



Scalp Micropigmentation Changes Transplant Planning
Many patients can still have a hair transplant after scalp micropigmentation, but SMP should be assessed before surgery is planned. Pigment in the scalp does not create donor hair, and by itself it does not stop transplanted grafts from growing. The key question is whether the SMP hairline, pigment density, scalp condition, and donor area still allow a natural surgical plan.
Previous SMP does not give one fixed answer. I first look at how low the pigment hairline sits, whether the dots are too dark or blurred, whether the scalp is healthy, and whether the patient has enough donor capacity to create real coverage over the visual pattern already placed on the scalp.
If you are in this situation, bring clear photos from before SMP, after SMP, and your current hair length. Those photos help separate the real hair pattern from the pigment pattern. Without that separation, it is easy to plan surgery around the illusion instead of the scalp that actually needs treatment.
Timing depends on healing, pigment stability, and skin reaction
If the SMP is old and fully healed, timing is usually less important than the quality of the pigment design and the health of the scalp. If the SMP was done recently, I treat it like other tattoo work around hair transplant surgery. I would not plan recipient area incisions through skin that is still red, tender, crusted, itchy, or reacting to pigment.
As a practical minimum, I usually want the SMP to be fully settled for several weeks, and many patients are better assessed after about 4 to 6 weeks if the skin is calm. That is not a universal permission to operate. It is only the earliest point where the scalp may be easier to judge in selected cases.
If laser removal has been used to soften or remove SMP, the timing can become longer. I want the skin color, texture, sensitivity, and healing response to settle before transplant planning. A rushed operation after pigment trauma can make both the surgical result and the pigment problem harder to control.
SMP creates camouflage, not donor hair
Scalp micropigmentation is a visual treatment. It uses tiny pigment points to reduce the contrast between scalp and hair, but it does not grow hair and it does not replace the need for real donor grafts when a patient wants actual length, texture, and movement.
In surgical planning, pigment is usually not the main obstacle. The weaker point is planning around the illusion it creates. A transplant must still respect the donor area, the future hair loss pattern, the scalp condition, and the hairline design. If those parts are ignored, surgery can look unnatural even if the grafts technically grow.
I explain SMP as camouflage, not restoration. It can be useful in the right case, but it should never be used to pretend that the donor area is stronger than it really is.
Hairline, pigment density, scalp health, and donor capacity need review
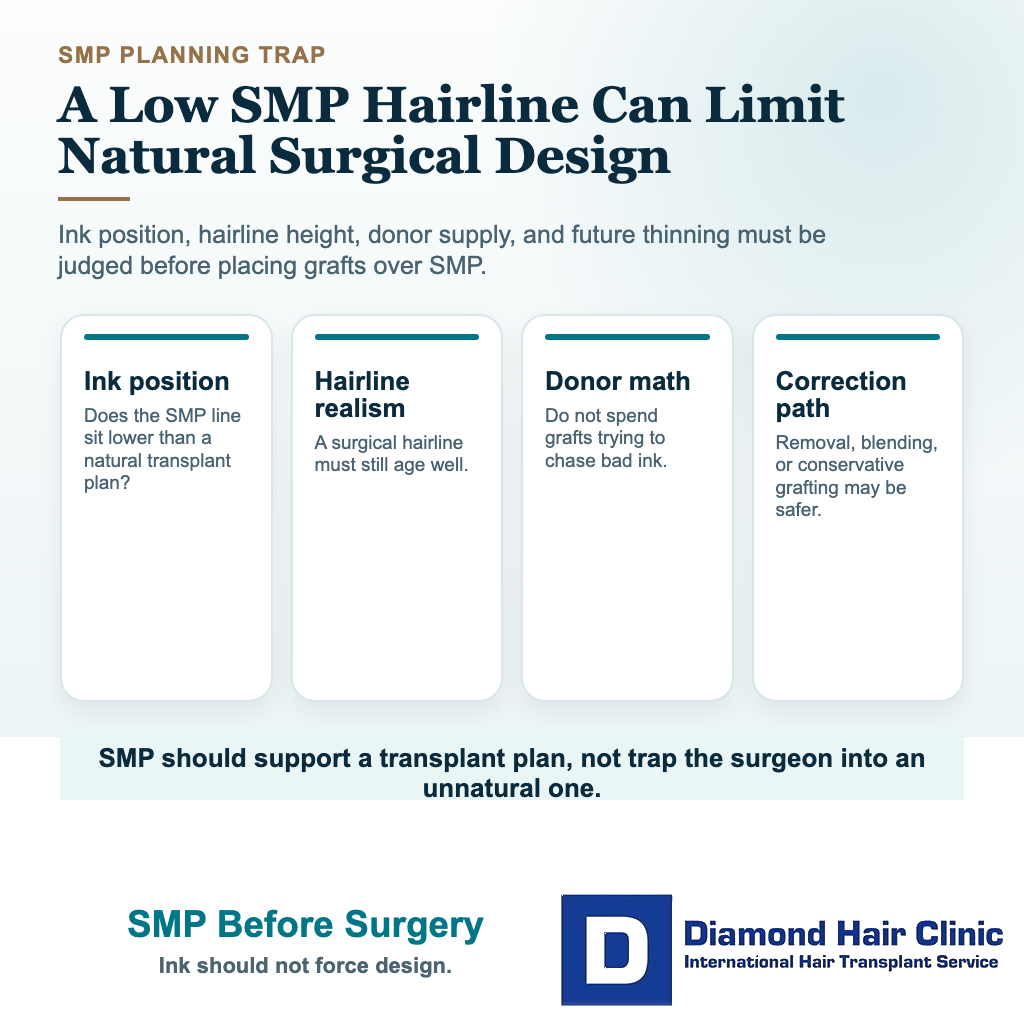
The first thing I check is whether the SMP has created a hairline that surgery can match. A pigment hairline can be drawn lower than a transplant hairline because no donor grafts are being used. That can look acceptable when the scalp is shaved very short, but it may become a problem if the patient later asks for real hair in the same place.
Real hair has direction, caliber, spacing, and softness. A natural surgical hairline needs single grafts, irregularity, and the right angle. If the SMP is too low, too straight, too dense, or too dark, the surgeon may be forced to choose between chasing an artificial pigment line or explaining that the pigment line should not be copied.
The scalp itself also has to be healthy enough for surgery. Redness, irritation, heavy scarring, inflammation, or poorly healed pigment work can change the timing. A hair transplant should not be planned over skin that is not ready for precise incisions and stable healing.
There is a difference between old, stable SMP and freshly treated skin. Recipient area incisions should not be made through scalp that is still red, crusted, tender, infected, or reacting to pigment. The pigment should be healed and stable enough that I can judge the real skin, not the short term irritation from the SMP session.
SMP makes planning harder when it hides the real hair loss pattern
SMP makes planning harder when it hides the true pattern of hair loss. If the scalp is very dark with pigment, it can be harder for the patient to understand how much real hair is missing. A surgeon can still examine the scalp closely, but the patient may expect a density that the donor area cannot supply.
The most difficult cases are usually advanced hair loss with a strong SMP outline. A patient may feel that the pigment has already given him a framed hairline, then expect surgery to fill everything behind it. In reality, the graft number may not be enough to recreate a full scalp of hair, especially when the crown is also involved.
That is where weak donor area planning becomes important. The donor area is not an unlimited bank. If surgery uses too many grafts trying to match a cosmetic pigment design, the patient may lose the chance to manage future thinning more intelligently.
Removal is not always needed, but some pigment needs softening
If the SMP is light, natural, well placed, and the planned transplant will sit comfortably within the same area, removal may not be necessary. In some patients, the pigment can even reduce the appearance of scalp contrast after the transplanted hair grows.
But removal may need to be discussed when the SMP is too low, too blue, too dense, blurred, patchy, or placed in an area that surgery should not follow. It is better to correct the plan before surgery than place grafts into a design that will age badly.
Laser removal is not a small cosmetic detail. It can require time, repeated sessions, and careful skin healing before surgery is reconsidered. If the pigment is only mildly imperfect, I may design the transplant around it. If the pigment creates an obviously wrong hairline, ignoring it can make the final result harder to repair.
Softening pigment is different from trying to erase it in a hurry. If laser is needed, I want the last treatment to settle before I judge the skin, the remaining color, and the surgical hairline. A scalp that is still irritated from removal is not the right foundation for precise recipient area work.
SMP can improve contrast, but it cannot create hair texture
SMP can sometimes make a thin result look fuller, but only when the hair length, skin color, hair color, and density are suitable. It works best as background shadow. It does not change hair caliber, it does not add texture, and it does not make long sparse hair behave like dense hair.
These are two different decisions. A patient asking about scalp micropigmentation for a thin transplant is usually trying to improve an existing result. A patient asking about hair transplant after SMP is asking whether earlier pigment will limit a future surgical plan.
The order matters. If SMP is done after surgery, it can be adjusted to the real hair that grew. If SMP is done first, the transplant may need to respect a visual pattern that was created before donor capacity, hairline design, and future loss were fully understood.
SMP chosen before surgery needs conservative future planning
That is a common situation, especially in younger patients or men with advanced thinning who are not ready for surgery, medication, or a large financial commitment. SMP can give a cleaner shaved look while the patient waits, but it needs planning conservatively if surgery may be wanted later.
A young patient with a low, sharp SMP hairline and active hair loss needs extra caution in planning. The pigment can feel satisfying at first, but it may make a future transplant more difficult because the surgery has to respect age, donor reserve, and long term balance.
If hair loss is still active, I also discuss whether a patient is medically and emotionally ready for surgery at all. Some patients need time, follow up, and medical stabilization before transplantation becomes a better decision. That is especially important in cases similar to diffuse thinning hair transplant planning, where placing grafts between weak native hairs can carry extra risk.
Donor capacity decides how far surgery can go
Donor capacity is the part many patients underestimate. SMP can cover a large bald area visually, but a hair transplant has to move real follicular units from a limited donor supply. The bigger the area, the more carefully the grafts must be used.
I also look separately at SMP in the recipient area and SMP in the donor area. Pigment in a thin or scarred donor can make the back of the scalp look stronger than it truly is, especially in photos. Before I plan any extraction, I need to examine the donor hair itself, not the photo darkened by pigment, to see whether SMP is hiding low density, FUE marks, or previous overharvesting.
If a patient has a strong donor area and a realistic SMP design, surgery may be very reasonable. If the donor area is weak, already overused, or too fine for the size of the bald area, a transplant may only create partial coverage. In that case, the patient must understand the limit before committing.
This is also where medication discussions may affect the plan. Some patients can have surgery without medication, but progressive native hair loss changes the long term picture. The logic is similar to the decision behind having a hair transplant without finasteride, where the transplanted hair and the remaining native hair must be judged separately.
Low SMP hairline can create a problem over time
Conservative planning matters here. A pigment hairline can be placed quickly, but a transplanted hairline has to look natural from close distance, in movement, in different lighting, and as the patient ages.
If the SMP hairline is too low, a surgeon may not want to copy it with grafts. Copying it could use too many grafts in the front, weaken future options, and create a hairline that does not fit the patient later. Refusing to copy it may leave visible pigment below the surgical hairline.
Good hairline design in hair transplant surgery is not just drawing a nice shape. It is deciding what will still look natural when the patient is older, when native hair changes, and when the donor area may need to be used again.
SMP, surgery, or both should be chosen by the goal
The best choice depends on what you want your hair to do. If you are happy with a shaved look and want lower surgical risk, SMP may be enough. If you want hair that grows, can be styled, and creates real texture, SMP alone cannot provide that.
If you want both, the order needs planning carefully. Surgery first often gives the clearest foundation because the real graft result can be assessed before pigment is added. SMP first can still be workable, but it should stay soft, natural, and conservative if future surgery is a possibility.
A patient using a hair system after a hair transplant has a different set of decisions, but the principle is similar. Any cosmetic cover should not hide the medical reality. The scalp, donor area, hairline, and future hair loss pattern still decide what is safe.
Surgery after SMP is weak when expectations exceed donor supply
Surgery after SMP becomes a poor plan when the pigment has created expectations that the donor area cannot meet. If the patient expects full coverage from a limited donor supply, a transplant may create disappointment rather than relief.
I am also cautious if the patient already has poor donor density, an overharvested donor area, unstable hair loss, heavy scarring, or a very dark SMP design that does not match the intended surgical hairline. In those cases, the operation may be technically possible but strategically weak.
Sometimes the wiser step is not immediate surgery. It may be to wait, reassess the donor area, review old photos, check whether the SMP can be softened, and decide whether the patient is trying to solve a surgical problem or an expectation problem. That same judgment is central in bad hair transplant repair, where acting too quickly can make a difficult situation worse.
Plan the next step from the real scalp, not the pigment illusion
When SMP is already present and you are considering a hair transplant, do not start by asking only whether surgery is possible. Start by asking whether surgery can create a natural result without chasing an artificial pigment pattern.
I examine the SMP in normal light, harsh light, and close distance. I check whether the hairline is too low, whether the color has changed, whether the pigment has spread, whether the scalp is healthy, and whether there is enough donor hair to create the result the patient expects.
Then I decide whether the best plan is surgery, surgery later, SMP adjustment, pigment removal, medical stabilization, or no surgery. That sequence is surgical judgment, because the wrong plan can consume grafts that cannot be replaced.
When a patient has both SMP and limited donor capacity, I think in terms of long term appearance rather than short term coverage. The same principle applies to overharvested donor area repair and to whether a result will still feel natural years later.
The better decision is the one that keeps your future options open. SMP does not by itself close the door to a hair transplant, but an aggressive SMP design can make the next door narrower. If the pigment is conservative, the scalp is healthy, and the donor plan is clear and realistic, a hair transplant after scalp micropigmentation can be reasonable.
The plan should never be built around hiding a problem from the patient. It should make the limits clear, protect the donor area, and create a result that can still make sense as the patient ages. That is the same long term thinking behind a hair transplant that still looks natural as you get older.