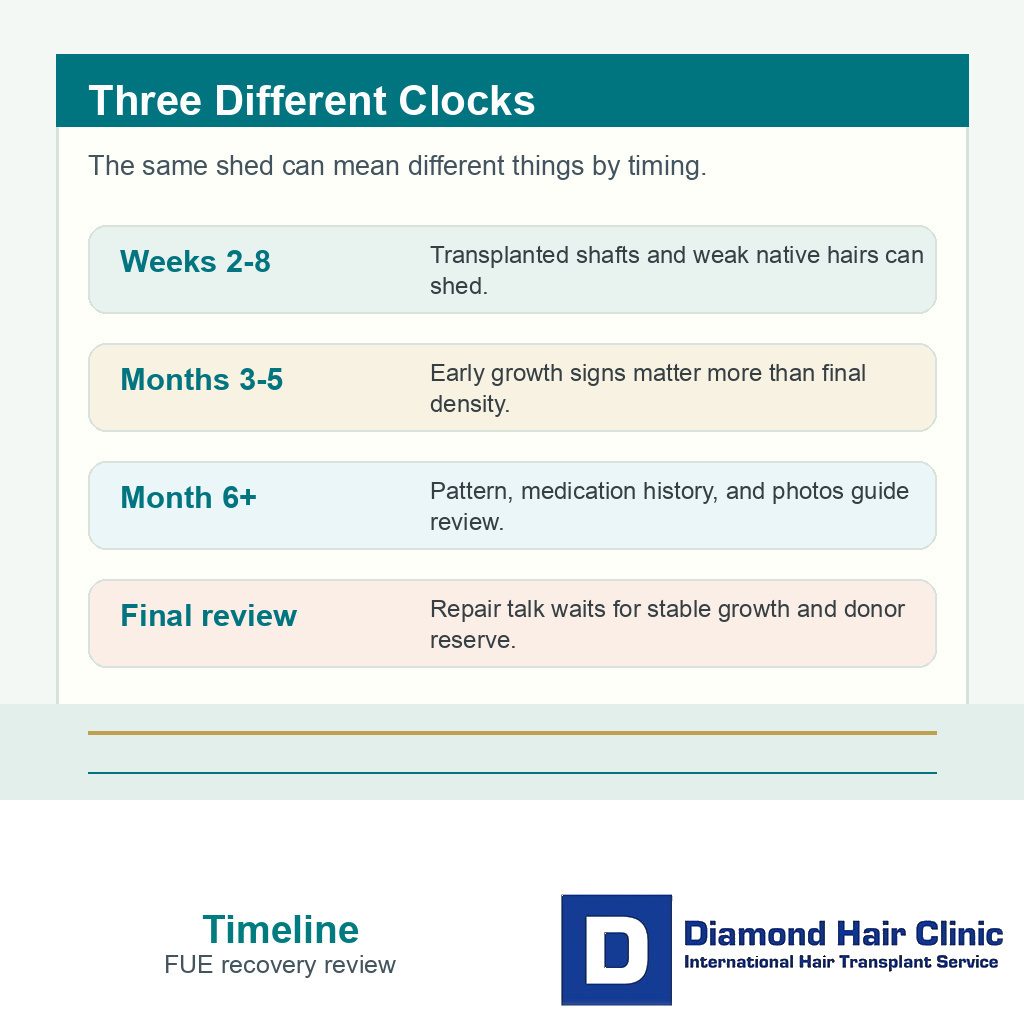
Transplanted shedding, native shock loss, and later growth review are related, but they are not the same checkpoint.
Use the 10 shedding interpretation slides below to separate short transplanted shafts, longer native hairs, weak native hair risk, timing, matched photos, medication history, diffuse shedding, scalp symptoms, donor shedding, and why repair talk is usually too early. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.






Photos can show whether the area is truly worse
Shock loss is often judged in a bathroom mirror, under harsh lighting, with wet hair, or after cutting the surrounding hair shorter. That comparison is not reliable. Matched photos are more useful. I need the same angle, the same light, the same hair length, the same camera distance, and no product in the hair.
Useful photos show the frontal hairline, mid scalp, temples, donor area, and a top down view. A close crop of only the thinnest spot can exaggerate the fear. A wider set of photos tells me whether the thinning is limited to the recipient field, spreading through native zones, or part of a general shedding event.
This is also where the before photo has to be judged in context. If the before surgery hair looked fuller because it was long, styled forward, or photographed in low light, the comparison after surgery may feel unfair. Good follow-up uses matched evidence, not the most frightening image.
Medication history can change the interpretation
Medication history is one of the first things I check. Starting finasteride, stopping finasteride, changing minoxidil, pausing treatment because of travel, or switching supplements around surgery can all make shedding harder to interpret.
If hair loss was unstable before surgery, native hair can keep miniaturizing while the grafts are recovering. That situation belongs close to the question of still losing hair on medication before or after a transplant. The surgery did not create the entire pattern. It happened while the pattern was still active.
Medication decisions should not be made in panic after a shed. If side effects are the worry, review the plan in detail, including the realistic role of finasteride side effects in hair transplant planning or over the counter choices such as saw palmetto before and after hair transplant. The goal is to avoid changing treatment on your own during the most confusing phase of recovery.
Diffuse thinning needs stricter review
Native shock loss is easier to understand when it sits around the recipient area. Diffuse thinning is different. If the whole scalp looks thinner, if the sides or crown are changing at the same time, or if shedding is heavy in the shower, I look beyond the surgery field.
Diffuse hair loss may involve androgenetic hair loss, telogen effluvium, nutritional issues, thyroid problems, inflammatory scalp disease, or medication changes. A transplant can still be planned in some diffuse thinning cases, but the diagnosis and long term donor strategy must be stricter. The separate page on diffuse thinning and hair transplant planning is important before anyone assumes every shed hair is only shock loss.
The mistake is treating all after surgery shedding as harmless. Most early shedding is not an emergency, but a broad change in hair quality deserves a proper review. During review, I want to know where the loss is happening, how fast it changed, and whether the scalp itself looks healthy.
Scalp symptoms can change the urgency
Shock loss should not come with severe scalp illness. Mild redness, sensitivity, or dryness can be part of recovery, but worsening pain, spreading redness, discharge, fever, crusting that looks infected, or scaling that does not settle should be reviewed quickly.
When the scalp has unusual inflammation, the question is no longer only cosmetic density. Infection, dermatitis, psoriasis, folliculitis, or scarring scalp disease can change the plan. If the story is unclear, clinical examination, dermoscopy, lab work, or in selected cases a scalp biopsy before hair transplant decisions may be needed before the plan is made or revised.
Contact the clinic if symptoms are getting worse instead of better. Photos help, but symptoms matter. A message with the date of surgery, current medications, temperature if fever is suspected, and clear photos is more useful than ten anxious close-ups without context.
Donor shedding is a different concern
The phrase shock loss is sometimes used for both recipient thinning and donor area changes. Donor shock loss can happen, but it is a different concern from native hair thinning in the recipient field. The donor area has its own healing pattern, extraction density, and long term limits.
If the back or sides look patchy, I check whether the issue is temporary shedding, overharvesting, inflammation, haircut contrast, or simply early healing. That belongs closer to the discussion of when donor hair does not grow back after FUE. Mixing donor questions with recipient native shock loss can lead to the wrong conclusion.
For this article, the main question is the native hair in and around the implanted area. Donor area concerns should still be documented, but they should not be used as proof that the recipient grafts failed.
Repair talk is usually too early in the first months
When you feel worse than before surgery, it is easy to jump straight to repair. I understand that reaction. Still, repair talk in the first months can create more harm than clarity. The scalp has not shown its final growth, native hair may still recover, and the donor area should not be used again before the first operation has declared itself.
Later milestones matter, but they answer different questions. Six month density after hair transplant and shedding between months six and eight after FUE are useful when the concern is growth direction or later shedding. Native shock loss in the early months is not the same as a final density failure.
A second surgery should be considered only after the surgeon can see stable growth, stable native hair behavior, and enough donor reserve. Early anxiety should trigger documentation and follow-up, not rushed graft planning.
A useful review separates photos, medication changes, scalp symptoms, and timing before deciding what the shedding means.
Useful information helps the review
For a native hair shock loss review, send the surgery date, graft number if known, and the exact areas transplanted. Also tell me your current medicines, recent medicine changes, and whether there is pain, redness, scaling, discharge, fever, or heavy shedding outside the transplanted area.
I also ask for photos taken in a disciplined way. Front, left, right, top, donor, and a close view of the worried area are usually enough. The hair should be dry, without fibers or styling product. If you have before surgery photos from the clinic and your own phone, I compare both because clinic lighting and home lighting can tell different parts of the truth.
The emotional side matters too. Constant checking can become part of the problem, especially after the first shed. The page about mirror checking after hair transplant can help when the behavior itself is making recovery harder. If the anxiety feels overwhelming, the related discussion of the emotional crash after hair transplant recovery may be more useful than another close-up photo.
This stage needs a cautious decision
If the scalp is quiet, the shedding is near the transplanted area, and the timing fits early recovery, the usual decision is to document the change, keep follow-up photos, protect the medical plan, and wait for the growth window. That is not passive. It is controlled observation during a phase when the appearance can be misleading.
This is not the stage to test grafts or plan repair. Document the pattern clearly and let the timeline declare itself unless warning signs are present.
If thinning is diffuse, symptoms are worsening, medication history is unstable, or photos show a pattern that does not fit simple shock loss, the decision changes. You need clinical review rather than social media guessing. Sometimes the review is reassuring. Sometimes the medicine plan needs adjustment through the right doctor. Sometimes the scalp needs treatment before any cosmetic judgment is made.
Native hair shock loss after FUE is frightening because it can make surgery feel like a step backward. My job is to separate fear from evidence. I do not promise that every weak native hair returns. I also do not label an early shed as failure before the scalp, photos, medication history, and timeline have been reviewed properly.