



IBD and Hair Transplant Surgery Safety
A hair transplant may be possible with Crohn disease or ulcerative colitis, but timing depends on medical stability. I do not decide from the diagnosis name alone. I look at current symptoms, last flare, bleeding or diarrhea, weight change, hydration, infection history, medicines, blood tests, nutrition, and the gastroenterologist’s view.
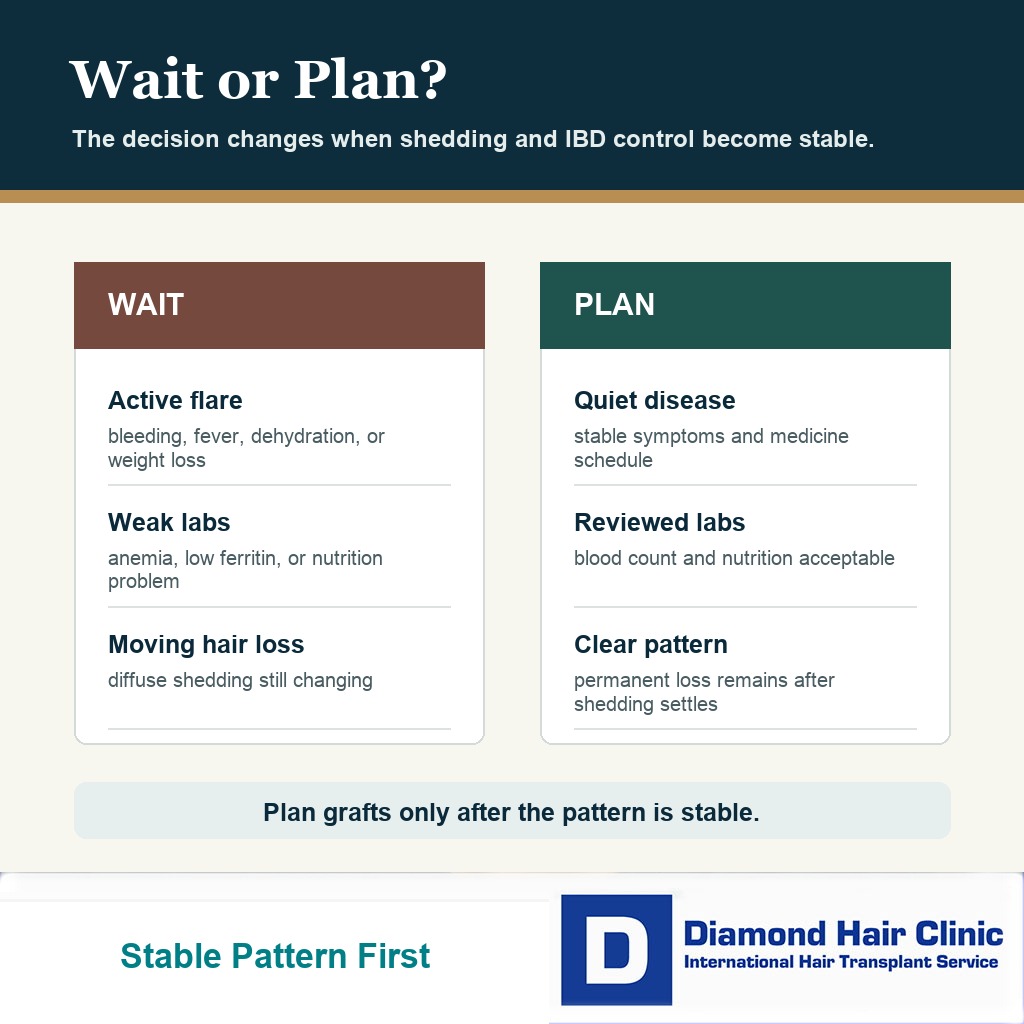
Stable remission or quiet disease is very different from an active flare. If you are eating and drinking normally, without fever, not losing weight, not bleeding, not dehydrated, and not changing immune treatment suddenly, surgery can sometimes be planned carefully. If there is severe diarrhea, rectal bleeding, fever, dehydration, recent hospitalization, recent bowel surgery, active infection, significant anemia, or diffuse shedding after illness, waiting protects both health and donor grafts.
The IBD label is only the starting point. I need to know whether your body is stable enough for an elective surgical day and whether the thinning is permanent pattern loss rather than temporary shedding after a flare or nutritional stress.
Surgery is most reasonable when IBD is quiet
Hair transplant surgery is most reasonable when inflammatory bowel disease is under control and you feel physically well enough for a long elective procedure under local anesthesia. The bowel symptoms, medication plan, scalp condition, donor area, and hair loss diagnosis all need to fit together.
The word stable matters more than the label Crohn disease, ulcerative colitis, or IBD. Someone in long remission on a steady medicine plan is in a different position from someone who has just had a flare, new bleeding, dehydration, weight loss, or a hospital admission.
I also separate IBD from scalp autoimmune disease. Crohn disease and ulcerative colitis do not normally attack scalp follicles in the same way as some scarring scalp diseases, but they can still affect timing through inflammation, nutrition, medication, infection risk, and temporary shedding. With autoimmune disease and hair transplant surgery, the diagnosis name alone is never enough to judge safety.
For IBD, I am asking a practical surgical question. Can the scalp heal predictably after thousands of small donor and recipient area openings, and can we identify the permanent hair loss pattern clearly enough to plan grafts responsibly?
Surgery should wait when IBD is active or health is unstable
Surgery should wait if you are in an active flare, have fever, active infection, severe diarrhea, dehydration, unexplained weight loss, fresh rectal bleeding, significant anemia, or a recent major medication change. These are not small cosmetic details. They change how your body may tolerate the operation and the first days of healing.
I also slow the plan down after recent hospital treatment, recent bowel surgery, a new abscess or infection, high dose steroids, or a flare that has not yet been properly controlled. A hair transplant is elective, so the date can be chosen when the body is not fighting a larger medical problem.
A delay after flights, hotel plans, or time off work are arranged can feel frustrating. If the health change appears after booking, the safer path is to treat it as a medical change after booking a hair transplant, not as a minor inconvenience. The donor area is limited. If the body is under stress and the hair loss pattern is unclear, a rushed operation can spend grafts on the wrong problem.
When medicine timing is uncertain, I connect the decision with the same discipline used for medication before a hair transplant. Do not stop prednisone before a hair transplant, azathioprine, methotrexate, mesalamine, Humira or other biologics before a hair transplant, JAK inhibitors, or other prescribed IBD medicine just to make surgery feel simpler. The doctor treating your bowel disease needs to be involved when a change is being considered.
IBD can be linked with hair loss
Crohn disease and ulcerative colitis can be connected with hair loss, but not always in a way that surgery can fix immediately. A flare, blood loss, iron deficiency, low B12, low folate, poor nutrition, rapid weight loss, major stress, surgery, or medication change can push hair into temporary shedding.
Temporary shedding can be frightening because it feels sudden and visible. Seeing hair in the shower or on the pillow can make a transplant feel urgent. But if the shedding is active and diffuse, surgery may be the wrong first step because the donor and recipient planning are being judged during a moving medical event.
Telogen effluvium before a hair transplant matters here because illness or nutritional stress can create delayed shedding. Donor grafts should not be used until the trigger has been reviewed and the pattern becomes clearer.
A permanent male or female pattern can still exist in the same person. IBD does not protect someone from genetic hair loss. The surgical decision becomes reasonable only after the temporary component and the permanent component are separated.
Steroids, biologics, and immune medicines change planning
IBD medicine changes planning because it tells me how active the disease has been and what risks need respect. Mesalamine, steroids, immunomodulators, biologics, antibiotics, JAK inhibitors, and other immune medicines do not all mean the same thing. The names, doses, timing, reason for use, and recent changes matter.
A stable maintenance plan is different from treatment being escalated because the disease is still active. A biologic that has kept the bowel disease quiet for years is different from a biologic that has just been started after a severe flare. A medication pause ordered by your gastroenterologist is different from stopping medicine alone because you are afraid the clinic will refuse surgery.
Stable maintenance treatment is different from treatment being changed because the disease is moving. I become more cautious when the medication plan and the hair loss picture are both changing at the same time.
I do not give a universal stop date for IBD medicine in a hair transplant article. That would be unsafe. The timing should be handled by the treating gastroenterologist and the surgeon together, especially if the medicine affects infection risk, wound healing, blood count, liver tests, kidney function, or immunity.
Share the exact drug names, doses, injection or infusion schedule, last dose date, recent flare history, recent infections, and whether your gastroenterologist considers the disease controlled. A clear medical story is much safer than a hidden medication list.
Biologic dose or steroid timing needs coordination
Do not move or skip an IBD medicine dose by yourself to make a hair transplant date easier. A missed biologic dose, sudden steroid stop, or unplanned medicine break can make bowel control worse. A flare around surgery is often a bigger problem than the medicine schedule itself.
The reason for the medicine matters. A stable maintenance biologic with good blood results and no infection is a different situation from a high dose steroid course started because of a recent flare. When the drug plan has just changed, or there is fever, an abscess, active infection, severe diarrhea, or poor nutrition, the transplant should wait until the gastroenterologist confirms that the timing is sensible.
Bring the injection or infusion dates, current dose, recent blood results, and any planned taper. In a complex case, it may be better to schedule the transplant between treatment dates, or to delay surgery so bowel disease control is not sacrificed for a cosmetic calendar.
Blood tests and nutrition problems that matter before surgery
Blood count, iron status, ferritin, B12, folate, vitamin D, inflammatory markers when relevant, liver function, kidney function, albumin or nutrition markers when requested, and infection screening may all matter in an IBD case. The exact panel depends on your history. The question is simple. Can the body heal, and is the hair loss being driven by a correctable medical problem?
IBD can cause iron deficiency through inflammation or blood loss. Crohn disease involving the ileum, or previous ileal surgery, can make B12 absorption more difficult. Poor intake during a flare can add another problem. If these issues are significant, a transplant plan based only on scalp photos is incomplete.
General blood tests before a hair transplant still matter, and IBD adds a specific question about anemia, low ferritin, low B12, low folate, inflammation, and poor nutrition because these may be part of the reason the hair is shedding in the first place.
If the issue is low iron or anemia, the more focused page on low ferritin, anemia, and hair transplant timing is directly relevant. Correcting the medical weakness first may protect both healing and the surgical plan.
IBD risk depends on disease control and healing reserve
IBD by itself does not mean poor healing after a hair transplant. Many people with controlled Crohn disease or ulcerative colitis heal normally after minor procedures. The risk changes when the disease is active, nutrition is poor, the blood count is weak, infection is present, or medicine that suppresses immunity needs special coordination.
Hair transplantation creates many small wounds, but it is not the same as bowel surgery. Even so, I do not dismiss healing risk just because the operation is performed under local anesthesia. The scalp still needs clean healing, and the body still needs enough general reserve to recover well.
With immune treatment, the answer is not panic and it is not automatic clearance. Fever, active infection, recent antibiotics, recent hospitalization, current steroid exposure, skin problems, and the gastroenterologist’s view all matter before elective surgery.
After surgery, warning signs such as worsening pain, spreading redness, pus, fever, or feeling unwell should trigger contact with the clinic rather than guessing. With infection after a hair transplant, the direction of symptoms matters, especially when they worsen instead of settling.
Antibiotics and stomach sensitivity need a plan
Antibiotics before a hair transplant need extra thought when there is Crohn disease, ulcerative colitis, previous C. diff, severe diarrhea after antibiotics, allergy, tendon pain, rash, swelling, or hospitalization after antibiotics. Also mention whether your gastroenterologist has told you to avoid a specific antibiotic.
Do not refuse every antibiotic by default, and do not silently take a tablet that has caused a serious problem before. The safer path is a plan before surgery, with the surgeon and the doctor managing the bowel disease aware of the risk.
If antibiotics are prescribed after the operation, take them as directed or contact the clinic before changing them. With antibiotics after a hair transplant, side effects and infection protection both need communication.
Diarrhea after hair transplant surgery should not be ignored in someone with IBD. Mild stomach upset and severe watery diarrhea are not the same. Blood in stool, fever, dehydration, weakness, or severe abdominal pain belongs in medical review, not only in a hair transplant aftercare conversation.
Details to send before arranging travel
The clinic needs the exact diagnosis, whether it is Crohn disease or ulcerative colitis, when the last flare happened, whether you have bleeding or diarrhea now, and whether you have been hospitalized or had bowel surgery recently. Send the current medicine list and the latest relevant blood results if the clinic requests them.
For travel to Turkey, mention a flare, severe diarrhea, new bleeding, dehydration, recent biologic infusion, steroid taper, antibiotic reaction, or abnormal blood test before flights are arranged, not on the morning of the operation. Travel makes timing mistakes more expensive and more stressful. It is better to postpone early than to arrive tired, dehydrated, and medically unsuitable. The usual instructions before hair transplant surgery still matter, but IBD adds another layer because medication timing, hydration, bowel symptoms, and blood results can change the decision.
Travel planning can also include blood clot risk questions when the disease is active, after hospitalization, after recent surgery, or when there is leg swelling. Most people with IBD do not need special medication for this alone. Warning signs such as calf swelling, chest pain, or shortness of breath belong in the medical conversation before the trip.
Photos of the scalp are helpful, but they are not enough for IBD. I need the medical context behind the hair loss. If the hair became thin after a flare, hospitalization, weight loss, poor eating, or medication change, that timeline matters as much as the hairline photo.
Bring or send the names of your medicines, recent test results, allergy history, antibiotic reaction history, and the contact details or written opinion from your gastroenterologist when the case is complex.
The 4 slides here make the travel and medical details easier to check before planning surgery. Swipe sideways, use the arrows, or choose a number below the image.
Temporary shedding must be separated from transplantable hair loss
I separate temporary shedding from transplantable loss by looking at the timing, pattern, donor area, miniaturization, and medical story. Hair loss that starts two or three months after illness, flare, severe stress, poor eating, anemia, or surgery may behave differently from long term male or female pattern loss.
If thinning is diffuse across the whole scalp, I become more cautious. A diffuse thinning hair transplant needs careful diagnosis because the donor area itself may be part of the problem, or the visible thinning may be moving too quickly to plan safely.
Other medical causes can imitate or add to shedding related to IBD. Thyroid disease is one example, and the same diagnostic discipline applies to hair transplant planning with thyroid disease. Medical treatment may need to come first, then surgical planning later if a stable permanent pattern remains.
When shedding settles, some people realize they do not need surgery yet. Others are left with a clear hairline, crown, or density problem that surgery can address. Waiting does not waste time when it prevents the wrong operation.
Decision should involve both doctors
The best decision separates two responsibilities clearly. Your gastroenterologist judges bowel disease control, medication safety, anemia, nutrition, infection risk, and whether the timing is medically reasonable. The hair transplant surgeon judges donor capacity, hair loss diagnosis, hairline design, graft planning, and whether the scalp can be operated on responsibly.
If both sides are comfortable, the next question is not how many grafts can be sold. It is whether the plan protects the donor area and answers the permanent hair loss pattern. IBD does not remove the need for careful graft planning. It adds extra respect for the medical history.
Wanting more hair is not enough to make someone a good candidate for a hair transplant. The body should be medically ready, the donor area should be safe, and the problem should be the kind that surgery can improve.
If your Crohn disease or ulcerative colitis is stable, your tests are acceptable, your medicines are understood, and the hair loss pattern is clear, hair transplant surgery may be reasonable. If the disease is active or the hair loss is still changing after a flare, waiting is not a failure. It protects your health, your donor area, and the quality of the final result.