Telogen Effluvium and Hair Transplant Timing
A hair transplant is usually not the right next step while telogen effluvium is still active. Telogen effluvium is a shedding problem before it is a graft problem. If the shedding is recent, heavy, unexplained, or changing month to month, surgery should wait until the trigger has been reviewed and the visible pattern is stable enough to plan safely.
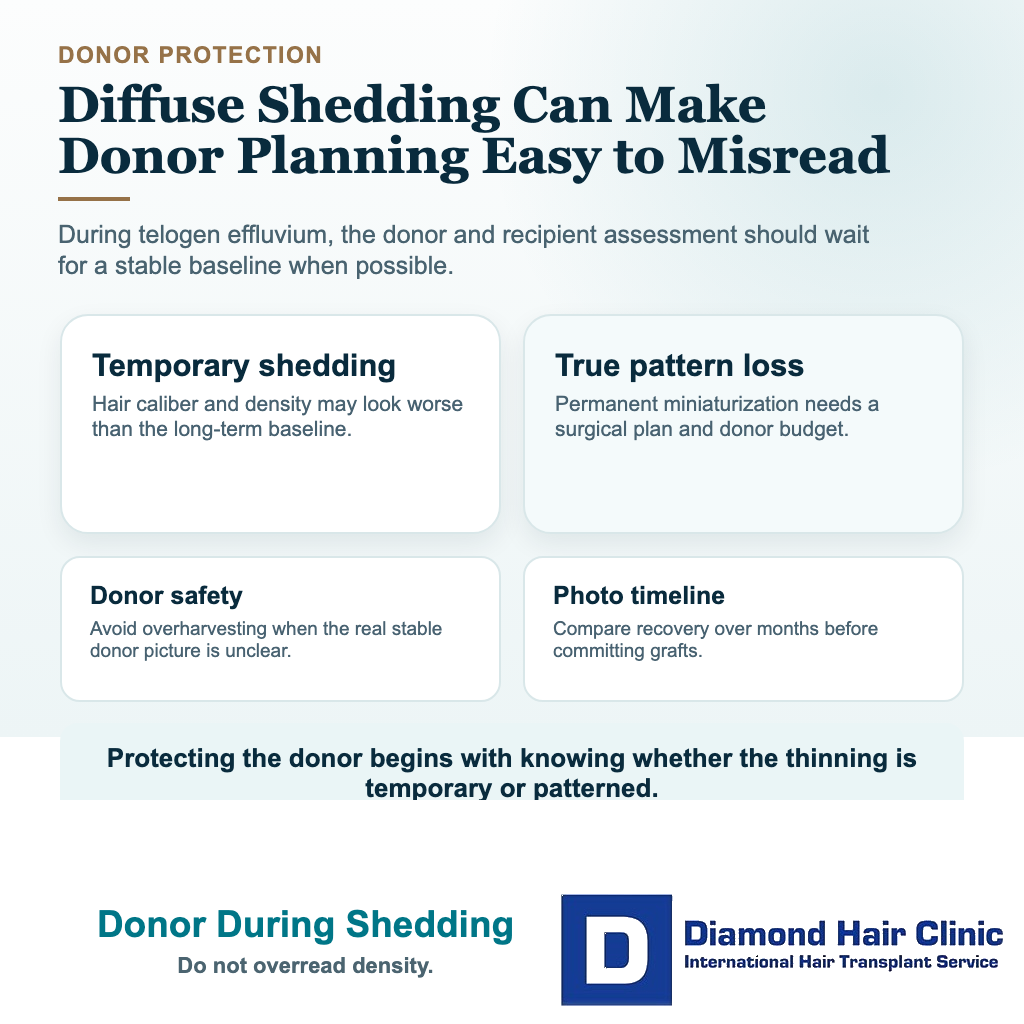
I separate active shedding from a stable permanent pattern. Active shedding can make the whole scalp look worse than it really is. A stable pattern can be planned more responsibly. After surgery, a related concern is native hair shock loss after FUE, where existing recipient hair may shed around the grafted area. Once the shedding has settled, surgery may become reasonable if a permanent hairline, mid scalp, crown, or density problem remains.
I understand why this feels urgent. Seeing hair in the shower, on the pillow, or in your hands can make you feel that the chance to fix it is slipping away. But a frightening wash day, a Close up photo, or one bad week should not decide a donor plan. If we operate while the picture is distorted, we can choose the wrong area, the wrong graft number, or the wrong hairline design.
Telogen effluvium differs from pattern hair loss
Telogen effluvium usually means many hairs have shifted into a shedding phase after a trigger such as illness, fever, major stress, childbirth, rapid weight loss, crash dieting, thyroid imbalance, iron deficiency, an inflammatory flare such as Crohn disease or ulcerative colitis, methotrexate or another medication change, or major surgery around a hair transplant.
The follicles are often still alive, but the timing of the hair cycle has been disturbed. That is different from androgenetic pattern hair loss, where susceptible hairs slowly miniaturize over time. Telogen effluvium is often delayed, so the shedding may appear one to several months after the trigger instead of on the same day.
A hair transplant can move donor grafts into an area where hair has been permanently lost. It cannot stop a temporary shedding process that is still active across the scalp. With telogen effluvium, the first job is to understand the trigger and wait until the scalp picture becomes readable again. If shedding is mixed with male or female pattern hair loss, the permanent part may be treated surgically later, after the temporary part is separated from it.
A temporary shed can look like transplanted hair thinning years later, so the trigger and timing should be separated before surgery is considered.
This distinction protects donor hair. Donor grafts are limited. If grafts are used during a temporary shedding phase, we may spend them on an area that would have recovered, or we may underestimate another area that will need treatment later. The same caution applies to diffuse thinning and hair transplant planning, because the visible scalp alone does not always tell the full diagnosis.
Surgery should wait while shedding is active
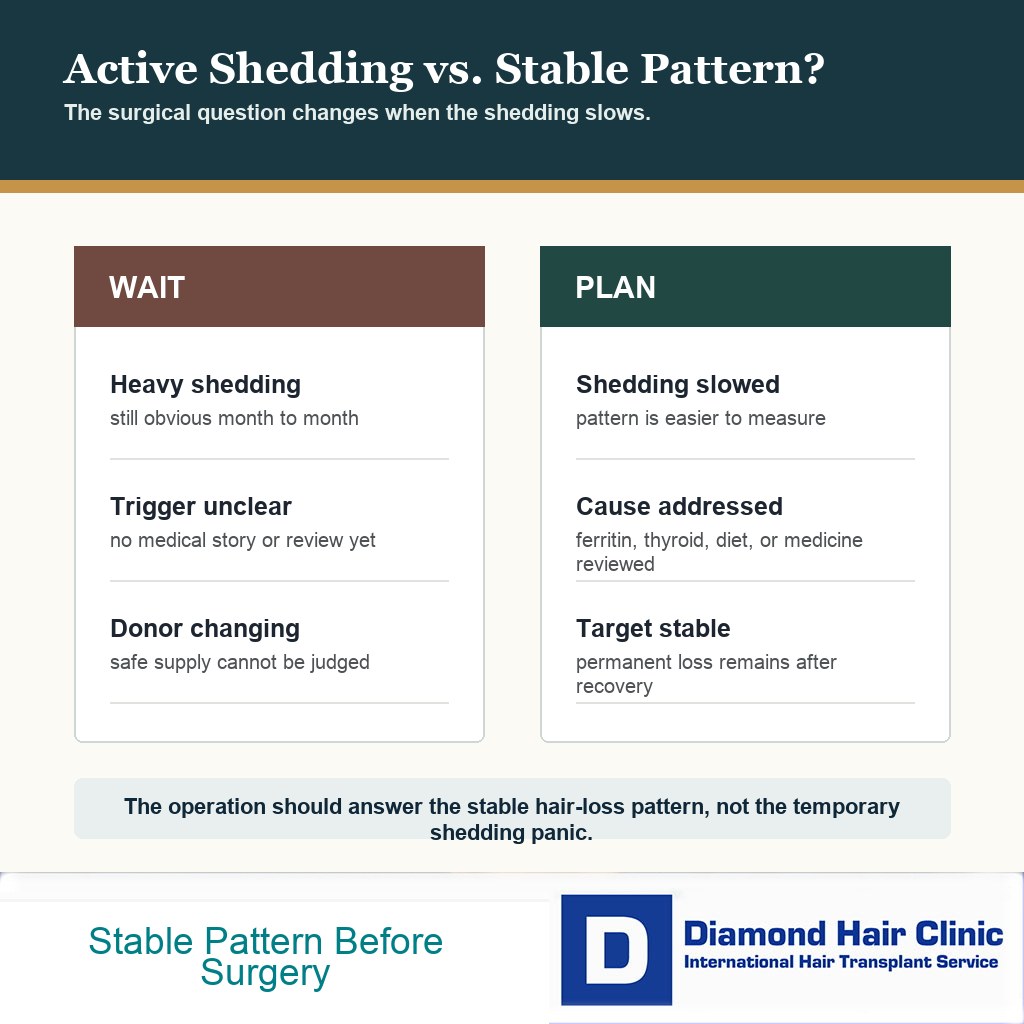
Surgery should wait when shedding is still heavy, the cause is unclear, the donor area is also changing, or likely triggers have not been medically reviewed. If the shedding began after fever, COVID infection, crash dieting, weight loss surgery, childbirth, iron deficiency, thyroid disease, a new medication, pregnancy, or IVF treatment, the timing of surgery should respect that story.
I am also cautious when the hair looks different every week. A transplant plan needs a stable target. If the hairline, mid scalp, crown, and donor area are changing quickly, the plan becomes guesswork. Surgery should not be used as a way to escape uncertainty. It should be done when the uncertainty has been reduced enough that the operation is actually serving you.
For some people, the safer delay is a few months. For others, especially with nutritional deficiency, thyroid disease, postpartum shedding, medication changes, chronic illness, or active hair loss, the delay may need to be longer. I do not give one fixed waiting period to everyone because the responsible answer depends on the trigger, recovery pattern, examination, donor area, and whether androgenetic hair loss is also present. A hormonal contraception change can be one of those timing clues, so birth control and hair transplant planning should not be separated from the shedding history.
If shedding continues beyond the expected recovery window, I do not simply keep waiting without a plan. Persistent diffuse shedding needs diagnosis. That may mean blood tests, medication review, scalp examination, trichoscopy, or dermatology input before donor grafts are used.
Useful blood test context usually means more than one number. If testing was done, send the full report with dates and reference ranges, especially thyroid markers, ferritin or iron status, CBC, vitamin or nutrition results, and any abnormal result your doctor is following. If nothing has been checked yet, say that clearly rather than guessing the trigger.
Active shedding has to be judged by trend
The first sign is the story. When did the shedding start? Was there a fever, infection, stressful event, childbirth, new medicine, stopped medicine, rapid weight change, low protein intake, or new medical diagnosis one to several months before it appeared? Telogen effluvium often has a delay between the trigger and the visible hair fall, so the cause is not always obvious on the day you first notice shedding.
The second sign is the pattern. Telogen effluvium often feels diffuse. Hair comes out from many areas, and the change is usually a sudden drop in volume rather than one clean bald spot. Pattern hair loss usually has a more recognizable distribution, such as temples, frontal hairline, mid scalp, crown, or a widening part. The two can overlap, so a consultation should not rely on one photograph, one anxious week, or one shower where more hair came out than usual.
The third sign is measurement over time. I compare current photos with older photos, examine the donor area, look for miniaturization when needed, and ask whether shedding is slowing. If the story suggests anemia, thyroid disease, nutritional deficiency, postpartum shedding, or another medical trigger, blood tests before a hair transplant can be part of safe planning rather than a formality.
Track the trend in a way that can be compared. Take front, mid scalp, crown, sides, and donor photos in the same lighting, with the same hair length and styling when possible. Write the date beside each set. Counting every hair after every wash usually increases anxiety. Repeated comparable photos and the story around them are more useful for planning.
The trend matters more than a single count. A high shedding day can happen during recovery and still settle. Repeatedly worsening volume, a changing donor area, or a new medical trigger is different. The pattern needs to be stable enough that the surgical plan is based on the real scalp, not on a temporary low point.
Improving shedding can still leave the scalp looking thin
Timing matters here. If shedding has clearly slowed but the scalp still looks thin, I do not judge the final transplant plan from the first quiet week. I check for short regrowing hairs, repeated photo stability, a readable hairline/crown pattern, and whether the donor area has returned to its usual appearance.
Recovery can lag behind the end of shedding. Short regrowing hairs, less hair fall, and steadier photos are encouraging, but they do not instantly prove the final density. The surgical question becomes clearer only after the temporary low point has passed and the remaining pattern can be examined without panic lighting or wet hair exaggeration.
If the donor area is also thinner than usual, surgery should wait. Donor grafts come from a limited area, so the scalp picture needs to be stable before that reserve is used. Operating while the donor looks artificially weak can lead to an overly cautious plan. Operating while the recipient area looks artificially empty can lead to an overly aggressive plan. Both mistakes come from reading the scalp too early.
When shedding has settled and a stable pattern remains, the decision becomes more surgical. At that stage, being a good candidate for a hair transplant depends on the remaining pattern, donor strength, age, hair caliber, medical history, and whether future loss has been planned for.
Transplant can help only when real balding remains
But the order matters. Telogen effluvium can reveal a pattern that was already there. A man may notice that after shedding improves, the frontal corners or crown still look thin. A woman may notice that after postpartum or nutritional shedding settles, the part line remains wider or the frontal hairline still lacks density. In those cases, a transplant may help the permanent pattern, not the temporary shedding itself.
The consultation has to answer two questions separately. How much of the current loss is likely to recover with time or medical correction? How much represents stable permanent thinning that donor grafts can improve? If those questions are mixed together, the plan becomes too aggressive or too vague.
For example, low ferritin can create active shedding and also sit beside androgenetic hair loss. Correcting ferritin may not restore every weak area, but it can make the true pattern clearer. I treat low ferritin or anemia before a hair transplant as a planning issue, not only a laboratory number.
Thyroid disease and postpartum shedding need medical context
If thyroid disease is involved, the thyroid problem should be diagnosed, treated, and stable enough that the shedding pattern can be judged. Surgery cannot correct uncontrolled thyroid related shedding. It may still have a role later if a permanent hair loss pattern remains, but the medical condition comes first.
After pregnancy, shedding can be dramatic, and it can make surgery feel urgent. Most of the time, the safer first step is to let the shedding settle, review breastfeeding and medication questions safely, and then decide whether the remaining pattern is truly surgical. The dedicated page on postpartum hair loss and hair transplant timing goes deeper into that situation.
Weight loss is another common trigger. After bariatric surgery or rapid weight change, protein intake, ferritin, vitamins, general health, and shedding stability all matter. If the body is still adjusting, a transplant can be technically possible but strategically unwise. The timing logic is similar to the one I use when planning a hair transplant after weight loss surgery.
Existing bookings may need to pause
If you already booked surgery and shedding suddenly becomes heavy, do not hide it from the clinic. Send clear photos in consistent lighting, explain when it began, and describe any recent illness, childbirth, diet change, weight loss, new medicine, stopped medicine, thyroid issue, low ferritin, or severe stress. A delay is better than an operation planned on a misleading scalp picture.
Also explain what has changed since the booking. That includes new blood tests, a new diagnosis, a new medication, stopped minoxidil, started minoxidil, changed contraception, recent fever, crash diet, or major stress. A plan that was reasonable before the shedding started may not be the same plan today.
Travel pressure is real, especially when flights, hotels, deposits, and time away from work are already arranged. Still, donor grafts are more valuable than a booking date. If the diagnosis is unclear, postponing can protect the long term result. It is better to lose time than to use grafts in the wrong surgical moment.
If shedding is already slowing and the remaining pattern looks stable, the answer may be different. In that case, photos, medical history, donor quality, and expectations can show whether surgery has a stable target. The decision should be made from evidence, not panic. After scalp radiation, the same separation matters because hair transplant after scalp radiation only makes sense once the permanent patch is clear.
Donor plan needs protection during uncertainty
Donor hair is the limited reserve that must last through future hair loss. Telogen effluvium can temporarily change how much hair appears to be missing, while androgenetic alopecia can continue for years. A surgeon led plan has to protect the donor area from both mistakes.
The first mistake is chasing all visible thinning as if it is permanent. The second mistake is assuming everything will recover and ignoring a real pattern of hair loss. The middle path is careful diagnosis. The stable target, likely future pattern, donor strength, age, and medical story all have to be reviewed together.
Medication may be part of the discussion when androgenetic hair loss is present. Every person does not need the same medicine, but the long term plan should be clear. Some cases can still be planned without medical support, but the design has to be more conservative. That same tradeoff applies to having a hair transplant without finasteride.
Telogen effluvium can happen after transplant surgery too
Hair shedding after surgery can involve transplanted hairs and native hairs, but the meaning is different from active shedding before surgery. After a transplant, many grafted hairs shed as part of the early cycle while the follicle remains under the skin. Native hairs around the work can also shed temporarily from surgical stress. Native hair shock loss after a hair transplant can then become part of the discussion.
Before surgery, the concern is planning. If the scalp is already shedding heavily, the surgeon may not be seeing the true baseline. After surgery, the concern is recovery and interpretation. These are related topics, but they are not the same decision.
The difference matters in practice. Preoperative telogen effluvium can distort the map before grafts are used. Shedding after surgery has to be interpreted against a known surgical plan, healing timeline, and graft cycle. Those are different problems, so they should not be explained with the same quick reassurance.
No one should be told that every shed hair is harmless. Warning signs after surgery still matter, including fresh bleeding, worsening pain, discharge, spreading redness, fever, open wounds, or symptoms that worsen instead of settling. But surgery planned at the right time begins with a clearer diagnosis before surgery, and that is the point telogen effluvium forces us to respect.
The carousel below separates temporary shedding from a stable pattern that can be planned surgically. Swipe sideways, use the arrows, or choose a number below the image.