Shedding at 2.5 Months Rarely Means Graft Loss
At 2.5 months, shedding is usually a hair cycle event, not permanent graft loss. In most patients, the transplanted follicles are already anchored under the skin, the old visible shafts have shed, and the follicles are resting before new growth begins. The result can look worse before it starts to improve.
Later hair fall needs a different reading. I do not judge month 6 to 8 shedding after FUE the same way as early shaft shedding, because the timeline and possible causes are different.
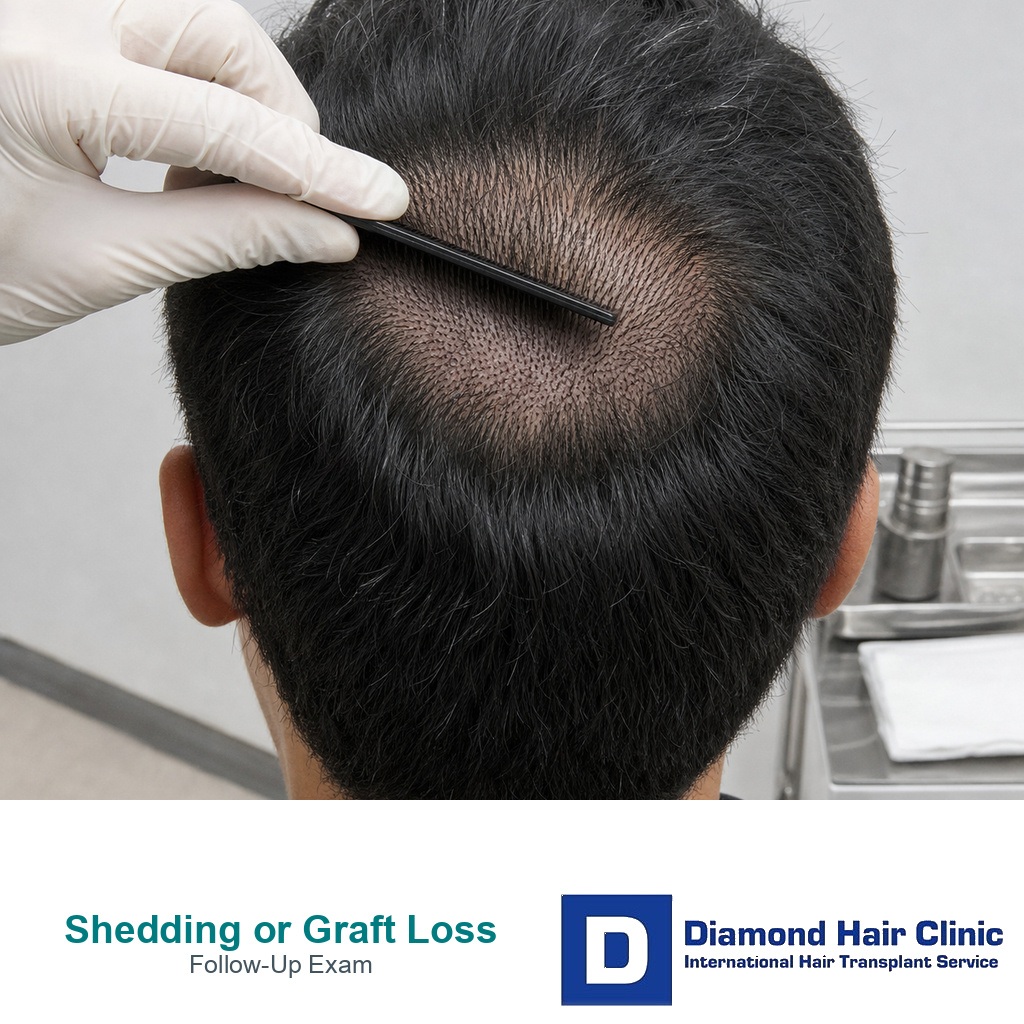
Bleeding, an open wound, discharge, spreading redness, or repeated loss from one spot changes the concern level. A thick cluster after combing may still be only shed hair shafts, but tissue like material, increasing pain, pus, or a history of trauma deserves clear photo review and, when needed, an examination.
I wrote this page because the second and third month create a very specific kind of worry. Some patients are seeing normal transplanted hair shedding. Some are seeing native hair shock loss. Some are seeing the early visual weakness of a poor plan. I separate these possibilities carefully, because the same answer does not fit every photo or every timeline.
How should you read shedding at 2.5 months?
If the scalp is settled and there is no fresh bleeding, a hair or small hair cluster falling out at 2.5 months is more likely to be shedding than a permanently lost graft. The follicle that produces the future hair is usually deeper in the skin than the visible shaft the patient sees.
True graft dislodgement is mainly an early risk. It is most concerning in the first days after surgery, before hair transplant grafts become secure enough for ordinary light contact. Later, what patients call a lost graft is often a dry hair shaft, a crust, or a piece of shedding hair that looks more dramatic than it is.
That early healing difference is explained in lost grafts after scabs come off.
Why can the transplant look worse around month two or three?
The second and third month can be emotionally difficult because the transplanted hairs may have shed while the new cycle has not yet produced visible density. This creates an empty looking period. Patients compare the scalp with the first week after surgery and feel that the result has disappeared.
This stage does not mean the surgery has failed. The follicles can be alive under the skin while the visible hair shaft is gone. New growth often begins around month 3 or month 4, but it may be thin, uneven, and slow at first.
Early growth cannot be judged like a final result. That same timing issue appears in low density 4 months after hair transplant.
Normal shedding after a hair transplant
Normal shedding means the old hair shaft falls while the follicle remains in place. It often starts within the first few weeks after surgery, but the timing varies. Some patients shed early. Some shed later. Some shed very little and keep more temporary hair for longer.
The shed hair may look like a single hair, several hairs together, or a hair attached to a small dry crust. This can be frightening, especially when the graft originally contained 2, 3, or 4 hairs.
The skin afterward matters more than the loose hair itself. Without fresh bleeding, an open hole, increasing pain, or spreading inflammation, the situation is usually less serious than it feels.
Can several hairs in one shed piece still be shedding?
A shed piece with several hairs can look frightening because many transplanted grafts naturally contain more than one hair. Patients often see 2, 3, or 4 hairs together and immediately think the whole graft has come out.
Sometimes several shafts are stuck together with dry skin, product residue, or a small crust. Sometimes the hairs came from the same follicular unit. Sometimes nearby shed hairs collected together during washing or combing.
The key question is still the skin response. A fresh graft loss is more suspicious when there is bleeding from the spot, a new wound, or a missing point in the scalp. A dry hair cluster without bleeding is less concerning, but it is still worth documenting when it worries the patient.
What does a lost graft look like in early healing?
A truly dislodged graft early after surgery often looks like more than a loose hair. It may appear as a small soft tissue piece and may be associated with bleeding from the recipient area. This is different from a dry shaft with a small bulb or crust attached.
Patients often use the word root for anything seen at the end of a shed hair. That can be misleading. The visible bulb like part does not necessarily mean the living follicle has been pulled out.
By 2.5 months, the living structure is usually not sitting loosely at the surface. I do not diagnose graft loss from one shed hair photo unless the surrounding scalp also supports that concern.
Native hair shock loss can mimic graft loss
Native hair shock loss is shedding of the patient’s original hair after surgery. It can happen around the recipient area and sometimes around the donor area. It is more common when the native hair is already miniaturized and weak.
This can make the patient think that the transplant has failed, because the whole area may look thinner than before surgery. In reality, some of the missing density may be temporary shedding of native hair, not loss of transplanted grafts.
This distinction matters for judging the result, especially when reviewing native hair shock loss after hair transplant.
When is graft loss after 2.5 months more concerning?
It is uncommon, but I do not say it is impossible. A real problem may occur if there was infection, severe scratching, trauma, poor healing, necrosis, aggressive combing over an inflamed area, or poor graft placement during the operation.
A true lost graft is more concerning when it comes with fresh bleeding, an open wound, tissue like material, repeated loss from the same exact area, or a visible gap that does not begin to improve over time. One shed cluster alone is not enough to diagnose permanent loss.
Photo review is useful at this stage. An in person examination is stronger when the patient has pain, discharge, spreading redness, persistent crusting, or a scalp area that looks unsettled or wounded.
Which photos make a shedding concern easier to judge?
Take one clear photo of the shed material on a plain background, one photo of the exact scalp area it came from, one photo of the same area under strong light, and a donor area photo if harvesting is part of the concern. The photos need to be sharp and taken without filters.
The clinic also needs the surgery date, graft number, method used, washing routine, medication list, any trauma, whether there was bleeding, and whether the scalp has pain or discharge.
A surgeon cannot responsibly judge every shedding concern from one close photo of a hair cluster. Context matters.
How should you wash and comb at this stage?
By 2.5 months, normal gentle washing is usually allowed, but aggressive scratching, scraping, or testing the grafts can irritate the scalp. If the scalp feels irritated, slow down and use mild products rather than repeatedly checking the same area.
Comb gently. If hair comes away during combing, do not keep pulling to see if more will come out. That creates anxiety and can irritate the scalp. Take a photo once, clean the scalp gently, and send the information to the clinic if needed.
When persistent crusting, itching, pimples, or soreness is present, the issue may be inflammation rather than graft loss. The right response is skin review and aftercare adjustment, not panic.
Which warning signs need prompt review?
Shedding needs prompt review when it is associated with fresh bleeding, increasing pain, heat, swelling, yellow or green discharge, bad smell, fever, expanding redness, or an area that looks wounded rather than normally healing.
Review is also important after trauma to the recipient area, aggressive scratching, forceful scab removal, strong chemicals, or thick painful crusting. If discharge, bad smell, heat, fever, or spreading redness is present, the question is no longer only shedding. The scalp needs review for an infected hair transplant.
If the scalp looks settled and the only finding is hair shedding, the next step is usually reassurance, timeline education, and follow up rather than emergency repair planning.
Clinic quality still affects final graft survival
Normal shedding is not a sign of poor surgery, but poor surgery can still reduce graft survival. The difference is important.
Graft survival can be harmed by rough extraction, graft dehydration, long time outside the body, crushing during implantation, poor recipient area angle, excessive density, weak hygiene, or a clinic model where critical steps are delegated without real surgeon responsibility.
Do not judge the result only by the name of the method. DHI, FUE, and Sapphire FUE all depend on execution. The broader warning signs are covered in Turkish hair transplant clinic red flags.
Poor placement may show later, not during the shedding phase
Poor placement can affect the final result, but it usually cannot be confirmed at 2.5 months from shedding alone. If grafts were placed at poor depth, wrong angle, excessive density, or with too much trauma, the result may later show weak growth or unnatural direction.
This is different from normal shedding. Normal shedding is a temporary timeline event. Poor placement is a surgical quality issue. Patients often mix the two because both can make the scalp look empty during the early months.
The fair approach is to follow the timeline, document the scalp, and review the final growth window. If the result remains weak after the proper time has passed, then the discussion becomes graft survival, density planning, and possible repair.
Method names do not remove the shedding cycle
The method can influence trauma and early healing, but it does not remove the shedding phase. Patients can shed after FUE, Sapphire FUE, or DHI. The follicle still responds to being moved from the donor area to the recipient area.
Technique matters because it affects graft handling, incision quality, density, and tissue trauma. A method name cannot skip the normal hair cycle.
Hair transplantation gives a broader explanation of how the procedure works, and donor area explains why extraction planning remains central.
Medication can protect native hair, not erase the cycle
Finasteride and dutasteride can help protect miniaturized native hair in suitable male patients, but they are not a guarantee that transplanted hairs will never shed. Their main value is usually long term stabilization of androgen related hair loss.
Some patients benefit from medical treatment before and after surgery. Others may not be suitable because of side effects, medical history, fertility concerns, hormone sensitivity, or personal preference. Medication decisions belong to an individual consultation.
The articles on hair transplant without finasteride and dutasteride versus finasteride after hair transplant explain this decision with more nuance.
New medication belongs in diagnosis, not panic
Do not start or change medication only because one shed cluster looks frightening. Medication decisions need diagnosis, ongoing hair loss assessment, miniaturization review, side effect discussion, and a long term plan.
If male pattern hair loss is progressing behind the transplant, medication may be important for native hair protection. But it is not an emergency reaction to one shed hair cluster.
Changing treatment out of panic can create confusion. If a medication causes side effects or shedding changes later, it becomes harder to know what is recovery and what is a treatment effect.
PRP is support, not a way to stop shedding completely
PRP may be useful as a supportive treatment in selected cases, but it is not a way to completely prevent shedding. A transplanted follicle can still enter a resting phase even when supportive treatments are used.
When PRP is used sensibly, I see it as support, not a replacement for surgical planning, graft handling, donor management, and aftercare. It also cannot repair a poor transplant plan after the fact.
PRP treatment has a place in selected cases, but the expectations need to stay modest.
Graft number affects planning and survival risk
Graft number matters because larger sessions place more demand on planning, time, staff coordination, and recipient area blood supply. A high graft number is not necessarily dangerous, but it must be supported by the donor area and the scalp.
For some patients, a large first session can be useful. For others, a smaller, more cautious plan is safer. The risk appears when the graft number is chosen for marketing rather than biology.
The safe number depends on hair loss pattern, donor density, area size, hair type, and long term planning, especially when judging how a surgeon calculates graft number.
These 10 shedding review slides separate normal month two or three shedding, scalp warning signs, hair clusters, same spot patterns, trauma history, shock loss confusion, early density judgment, and what evidence to send. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.