Vitiligo Before FUE Needs Stable Skin
A hair transplant can be possible with vitiligo, but I do not treat it as a routine case. Before planning grafts, I check stability, new patches after cuts or scratches, and whether the donor and recipient areas are quiet. If vitiligo is active or the skin reacts strongly to trauma, waiting is safer than rushing into surgery.
The operation does not treat vitiligo itself. It treats hair loss. That distinction matters because a clinic may be able to move hair safely, but it cannot promise that pigment will behave perfectly after thousands of tiny surgical injuries.
Vitiligo changes the hair transplant decision
Vitiligo changes the discussion because the skin is not only a surface where grafts are placed. It is part of the medical environment where healing happens. In a normal hair transplant consultation, I assess donor strength, hair loss pattern, hairline position, density goals, and future loss. With vitiligo, I also ask how the skin has behaved after injury.
Follicles can often grow in someone who has vitiligo. The more serious issue is whether the skin condition is stable enough for surgery and whether the result will still look natural if the skin or hair color changes later.
I also separate vitiligo from the cause of hair loss. You can have vitiligo and still be losing hair from male pattern baldness, female pattern thinning, traction, medication changes, or another cause. Surgery only makes sense when the diagnosis of the hair loss is clear. If the hair loss itself is unstable or autoimmune, the risk discussion becomes very different, especially when you are comparing vitiligo with a broader autoimmune disease hair transplant concern.
Surgery can be considered with vitiligo only after stability checks
Surgery becomes easier to consider when the vitiligo has been stable for a meaningful period, no new patches have appeared after minor skin injuries, and the scalp does not show active irritation, inflammation, infection, or unexplained shedding. A stable small patch on the body is a very different situation from rapidly spreading scalp or hairline involvement.
Possible does not mean automatic. The donor area still has to be strong enough. The hairline still has to be age appropriate. The plan still has to protect future donor capacity. Vitiligo does not remove the usual rules of good surgery.
If you are otherwise a good candidate for a hair transplant, vitiligo becomes one more medical factor to evaluate, not an automatic rejection. But if the basic hair transplant plan is already weak because of unstable hair loss, unrealistic density goals, poor donor area, or rushed clinic planning, vitiligo makes the decision more cautious.
Vitiligo stability before surgery
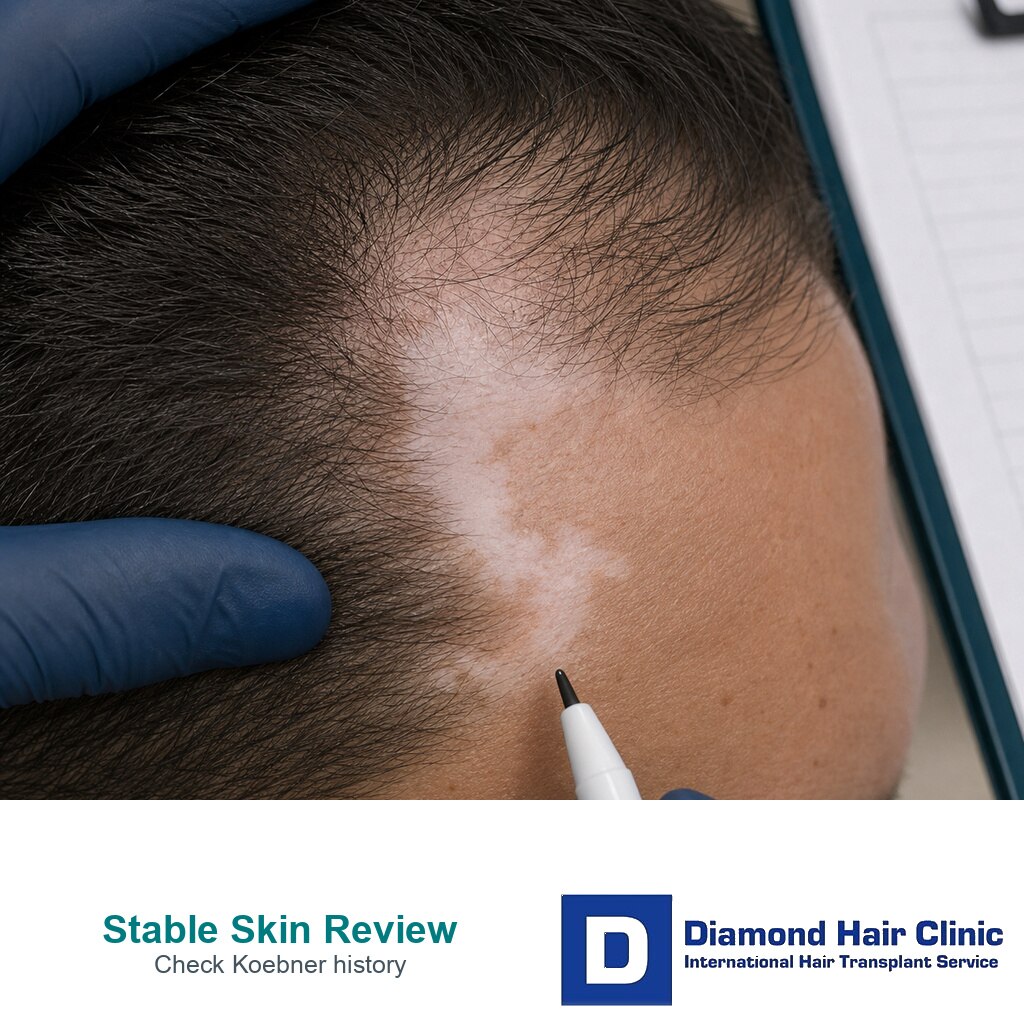
For an elective hair transplant, a quiet period is safer than a hopeful guess. That often means at least 6 to 12 months without clear spreading, new patches, active borders, or pigment change after scratches, shaving irritation, burns, or previous procedures. If the scalp itself has been involved, or if there is a strong Koebner history, the case needs more caution and often dermatologist input.
Stability is not only a date on the calendar. I look at how the skin has behaved, whether treatment has recently changed, whether the dermatologist considers the disease controlled, and whether older photos match the story. A patch that has been unchanged for years is very different from vitiligo that looks quiet today but was spreading a few weeks ago.
A fast, fixed answer from photographs alone is not enough. Pigment alone also does not prove stability. Itching, redness, active borders, recent treatment changes, or fresh scalp involvement all change how safe the timing feels. The timing decision should protect the scalp, the donor area, and your recovery.
Signs that mean surgery should wait
I advise waiting if the vitiligo is actively spreading, if new patches have appeared recently, if the scalp has fresh depigmented areas, or if you clearly develop pigment loss after cuts, scratches, friction, burns, or previous procedures. Surgery creates controlled trauma. If the skin is already reacting unpredictably, the timing is not ideal.
I also pause if you are using or changing systemic treatments for vitiligo and the dermatologist has not confirmed that the disease is stable enough for an elective procedure. Hair transplantation is not urgent medical treatment. If waiting a few months gives a clearer picture of the skin, that delay can protect you from a poor decision.
Another reason to wait is anxiety that is stronger than the medical facts. If every red spot or white mark already feels like failure, the early healing period can become very difficult. Surgery should begin with clear expectations, not panic.

Koebner history matters for surgical planning
Koebner phenomenon means that a skin condition can appear in an area after trauma. In vitiligo, this may mean depigmentation after a cut, scratch, burn, pressure mark, or surgical injury. Not every person with vitiligo has this response, and not every injury creates a new patch, but the pattern matters.

A hair transplant involves many small incisions in the recipient area and many extraction points in the donor area. These are controlled injuries, but they are still injuries. If you have already seen vitiligo appear along scars or scratches, I treat that as a serious warning in the planning conversation.
This does not mean every person with a Koebner history can never have surgery. It means the decision needs more caution. I may want dermatology input, longer stability, a smaller plan, or no surgery at that time. A clinic that ignores this history and only talks about graft numbers is not evaluating the real risk.
Dermatologist involvement before surgery
If the vitiligo is mild, stable, and far from the scalp, a dermatologist may already have given enough background information. If the disease is active, treatment is changing, or there is a strong Koebner history, the dermatologist needs to be part of the timing decision. That does not make the case impossible. It makes the plan more responsible.
Vitiligo medication should not be stopped or changed alone because surgery is being planned. Some medicines affect inflammation, healing, infection risk, sun sensitivity, or general medical safety. The surgical plan should fit the medical plan rather than compete with it.
A short delay can sometimes give a much better answer. If new patches stop appearing, the scalp stays quiet, and the dermatologist is comfortable with elective surgery, the conversation becomes more practical. If the disease continues to move, surgery may still be possible later, but the timing is wrong.
White donor hair or depigmented skin can change the plan
White hair in the donor area does not necessarily make surgery impossible. Hair color, hair caliber, skin contrast, and density all affect how the result will look. A white or very light graft placed into a darker hairline area may blend poorly unless the whole plan is designed around that color difference.
The donor area also has to be examined for more than color. I check follicle strength, reliability of the safe donor zone, hair shaft diameter, and whether extraction marks may become more visible on depigmented skin. The donor plan should not be based on a photograph alone.
If vitiligo affects the donor area, I explain that the transplanted hair may carry the color characteristics of where it came from. If the issue is mainly depigmented skin under otherwise strong hair, the aesthetic question is different. You need a plan based on actual examination, not a simple promise that everything will blend.
Use the 10 vitiligo planning slides below to separate skin stability, injury response, donor and recipient area contrast, the real cause of hair loss, candidate rules, wait signals, useful photos, appearance goals, and the final individual review. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.